Download as pdf or txt
You might also like
- 8 Point AgendaDocument13 pages8 Point AgendaRoel AbricaNo ratings yet
- FAQs For Health FacilitiesDocument17 pagesFAQs For Health FacilitiesPhilhealth ISDH SinaitNo ratings yet
- Powerchart Review Guide v2 1rpDocument6 pagesPowerchart Review Guide v2 1rpapi-224958119No ratings yet
- AMBULATORY SURGICAL CLINICwpsDocument3 pagesAMBULATORY SURGICAL CLINICwpsJose Bernel100% (3)
- PMA Member Registration FormDocument1 pagePMA Member Registration Formmaria angela Saldajeno100% (1)
- Ateneo de Davao Memorandum of AgreementDocument3 pagesAteneo de Davao Memorandum of AgreementluismisaNo ratings yet
- An Analysis of A Film Gifted HandsDocument9 pagesAn Analysis of A Film Gifted Handscitra indah syaputri100% (1)
- ET Suctioning Check ListDocument2 pagesET Suctioning Check ListAnjali Rahul Ajmeri100% (1)
- Directory of Doctors - KenyaDocument18 pagesDirectory of Doctors - KenyaKush GuptaNo ratings yet
- DOH DM 2019 0062 HepB Demo Project With Interim GuidelinesDocument31 pagesDOH DM 2019 0062 HepB Demo Project With Interim GuidelinesRold Brio SosNo ratings yet
- Human Resource For Health (HRH) Evaluation 2020: Rural Health Unit Staff Behavioral RatingDocument17 pagesHuman Resource For Health (HRH) Evaluation 2020: Rural Health Unit Staff Behavioral RatingSeriel Tismo100% (1)
- Rev Manual DCF & Cert Page For Muns & CCs - PY 2018 - 2018 ProjPop - Updated 011619Document12 pagesRev Manual DCF & Cert Page For Muns & CCs - PY 2018 - 2018 ProjPop - Updated 011619Sheena SilorioNo ratings yet
- (Simpo 2 Dr. Sally) - Sindrom MetabolikDocument57 pages(Simpo 2 Dr. Sally) - Sindrom MetabolikYosefin RatnaningtyasNo ratings yet
- Diagnostic Approach of Short Stature / Stunted (Jan 2015) - Prof DR Jose BatubaraDocument49 pagesDiagnostic Approach of Short Stature / Stunted (Jan 2015) - Prof DR Jose BatubaraGerakan Kesehatan Ibu dan AnakNo ratings yet
- DOH-HFSRB-QOP01Form1 Rev2 6172022Document3 pagesDOH-HFSRB-QOP01Form1 Rev2 6172022clarisse salvadorNo ratings yet
- DOH-HFSRB-QOP-01-Form 2 A: Print Name and SignatureDocument1 pageDOH-HFSRB-QOP-01-Form 2 A: Print Name and SignatureJm CayabyabNo ratings yet
- Health Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthDocument1 pageHealth Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthPANACEE DIAGNOSTIC CENTERNo ratings yet
- DOH Dialysis AO 2013-0003Document4 pagesDOH Dialysis AO 2013-0003al gul100% (1)
- Dialysis Application For LTO Rev1 1232014Form-HDC-LTO-A-2007Document12 pagesDialysis Application For LTO Rev1 1232014Form-HDC-LTO-A-2007al gulNo ratings yet
- Gonzales Zosimo AbstractDocument2 pagesGonzales Zosimo AbstractDarnel Jasper HurtadoNo ratings yet
- PD996 Compulsory ImzDocument2 pagesPD996 Compulsory Imzapi-19824701No ratings yet
- Administrative Order 2010-0034Document15 pagesAdministrative Order 2010-0034Esperanza Evaristo-ReyesNo ratings yet
- Performance Commitment For ProfessionalsDocument3 pagesPerformance Commitment For ProfessionalsCecille Cabrera100% (2)
- AO2021-0066 Guidelines On The Issuance of Certificate On Inclusion (COI) in The Blood Services Network (BSN)Document17 pagesAO2021-0066 Guidelines On The Issuance of Certificate On Inclusion (COI) in The Blood Services Network (BSN)gravadorceciliaNo ratings yet
- PMRA ICD Invitation For November 2021Document1 pagePMRA ICD Invitation For November 2021Jam AicaNo ratings yet
- Moh New Requirements For Foreign Workers ContractDocument3 pagesMoh New Requirements For Foreign Workers ContractaikalessNo ratings yet
- Issuance of Dangerous Drugs License (S2-License, Practitioner)Document4 pagesIssuance of Dangerous Drugs License (S2-License, Practitioner)Josselle Sempio CalientaNo ratings yet
- REDCOP Updates (Reg.v)Document36 pagesREDCOP Updates (Reg.v)DaNiel AUreusNo ratings yet
- Biggest Loser RegistrationDocument2 pagesBiggest Loser RegistrationDawn BrennanNo ratings yet
- Oral Health SOPDocument14 pagesOral Health SOPZita AprilliaNo ratings yet
- DOH ICT SytemDocument19 pagesDOH ICT Sytemricohizon99No ratings yet
- DOH MLGP and SCM Executive CourseDocument42 pagesDOH MLGP and SCM Executive CourseHarnikka ConstantinoNo ratings yet
- Application Form Blood Collection Unit Blood StationDocument5 pagesApplication Form Blood Collection Unit Blood StationRhodora BenipayoNo ratings yet
- DOH AO 2021-0056 Revised IRR For The Sanitation Code Chapter 21Document55 pagesDOH AO 2021-0056 Revised IRR For The Sanitation Code Chapter 21Clarice ANo ratings yet
- Dialysis Licensing Requirment DC - LTO-LR12192006 PDFDocument5 pagesDialysis Licensing Requirment DC - LTO-LR12192006 PDFal gulNo ratings yet
- 2024 04 16 ADVISORY HRDU Process and Requirements For New and Renewal Applications For The Provisional Certification of PCWDocument6 pages2024 04 16 ADVISORY HRDU Process and Requirements For New and Renewal Applications For The Provisional Certification of PCWjefferson bustarga100% (1)
- Kilatis KutisDocument7 pagesKilatis KutisBorbe Clau100% (1)
- Additional Guidance On COVID-19 Vaccine Storage, Handling and DistributionDocument2 pagesAdditional Guidance On COVID-19 Vaccine Storage, Handling and DistributiondavebarceNo ratings yet
- 2238 PDFDocument4 pages2238 PDFIvy Glady Alcantara GarciaNo ratings yet
- PRC Forms Bicol University COllege of Nursing, Legazpi CityDocument5 pagesPRC Forms Bicol University COllege of Nursing, Legazpi CityekagaliasNo ratings yet
- Attendance Sheet For PRC CPD ActivityDocument2 pagesAttendance Sheet For PRC CPD ActivityFitz Jaminit100% (1)
- Annex B Konsulta ChecklistDocument8 pagesAnnex B Konsulta ChecklistFret Ramirez Coronia RNNo ratings yet
- 2019 Hfep Liph As of July 24, 2019Document49 pages2019 Hfep Liph As of July 24, 2019joey salagantinNo ratings yet
- Acute Flacid Paralysis ApproachDocument54 pagesAcute Flacid Paralysis Approacheman khammas100% (1)
- SPONSORSHIP LETTER Medical Mission EventDocument2 pagesSPONSORSHIP LETTER Medical Mission EventLexee DayanghirangNo ratings yet
- CPM Benign Prostatic HyperplasiaDocument7 pagesCPM Benign Prostatic HyperplasiaVon BellosilloNo ratings yet
- Dengue FormDocument2 pagesDengue FormZurc Saquin ApepeNo ratings yet
- RA 7164 Nursing Act of 1991Document8 pagesRA 7164 Nursing Act of 1991Filipino Nurses CentralNo ratings yet
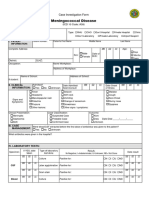
- Case Investigation Form - Meningococcal DiseaseDocument2 pagesCase Investigation Form - Meningococcal Diseaseclaverialc10No ratings yet
- Importance in Following Health Protocols and Saving Lives Against Covid 19Document1 pageImportance in Following Health Protocols and Saving Lives Against Covid 19Marianne MagistradoNo ratings yet
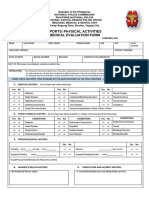
- Pre Medical Evaluatiom Form PFT 1 PDFDocument2 pagesPre Medical Evaluatiom Form PFT 1 PDFAIEN WENDELEIH Q. CAPINPIN100% (2)
- Sample Three: Physician and Hospital ContractDocument12 pagesSample Three: Physician and Hospital ContractMario Lopez100% (1)
- Memorandum of Agreement: LIFE - CARE MEDICAL AND DIAGNOSTIC CENTER, A Business Establishment Duly Presenting andDocument5 pagesMemorandum of Agreement: LIFE - CARE MEDICAL AND DIAGNOSTIC CENTER, A Business Establishment Duly Presenting andMarialynNo ratings yet
- Regional Trial Court Branch 226, Quezon CityDocument27 pagesRegional Trial Court Branch 226, Quezon CityCharissa Magistrado De LeonNo ratings yet
- Citizen's Charter - Filing For Walk in ClientsDocument2 pagesCitizen's Charter - Filing For Walk in ClientsJeffreyReyesNo ratings yet
- Self Monitoring Report System 2ND Quarter 2018Document9 pagesSelf Monitoring Report System 2ND Quarter 2018ARCHEMEDEZ RAMOSNo ratings yet
- Department of Pediatrics: Case ProtocolDocument11 pagesDepartment of Pediatrics: Case ProtocolKim Adarem Joy ManimtimNo ratings yet
- Memorandum of Agreement 2Document4 pagesMemorandum of Agreement 2z.fseiei01No ratings yet
- Module 1 Introduction To rHIVdaDocument49 pagesModule 1 Introduction To rHIVdaRaki Dallas100% (1)
- Maia Birthing Home: "Caring For Your Health & Wellness"Document1 pageMaia Birthing Home: "Caring For Your Health & Wellness"Imelda NatividadNo ratings yet
- Drug Action Indication Contraindicati ON Adverse Effects Nursing ConsiderationsDocument3 pagesDrug Action Indication Contraindicati ON Adverse Effects Nursing ConsiderationsRaphael PalomataNo ratings yet
- List of PPAS To Combat Acquired Immune Deficiency SyndromeDocument4 pagesList of PPAS To Combat Acquired Immune Deficiency SyndromeLeonard ArenasNo ratings yet
- PRDP 2024 Terms of ReferenceDocument4 pagesPRDP 2024 Terms of ReferencepolkadatuinNo ratings yet
- DOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1Document2 pagesDOH HFSRB QOP 01 Form1 3212019 postedDOH 1 1 1jheanniver nablo100% (1)
- DOH HFSRB QOP 01 Form1 3212019 postedDOH 1Document2 pagesDOH HFSRB QOP 01 Form1 3212019 postedDOH 1Karina Santos90% (10)
- Application Form 2019Document5 pagesApplication Form 2019Rocky MontañerNo ratings yet
- JJM Medical CollegeDocument1 pageJJM Medical CollegeRakeshKumar1987No ratings yet
- Acute Glomerulonephritis Physical Assessment Bagtas EstrelitaDocument11 pagesAcute Glomerulonephritis Physical Assessment Bagtas EstrelitamarengbibNo ratings yet
- TMSDocument2 pagesTMSrapgabrielNo ratings yet
- Maximum Recommended Doses and Duration of Local Anesthetics - Iowa Head and Neck ProtocolsDocument1 pageMaximum Recommended Doses and Duration of Local Anesthetics - Iowa Head and Neck ProtocolsFirmawati Muslim SkepNo ratings yet
- Gunderson Teppers Clinical Radiation Oncology 5Th Edition Edition Joel Tepper Full ChapterDocument67 pagesGunderson Teppers Clinical Radiation Oncology 5Th Edition Edition Joel Tepper Full Chaptersandra.glynn782100% (8)
- Ebook Abeloffs Clinical Oncology PDF Full Chapter PDFDocument67 pagesEbook Abeloffs Clinical Oncology PDF Full Chapter PDFsteven.walker989100% (37)
- ENT MCQsDocument13 pagesENT MCQsSheikha100% (2)
- Report - University of Santo Tomas HospitalDocument16 pagesReport - University of Santo Tomas HospitalMikee MeladNo ratings yet
- FAQs - DR KiranDocument15 pagesFAQs - DR KiranPradeep Reddy Anam100% (1)
- Alex Chernov CompletoDocument4 pagesAlex Chernov CompletolaparovetNo ratings yet
- Medicographia 86Document95 pagesMedicographia 86brave_ftNo ratings yet
- Two Steps Individualized ACTH Therapy For West SyndromeDocument1 pageTwo Steps Individualized ACTH Therapy For West SyndromeDrAmjad MirzanaikNo ratings yet
- 5 HD Specialists and ClinicsDocument2 pages5 HD Specialists and ClinicsRachael BrookingNo ratings yet
- Curriculum Vitae TempleteDocument4 pagesCurriculum Vitae TempletesyedNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore Annexure - Ii Proforma For Registration of Subjects For DissertationDocument10 pagesRajiv Gandhi University of Health Sciences, Karnataka, Bangalore Annexure - Ii Proforma For Registration of Subjects For DissertationAbhilash PaulNo ratings yet
- Testicular TorsionDocument5 pagesTesticular Torsionmohammed agungNo ratings yet
- Functions of The Corticospinal and Corticobulbar Tracts in The Human NewbornDocument6 pagesFunctions of The Corticospinal and Corticobulbar Tracts in The Human NewbornMas ArikNo ratings yet
- Resusitasi NeonatusDocument22 pagesResusitasi NeonatusnikkitaihsanNo ratings yet
- Essay On "Why I Am Interested in Medicine and How I Will Use It To Provide Good Health Care For The People of Indonesia in The Future"Document1 pageEssay On "Why I Am Interested in Medicine and How I Will Use It To Provide Good Health Care For The People of Indonesia in The Future"lourdes kusumadiNo ratings yet
- FTS PDFDocument2 pagesFTS PDFkukadiyaNo ratings yet
- Research TopicsDocument7 pagesResearch TopicsWillium ThomasNo ratings yet
- Clinical ExemplarDocument5 pagesClinical Exemplarapi-300362983No ratings yet
- First Admission List March23 PDFDocument387 pagesFirst Admission List March23 PDFMedic IronyNo ratings yet
- Floor Reaction OrthosisDocument45 pagesFloor Reaction OrthosisJipin Gopi100% (1)