Thrombotic Disorders Part 2
Thrombotic Disorders Part 2
Uploaded by
KAJAL SINGHCopyright:
Available Formats
Thrombotic Disorders Part 2
Thrombotic Disorders Part 2
Uploaded by
KAJAL SINGHOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Thrombotic Disorders Part 2
Thrombotic Disorders Part 2
Uploaded by
KAJAL SINGHCopyright:
Available Formats
This open-access article is distributed under
Creative Commons licence CC-BY-NC 4.0. CME
Thrombotic disorders (part 2)
N A Alli, MB BCh, FCPath (SA) Haem; J Vaughan, MB BCh, MMed (Haem), FCPath (SA) Haem; S Louw, MB BCh, MMed (Haem),
FCPath (SA) Haem; E Schapkaitz, MB BCh, MMed (Haem), FCPath (SA) Haem; B Jacobson, MB BCh, MMed (Haem), FCPath (SA) Haem, PhD
Department of Molecular Medicine and Haematology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg;
and National Health Laboratory Service, Johannesburg, South Africa
Corresponding author: N A Alli (nazeer.alli@nhls.ac.za)
Thromboembolic conditions are a leading cause of mortality, estimated to account for 1 in 4 deaths worldwide in 2010. Over time, the
incidence and mortality rates of these conditions have declined in developed countries, but are increasing in developing countries. A delicate
balance exists between procoagulant and anticoagulant factors within the vascular system. Numerous acquired or inherited conditions
may tip the balance either way, i.e. towards a prothrombotic or prohaemorrhagic state. Acquired thrombotic disorders are the subject of
discussion in this issue, the second of a 2-part series on thrombophilia.
S Afr Med J 2020;110(3):181-187. https://doi.org/10.7196/SAMJ.2020.v110i3.14634
Thrombotic disorders may be inherited, as Causes of acquired thrombophilia are listed the antiphospholipid syndrome, heparin-
discussed in part 1 (previous issue),[1] or in Table 1. induced thrombocytopenia and paroxysmal
acquired. They are the subject of discussion A more detailed discussion is given nocturnal haemoglobinuria). Thrombophilia
in this issue, the second of a 2-part series below regarding acquired risk factors associated with specific clinical scenarios
in CME. for thrombosis, as well as information mainly affecting the arterial circulation
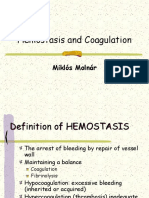
The process of coagulation involves pertaining to clinical entities characterised and microvasculature (e.g. myocardial
activation, adhesion and aggregation of by a marked predilection to thrombosis (i.e. infarction, diabetes, hypertension, thrombotic
platelets to damaged endothelium, followed
by deposition and maturation of fibrin, and
begins almost immediately after injury to Clot formation Amplification phase Initiation phase
the endothelial lining of the blood vessel.
Exposure of blood to the subendothelial
(XIIa)
area initiates two processes, viz. changes in IX VII TF
Fibrinolysis
platelets, and the exposure of subendothelial
XIII XI XIa Activated
tissue factor (TF) to plasma factor VII
platelets
(FVII). Platelets immediately form a plug -
at the site of injury, which is referred
AT -
to as primary haemostasis. Secondary IXa TF-VIIa
haemostasis occurs simultaneously where I -
- -
additional coagulation factors beyond FVII II PL
respond in a cascade to form fibrin strands, XIII VIIIa TFPI
Plg
which confer stability to the platelet plug
(Fig. 1).[2] PL
Fibrin Xa X
The TF-FVIIa complex is a crucial trigger tPA monomer Va
for haemostatic responses in vivo, and exces- -
-
sive initiation of coagulation through this
Clot
pathway can lead to thrombosis or consump Plasmin Cross-linked PT APC
dissolution fibrin
tive coagulopathy. Increased TF-FVIIa com-
plex formation can result from loss of vascu- -
PS II + TM
lar wall integrity and increased TF expression.
For example, atherosclerotic plaques contain α2AP
significant levels of TF, generally associated
PC
with monocytes/foam cells and smooth-
muscle cells.[2] TF expression can also be Fig. 1. Coagulation cascade. Dotted arrows indicate actions of natural anticoagulants and fibrinolytic
increased with malignancy, potentially leading factors. (V, VIII, IX, X, XI, XIII = procoagulant factors; suffix a = activated factor; AT = antithrombin;
to cancer-associated thrombosis.[3] During TF = tissue factor; I = fibrinogen; II = thrombin; Plg = plasminogen; PL = phospholipid (on platelet
sepsis, TF is expressed on monocytes, but is membrane); TFPI = tissue factor pathway inhibitor; tPA = tissue plasminogen activator; PT = pro
also expressed by endothelial cells in some thrombin; APC = activated protein C; PS = protein S; TM = thrombomodulin; α2AP = α2-antiplasmin;
areas, such as the splenic microvasculature.[4] PC = protein C.)
181 March 2020, Vol. 110, No. 3
CME
Table 1. Precipitating factors/conditions associated with Renal disease
thrombosis Chronic kidney disease (CKD) is an established risk factor for arterial
Antiphospholipid antibodies and venous thrombosis. The latter occurs 5.5 times more frequently in
Atrial fibrillation/congestive cardiac failure patients with CKD than in people with normal renal function.[10] The
Chronic inflammation, e.g. TB, HIV, inflammatory bowel disease hypercoagulable state in patients with CKD relates to procoagulant
Immobilisation/postoperative state factors (antiphospholipid antibodies, artificial shunts and indwelling
Malignancy/myeloproliferative disorders catheters), concomitant use of erythropoietin-stimulating agents,
Heparin-induced thrombocytopenia decline in fibrinolytic activity and decreased natural anticoagulant
Oral contraceptive use/pregnancy/oestrogen therapy levels. Anticoagulation therapy in patients with renal dysfunction can
Diabetes mellitus/obesity be challenging owing to altered drug pharmacokinetics, necessitating
Hyperviscosity dose adjustment and more intense monitoring.[10,11]
Chronic haemolysis, e.g. SCD, PNH
Iatrogenic, e.g. HIT, indwelling venous catheter
Inflammatory bowel disease
Patients with inflammatory bowel disease (IBD), the major forms
Renal disease
of which are ulcerative colitis (UC) and Crohn’s disease (CD), have
TTP
a 3-fold increased risk of developing venous and, to a lesser extent,
Trauma
arterial thrombosis. The hypercoagulability in patients with IBD is
TB = tuberculosis; SCD = sickle cell disease; PNH = paroxysmal nocturnal haemoglobinuria; multifactorial and not completely understood, but relates to chronic
HIT = heparin-induced thrombocytopenia; TTP = thrombotic thrombocytopenic
purpura. inflammation with increases in acute-phase reactants and cytokines,
hospitalisation, surgery and indwelling catheters. VTE episodes
usually correlate with disease activity, although these may occur
thrombocytopenic purpura (TTP)) are influenced by a multitude during periods of remission. There is evidence that patients with IBD
of factors and varied aetiologies. Such scenarios merit discussion experience the first episode of VTE at a younger age than the general
on discipline-specific platforms and therefore do not fall within the population, with an increased risk of recurrence, and that UC and CD
scope of this CME. The scope of this discussion is limited to clinical pose an equal thrombotic risk.[12,13]
entities associated with a marked increase in the risk of thrombosis.
We conclude with a guide to the diagnosis and further investigation Pregnancy/oral contraceptive use
of suspected thromboembolic disease. Among women, additional risk factors for VTE include combined
oral contraceptives (OCs), hormone replacement therapy, pregnancy
Acquired risk factors for thrombosis and the postpartum period.
Mycobacterium tuberculosis infection Oestrogen use increases the risk of VTE as a class effect, which is dose
The risk of venous thromboembolism (VTE) is 1.5 times higher dependent. The risk of VTE depends on the route of administration.
in patients with Mycobacterium tuberculosis (TB) infection than in There is lower associated risk with transdermal and intrauterine
uninfected individuals and relates to immobilisation, increase in hormonal therapy, as well as with progesterone-only OC use.[14]
procoagulant acute-phase reactants such as fibrinogen, decrease in The risk of VTE is increased 5 - 10-fold in pregnancy. The
the natural anticoagulants including protein C (PC) and protein S hypercoagulability of pregnancy persists for several weeks after
(PS), and mechanical compression of veins from enlarged lymph delivery, where the greatest risk for VTE is in the early postpartum
nodes.[5] Active TB infection is also frequently linked to underlying period. The recent decline in maternal deaths from VTE can be
infection with HIV, which further increases the risk of VTE.[6] attributed to the use of thromboprophylaxis in high-risk women.[15,16]
Concomitant HIV infection and VTE during TB treatment can VTE risk assessment is recommended early during pregnancy
result in clinically significant drug-drug interactions, as warfarin and in the postpartum period. Risk factors include previous VTE,
is metabolised by the cytochrome P450 (CYP450) pathway in the family history of VTE, hereditary thrombophilia, antiphospholipid
liver. Therapeutic agents that induce this pathway (e.g. rifampicin syndrome (APS), medical comorbidities, significant pregnancy
and nevirapine) or inhibit it (e.g. isoniazid and efavirenz), may complications, caesarean delivery, prolonged antepartum immobi
result in under- or over-anticoagulation, necessitating more intense lisation and clinical risk factors, such as increased body mass index
monitoring and management of anticoagulation therapy. (BMI), age >35 years and parity ≥3. High-risk patients should be
managed in conjunction with a haematologist and, in the case of APS,
HIV infection a rheumatologist. Antepartum and postpartum thromboprophylaxis
The incidence of arterial and venous thrombosis in HIV-infected with low-molecular-weight heparin (LMWH) and low-dose aspirin is
patients is increased compared with healthy controls. The patho recommended in women with APS and previous VTE. Higher doses
genesis of the hypercoagulability in people infected with HIV is of LMWH may be required.[16]
multifactorial and relates to an increase in procoagulant acute-phase The ideal anticoagulant in pregnancy does not cross the placenta
reactants (Von Willebrand factor, fibrinogen and FVIII), a decrease and can be easily reversed. The oral direct thrombin and FXa
in the level of natural anticoagulants (PC and PS), production inhibitors should not be used in pregnancy, as the molecules are
of lupus anticoagulant antibodies due to immune dysregulation small and cross the placenta. Warfarin is associated with a teratogenic
and endothelial dysfunction. Concomitant disease processes in effect, especially between 6 and 12 weeks’ gestation. Furthermore,
HIV-infected patients, including secondary malignancies, additional there is an increased risk of miscarriage, prematurity and fetal
infections, concurrent immobilisation and drugs, can also contribute bleeding (including intracranial haemorrhage resulting in brain
to the increased thrombotic risk that has been recognised in VTE damage) at any time during pregnancy. LMWH is the preferred
treatment and prophylaxis guidelines.[7-9] anticoagulant. Antepartum prophylaxis should be initiated early in
182 March 2020, Vol. 110, No. 3
CME
pregnancy. Postpartum thromboprophylaxis should be continued for Furthermore, these agents have been associated with an increased
6 weeks in high-risk women, for 10 days in intermediate-risk women risk of bleeding in patients with gastrointestinal cancers, and should
and at least until discharge from hospital in low-risk women. There is be used with caution in this group.[23] This has led the Scientific and
an increased dose requirement for LMWH during pregnancy because Standardization Committee on Haemostasis and Malignancy of
of increased volume of distribution and renal clearance. Regular anti-Xa the International Society of Thrombosis and Hemostasis (ISTH) to
monitoring is therefore recommended. recommend the use of DOACs only in patients with a low bleeding risk
who do not use agents likely to cause drug-drug interactions.[24] Cancer-
Obesity associated thrombosis should be treated for at least 3 - 6 months, and
Obesity is defined as a BMI ≥30 kg/m2. Owing to its increasing as the risk of recurrence is increased, ongoing anticoagulation should
prevalence, obesity has emerged as an important risk factor for VTE be considered while the patient has active cancer.[23]
in addition to myocardial infarction and stroke in high-income Among otherwise apparently well patients who present with
countries. In South Africa (SA), a resource-limited country, there is unprovoked thrombosis, a small proportion can be demonstrated
a bimodal distribution, with a rise in obesity, particularly in urban to be harbouring occult malignancies. Limited cancer screening
settings. Central obesity is characterised by chronic inflammation is therefore recommended by the ISTH in this group of patients,
and impaired fibrinolysis, which are the two major pathways that including a clinical evaluation, chest radiograph, full blood
contribute to VTE risk.[17] count, liver function testing, serum calcium, urinalysis and age-
As obesity is considered a moderate risk factor for VTE in high- appropriate screening tests (e.g. prostate-specific antigen level,
risk circumstances, such as hospitalised medical patients, surgery and mammography).[25] Patients who experience recurrent VTE while
immobilisation, thromboprophylaxis should be considered. Higher on anticoagulant therapy or bilateral deep-vein thrombosis are at
doses of LMWH are often required for the prevention of VTE in particularly high risk of occult cancer, and may benefit from a more
obese patients.[18] Laboratory monitoring of LMWH therapy in obese extensive work-up in the case of underlying malignancy.[20]
patients using anti-Xa levels is indicated. There are limited clinical
data available on the use of direct oral anticoagulants (DOACs), Sickle cell disease
such as dabigatran, rivaroxaban and apixaban, for patients with a VTE is a common comorbid condition found in sickle cell disease
BMI ≥40 kg/m2. DOAC activity levels should be monitored in these (SCD) and is associated with increased mortality.
patients using a drug-specific peak level.[19] The incidence of thrombotic stroke and pulmonary embolism
is higher than in persons without SCD.[26,27] SCD is also a risk
Cancer factor for pregnancy-related VTE (odds ratio (OR) 20.3).[28] As the
The risk of VTE is significantly increased among patients with pathogenesis of vaso-occlusion is multifactorial, the precise role
cancer, with an estimated relative risk 4 - 7-fold above that of the of hypercoagulability is not certain. The preponderance of evidence
background population.[20] The basis for malignancy-associated demonstrates increased platelet and coagulation activation.
VTE include factors related to the cancer itself (such as expression Prothrombin fragment 1.2, a marker of thrombin generation, is
of procoagulant molecules, particularly TF, by the tumour cells), elevated in SCD. Phosphatidyl serine exposure on the surface of the
chemotherapy-related endothelial injury and/or increased frequency red cell membrane is thought to serve as a trigger, with contributing
of other risks for VTE (e.g. major surgery, immobilisation, vascular factors, such as functional asplenia and nitric oxide depletion due to
obstruction by tumour masses or indwelling venous catheters).[21] chronic haemolysis.[29]
VTE rates are particularly high in certain types of cancer (such as Prophylactic anticoagulation is recommended during potentially
haematological neoplasms, and tumours of the stomach, pancreas, triggering events such as perioperative periods and indwelling venous
brain, lung and breast),[21,22] in advanced-stage disease and when catheters. Meaningful data on the long-term use of anticoagulants
therapeutic agents with increased thrombogenic potential are used, or antiplatelet agents are lacking owing to small and/or poorly
such as platinum-based chemotherapy agents, immunomodulatory controlled studies.
drugs (e.g. thalidamide, tamoxifen) and haemopoietic-stimulating
agents (e.g. erythropoietin).[21,22] Clinical entities characterised by a
Despite the increased risk of VTE in association with cancer, thrombotic tendency
routine primary prophylaxis among ambulatory individuals with a The antiphospholipid syndrome
malignancy is not advocated, as the rate of bleeding complications APS is associated with a predilection to thrombosis and recurrent
is also elevated with LMWH-based VTE prophylaxis.[21,22] However, morbidity related to pregnancy. Thrombosis can affect any vessel
thromboprophylaxis is recommended for hospital inpatients, (arterial, venous or the microvasculature), and recurs often. The
particularly following major surgery, such as abdomenopelvic surgery, pathogenesis of thrombotic APS is not well understood, but the
which necessitates prophylaxis with LMWH for 30 days.[21] Among binding of autoantibodies directed against various phospholipids
patients with confirmed thrombosis, therapeutic doses of LMWH or phospholipid-binding proteins (including cardiolipin and beta-2
have shown superior efficacy compared with oral vitamin K antagonists, glycoprotein I) results in: (i) upregulated monocyte and endothelial
possibly due to difficulties in achieving predictable anticoagulation cell TF expression; (ii) platelet activation; and (iii) disruption of
in patients with cancer owing to numerous drug-drug interactions, natural anticoagulant mechanisms (such as the activated PC pathway
poor diet/vomiting (which can affect vitamin K bio-availability) and the annexin V shield (which blocks access of coagulation
or associated liver/renal impairment.[21] Early indications suggest factors to procoagulant phospholipid surfaces).[30] The most common
that the DOACs, rivaroxaban, apixaban and edoxaban (of which thrombotic manifestations include cerebrovascular accidents, lower-
only rivaroxaban is currently available in SA), may be acceptable limb deep-vein thrombosis and pulmonary embolism.[3] APS should
alternatives for the management of VTE, but caution is warranted if be suspected if:
potent inducers or inhibitors of CYP450 are used concomitantly.[21,23] • thrombosis occurs in a young patient, at an unusual site or recurs[31]
183 March 2020, Vol. 110, No. 3
CME
• other clinical features associated with APS are present, including and platelet FIV (PF4), which is an endogenous platelet protein
underlying systemic lupus erythematosus, mild thrombocytopenia, released from the alpha granules of platelets on platelet activation.[33,34]
autoimmune haemolysis, livedo reticularis, cardiac valve When bound to heparin-PF4 complexes, these antibodies cross-link
thickening or vegetations, thrombotic microangiopathy, recurrent FcƔRIIa receptors on platelets and monocytes, which generates
miscarriages, nephropathy, neurological abnormalities or unex a prothrombotic state by triggering platelet activation and TF
plained prolongation of the activated partial thromboplastin time expression on the surface of monocytes.[34]
(aPTT).[31] These antibodies occur fairly commonly in patients exposed to
heparin, but HIT occurs in only 0.2 - 3.0% of such patients.[34] Factors
The diagnosis is based on the revised Sapporo criteria, which require associated with a high risk of HIT include a history of recent
demonstration of ≥1 laboratory criteria with ≥1 clinical manifestations major surgery, unfractionated heparin (UFH) exposure and use of
(Table 2).[32] The laboratory findings (i.e. anticardiolipin antibodies, therapeutic doses of LMWH.[34] Notably, the risk of HIT is significantly
anti-beta-2 glycoprotein antibodies or a lupus anticoagulant) are lower with prophylactic doses of LMWH.[33,34] Diagnosis is primarily
somewhat nonspecific, and can occur transiently after a viral infection based on clinical suspicion, with the presence of thrombocytopenia
or secondary to underlying autoimmune pathology, malignancy or or thrombosis at the appropriate time interval following heparin
drug exposure. Persistence of these abnormalities must therefore be exposure without an alternative cause (assessed in the 4T score)
demonstrated for >12 weeks with appropriate clinical manifestations (Table 3). HIT can be excluded if the 4T score is low (<4), but requires
before a diagnosis of APS can be made. laboratory confirmation when the score is intermediate or high.[33,34]
Management of thrombotic APS entails lifelong anticoagulation Laboratory tests available in SA include functional tests that detect
with a vitamin K antagonist (such as warfarin and a target platelet activation upon heparin exposure, as well as immunoassays
international normalised ratio (INR) of 2 - 3), with optimisation that demonstrate antiheparin/PF4 antibodies. The immunoassays
of other risk factors for thrombosis (e.g. hypertension, hyper have superior sensitivity, but poorer specificity; therefore, while a
cholesterolaemia). Concomitant use of aspirin is advocated for negative result excludes a diagnosis of HIT, a positive result is only
arterial thrombosis in patients with significant risk factors for confirmatory when the 4T score is high.[34] In contrast, the sensitivity of
cardiovascular disease. In the event of recurrent thrombosis despite the functional assay is lower, but its specificity is higher, and a positive
adequate anticoagulation (a well-described complication), options functional test result therefore confirms a diagnosis of HIT, even in
include the addition of aspirin, use of high-dose vitamin K antagonist patients with an intermediate 4T score.[34] Knowledge regarding the type
therapy (target INR 3 - 4) and/or an alternative anticoagulant of assay performed is important; therefore, consultation with regional
(particularly LMWH). Currently, DOACs are not advocated for the laboratory services is necessary.
management of APS, as their efficacy and safety are not proven.[31] Management of HIT entails immediate cessation of heparin therapy
and commencement of an agent that does not cross-react with the
Heparin-induced thrombocytopenia antiheparin/PF4 antibodies. Importantly, the results of laboratory
Heparin-induced thrombocytopenia (HIT) is an immunological assays should not be awaited before initiating the alternative
complication of heparin therapy that is associated with a decrease anticoagulant, as the risk of thrombosis is very high (~50%),[33] and
in the platelet count (usually resulting in thrombocytopenia) and an the test results are often not available for a few days. Agents that can
increase in the risk of thrombosis (both venous and arterial).[33,34] It be employed include parenteral inhibitors of thrombin (argatroban),
typically develops 5 - 10 days after the commencement of heparin FXa (fondaparinux) or the DOACs (dabigatran or rivaroxiban).[35]
therapy, except in patients with a history of recent heparin exposure, LMWH should be avoided. Warfarin is contraindicated, as warfarin-
in whom the clinical features may manifest more rapidly. It is caused related PC deficiency may cause significant extension of the
by the production of antibodies directed against a complex of heparin thrombus, with a risk of venous gangrene.[33,34] In the absence
Table 2. Revised Sapporo classification criteria for the diagnosis of antiphospholipid syndrome[32]
Clinical criteria
Objectively confirmed arterial, venous or small-vessel thrombosis in any organ
Pregnancy morbidity
• ≥1 unexplained death/s of a morphologically normal fetus at or beyond the 10th week of gestation
• ≥1 premature birth/s of a morphologically normal neonate before the 34th week of gestation due to eclampsia, severe pre-eclampsia or
placental insufficiency
• ≥3 unexplained, consecutive spontaneous miscarriages before the 10th week of gestation (without maternal anatomical or paternal and
maternal chromosomal abnormalities)
Laboratory criteria
LA on ≥2 occasions at least 12 weeks apart (detected by prolongation of a phospholipid-dependent clotting time, e.g. DRVVT, lupus-sensitive
aPTT)
ACL antibody (IgG and/or IgM) measured by an ELISA-based immunological assay, present in medium- or high-titre (i.e. ≥40 GPL or MPL),
on ≥2 occasions, at least 12 weeks apart
Anti-β2-glycoprotein I (IgG and/or IgM) measured by an ELISA-based immunological assay, present in medium- or high-titre (i.e. ≥99th percen
tile), on ≥2 occasions, at least 12 weeks apart
Patients with LA positivity are at greater risk of clinical events, particularly those with triple positivity for LA, ACL and anti-β2-glycoprotein I
LA = lupus anticoagulant; DRVVT = dilute Russell viper venom time; aPTT = activated partial thromboplastin time; ACL = anticardiolipin; ELISA = enzyme-linked immunosorbent assay;
GPL = IgG phospholipid; MPL = IgM phospholipid.
184 March 2020, Vol. 110, No. 3
CME
Table 3. 4T scoring system* for the diagnosis of heparin-induced thrombocytopenia
+2 +1 0
Thrombocytopenia Platelet count fall >50% and Platelet count fall 30 - 50% or Platelet count fall <30% or
platelet nadir ≥20 platelet nadir 10 - 19 platelet nadir <10
Timing Definite onset between days 5 and Probable onset between Platelet count fall <4 days
10 or platelet count fall ≤1 day days 5 and 10, but not clear; without recent exposure
if heparin exposure in the past onset after day 10 or platelet
30 days count fall ≤1 day if heparin
exposure in the past 30 - 100 days
Thrombosis New thrombosis or skin necrosis/ Progressive or recurrent None
acute systemic reaction after thrombosis; suspected
intravenous heparin bolus thrombosis (not proven)
Other causes for thrombocytopenia None apparent Possible Definite
*<4 = low risk; 4 - 5 = intermediate risk; 6 - 8 = high risk. Heparin was started on day 0.
of thrombosis, alternative anticoagulation
Symptoms of DVT: unilateral leg swelling, redness, pain or
treatment should be maintained for 4 weeks. discomfort, warmth and tenderness to touch
If thrombosis is present, warfarin should Symptoms of PE: dyspnoea, chest pain or tightness,
haemoptysis, syncope or collapse, tachycardia and/
be commenced once the platelet count has or hypotension (shock)
normalised (>150 × 109/L on ≥2 occasions),
and continued for 3 months.[34]
Paroxysmal nocturnal Apply clinical decision rule
haemoglobinuria • suspected DVT: Wells' DVT score (Table 4)
• suspected PE: Wells' PE score (Table 5)
Paroxysmal nocturnal haemoglobinuria
(PNH) is a rare clonal disorder that is caused
by an acquired mutation of the PIG-A gene, VTE unlikely VTE likely
which encodes an anchor molecule (glyco-
sylphosphatidylinositol (GPI)) required for
affixing a number of proteins on cell surfaces
(including the complement-inactivating pro- Perform D-dimer blood test
teins CD55 and CD59).[36] Cells with GPI
deficiency are thus vulnerable to comple-
ment activation on their surfaces, which
can cause cell lysis (in the case of red cells), Negative Positive Perform compression ultrasonography
(Doppler) for leg DVT or computed
cellular activation (in the case of platelets) tomography pulmonary angiography for PE
and indirectly, endothelial dysfunction.[36,37]
This accounts for the clinical manifestations
of PNH, which include episodic haemo
globinuria (due to intravascular haemolysis) DVT or PE excluded
Negative Positive
DVT or PE confirmed
and a predilection to thrombosis. PNH-
positive clones may also be seen in patients
with underlying haematological disorders Fig. 2. Diagnostic approach for patients with suspected venous thromboembolism. (VTE = venous
(particularly aplastic anaemia), although thromboembolism; DVT = deep-vein thrombosis; PE = pulmonary embolism.)
typical clinical manifestations of PNH are
unusual in this setting. PNH should be sus- Diagnostic considerations antithrombin) and elevated homocysteine
pected in patients with thrombosis, who also The algorithm in Fig. 2 outlines a diagnostic levels tend to be of low yield, and testing for
have cytopenias, iron deficiency (as a conse- approach for suspected thromboembolic dis- these should generally be limited to patients
quence of long-standing haemoglobinuria), ease.[38] Wells’ scores for clinical assessment of with particularly high-risk and unique
evidence of intravascular haemolysis or deep-vein thrombosis and pulmonary embo- presentations.
when thrombosis is detected at unusual lism appear in Tables 4 and 5, respectively. Thrombophilia testing need not be done
sites (particularly intra-abdominal or cere- in patients with a clear provoking event,
bral veins).[37] Diagnosis is made on flow Thrombophilia testing such as recent major orthopaedic surgery in
cytometry, which is used to detect cell popu- FV Leiden (which does not occur among black the absence of other factors suspicious for
lations that do not express GPI-linked surface population affinity groups) and prothrombin thrombophilia, or in those with underlying
antigens.[36] PNH-associated thrombosis can gene (20210A) mutations together with malignancy, as results are unlikely to alter
be very difficult to manage; these patients antiphospholipid antibodies constitute the the treatment plan.
should be referred to specialist haematology most prevalent thrombophilias. Deficiencies Samples for FV Leiden and prothrombin
centres. of the natural anticoagulants (PC, PS and gene (20210A) mutations, as well as anti
185 March 2020, Vol. 110, No. 3
CME
Table 4. Wells’ score* for deep-vein thrombosis
Criteria Points
Active cancer (patient either received treatment during the previous 6 months or currently receiving palliative treatment) +1
Paralysis, paresis or recent cast immobilisation of the lower extremities +1
Recently bedridden for ≥3 days, or major surgery within the previous 12 weeks, requiring general or regional anaesthesia +1
Localised tenderness along the distribution of the deep-venous system of the leg +1
Swelling of entire leg +1
Calf swelling at least 3 cm larger than that on the asymptomatic side (measured 10 cm below tibial tuberosity) +1
Pitting oedema confined to the symptomatic leg +1
Collateral superficial veins (non-varicose) +1
Previously documented DVT +1
Alternative diagnosis at least as likely as DVT –2
DVT = deep-vein thrombosis.
*Two-level clinical probability: <2 = unlikely; ≥2 = likely. Three-level clinical probability: ≤0 = low; 1 - 2 = intermediate; ≥3 = high.
3. Sud R, Khorana AA. Cancer-associated thrombosis: Risk factors, candidate biomarkers and a risk
Table 5. Wells’ score* for pulmonary embolism model. Thromb Res 2009;123(suppl 4):S18-S21. https://doi.org/10.1016/S0049-3848(09)70137-9
4. Bode M, Mackman N. Regulation of tissue factor gene expression in monocytes and endothelial cells:
Criteria Points Thromboxane A2 as a new player. Vascul Pharmacol 2014;62(2):57-62. https://doi.org/10.1016/j.
vph.2014.05.005
Clinical signs and symptoms of DVT +3 5. Dentan C, Epaulard O, Seynaeve D, Genty C, Bosson JL. Active tuberculosis and venous
PE is the most likely diagnosis or equally likely v. +3 thromboembolism: Association according to international classification of diseases. Clin Infect Dis
2014;58(4):495-501. https://doi.org/10.1093/cid/cit780
another diagnosis 6. Hodkinson KE, Mahlangu JN. Deep-vein thrombosis in the era of high HIV and tuberculosis
prevalence: A prospective review of its diagnosis and treatment in a quaternary centre. S Afr Med J
Heart rate >100/min +1.5 2017;107(10):859-863. https://doi.org/10.7196/SAMJ.2017.v107i10.12443
Immobilisation for at least 3 days or surgery in the +1.5 7. Jong E, Louw S, Meijers JC, et al. The hemostatic balance in HIV-infected patients with and without
antiretroviral therapy: Partial restoration with antiretroviral therapy. AIDS Patient Care STDS
previous 4 weeks 2009;23(12):1001-1007. https://doi.org/10.1089/apc.2009.0173
Previous, objectively diagnosed PE or DVT +1.5 8. Mayne ES, Louw S. Good fences make good neighbors: Human immunodeficiency virus and vascular
disease. Open Forum Infect Dis 2019;6(11):ofz303. https://doi.org/10.1093/ofid/ofz303
Haemoptysis +1 9. Jacobson BF, Louw S, Buller H, et al. Venous thromboembolism: Prophylactic and therapeutic practice
guideline. S Afr Med J 2013;103(4):260-267. https://doi.org/10.7196/samj.6706
Malignancy with treatment within 6 months or +1 10. Dager WE, Tsu LV, Pon TK. Considerations for systemic anticoagulation in ESRD. Semin Dial
palliation 2015;28(4):354-362. https://doi.org/10.1111/sdi.12376
11. Lutz J, Menke J, Sollinger D, Schinzel H, Thurmel K. Haemostasis in chronic kidney disease. Nephrol
DVT = deep-vein thrombosis; PE = pulmonary embolism. Dial Transplant 2014;29(1):29-40. https://doi.org/10.1093/ndt/gft209
*>6 = high probability; 2 - 6 = moderate probability; <2 = low risk. 12. Giannotta M, Tapete G, Emmi G, Silvestri E, Milla M. Thrombosis in inflammatory bowel diseases:
What’s the link? Thromb J 2015;13:14. https://doi.org/10.1186/s12959-015-0044-2
13. Zezos P, Kouklakis G, Saibil F. Inflammatory bowel disease and thromboembolism. World J Gastroenterol
2014;20(38):13863-13878. https://doi.org/10.3748/wjg.v20.i38.13863
14. Stegeman BH, de Bastos M, Rosendaal FR, et al. Different combined oral contraceptives and the risk
phospholipid antibodies (excluding functional lupus anticoagulant), of venous thrombosis: Systematic review and network meta-analysis. BMJ 2013;347:f5298. https://doi.
can be collected in the acute phase of thrombosis, as these results org/10.1136/bmj.f5298
15. Wilkinson H, Trustees, Medical Advisers. Saving mothers’ lives. Reviewing maternal deaths to
are not affected by acute thrombosis or anticoagulants. Functional make motherhood safer: 2006 - 2008. Br J Obstet Gynaecol 2011;118(11):1402-1404. https://doi.
lupus anticoagulant testing, as well as testing for PC and PS and org/10.1111/j.1471-0528.2011.03097.x
16. Bates SM, Greer IA, Middeldorp S, et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy:
antithrombin deficiencies, should preferably be delayed until completion Antithrombotic therapy and prevention of thrombosis. Chest 2012;141(2 Suppl):e691S-e736S. https://
of anticoagulation therapy. However, these can be collected in the acute doi.org/10.1378/chest.11-2300
17. Morange PE, Alessi MC. Thrombosis in central obesity and metabolic syndrome: Mechanisms and
phase prior to initiation of therapy in those patients who might require epidemiology. Thromb Haemost 2013;110(4):669-680. https://doi.org/10.1160/TH13-01-0075
18. Frederiksen SG, Hedenbro JL, Norgren L. Enoxaparin effect depends on body-weight and current
lifelong anticoagulation. doses may be inadequate in obese patients. Br J Surg 2003;90(9):1165-1166.
19. Martin K, Beyer-Westendorf J, Davidson BL, et al. Use of the direct oral anticoagulants in obese
Conclusions patients: Guidance from the SSC of the ISTH. J Thromb Haemost 2016;14(6):1308-1313. https://doi.
org/10.1111/jth.13323
The aetiology and pathogenesis of acquired thromboses are fairly 20. Timp JF, Braekkan SK, Versteeg HH, Cannegieter SC. Epidemiology of cancer-associated venous
thrombosis. Blood 2013;122(10):1712-1723. https://doi.org/10.1182/blood-2013-04-460121
diverse and depend to a large extent on the primary pathology and 21. Fernandes CJ, Morinaga LTK, Alves JL, jun., et al. Cancer-associated thrombosis: The when, how and
why. Eur Respir Rev 2019;28(151):pii180119. https://doi.org/10.1183/16000617.0119-2018
associated compounding factors. 22. Streiff MB. Thrombosis in the setting of cancer. Hematol Am Soc Hematol Educ Program
An accurate history (with knowledge of pre-existing conditions), 2016;2016(1):196-205. https://doi.org/10.1182/asheducation-2016.1.196
23. Kraaijpoel N, Carrier M. How I treat cancer-associated venous thromboembolism. Blood
physical examination and appropriate investigations are imperative 2019;133(4):291-298. https://doi.org/10.1182/blood-2018-08-835595
for proper diagnosis and management of acquired thrombophilia. 24. Khorana AA, Noble S, Lee AYY, et al. Role of direct oral anticoagulants in the treatment of cancer
associated venous thromboembolism: Guidance from the SSC of the ISTH. J Thromb Haemost
2018;16(9):1891-1894. https://doi.org/10.1111/jth.14219
25. Delluc A, Antic D, Lecumberri R, Ay C, Meyer G, Carrier M. Occult cancer screening in patients with
venous thromboembolism: Guidance from the SSC of the ISTH. J Thromb Haemost 2017;15(10):2076-2079.
Declaration. None. https://doi.org/10.1111/jth.13791
26. Lijfering WM, Brouwer JL, Veeger NJ, et al. Selective testing for thrombophilia in patients with first
Acknowledgements. None. venous thrombosis: Results from a retrospective family cohort study on absolute thrombotic risk for
currently known thrombophilic defects in 2 479 relatives. Blood 2009;113(21):5314-5322. https://doi.
Author contributions. NAA: concept, design and content; JV: design and org/10.1182/blood-2008-10-184879
content; SL: content; ES: content; and BJ: content. 27. Spencer FA, Emery C, Joffe SW, et al. Incidence rates, clinical profile, and outcomes of patients with
venous thromboembolism. The Worcester VTE study. J Thromb Thrombolysis 2009;28(4):401-409.
Funding. None. https://doi.org/10.1007/s11239-009-0378-3
28. Noubiap JJ, Temgoua MN, Tankeu R. Sickle cell disease, sickle trait and the risk for venous thromboembolism:
Conflicts of interest. None. A systematic review and meta-analysis. Thromb J 2018;16:27. https://doi.org/10.1186/s12959-018-0179-z
29. De Franceschi L, Cappellini MD, Olivieri O. Thrombosis and sickle cell desease. Semin Thromb
Hemost 2011;37(3):226-236. https://doi.org/10.1055/s-0031-1273087
1. Alli NA, Vaughan J, Louw S, Schapkaitz E, Jacobson B. Thrombotic disorders (part 1). S Afr Med J 30. Linnemann B. Antiphospholipid syndrome – an update. Vasa 2018;47(6):451-464. https://doi.
2020;110(2):83-87. https://doi.org/10.7196/SAMJ.2020.v110i2.14594 org/10.1024/0301-1526/a000723
2. Gale AJ. Current understanding of hemostasis. Toxicol Pathol 2011;39(1):273-280. https://doi. 31. Garcia D, Erkan D. Diagnosis and management of the antiphospholipid syndrome. N Engl J Med
org/10.1177/0192623310389474 2018;379(13):1290. https://doi.org/10.1056/NEJMc1808253
186 March 2020, Vol. 110, No. 3
CME
32. Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the 36. Luzzatto L. Recent advances in the pathogenesis and treatment of paroxysmal nocturnal
classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost 2006;4(2):295-306. hemoglobinuria. F1000Res 2016;5:pii. https://doi.org/10.12688/f1000research.7288.1
https://doi.org/10.1111/j.1538-7836.2006.01753.x 37. Hill A, Kelly RJ, Hillmen P. Thrombosis in paroxysmal nocturnal hemoglobinuria. Blood
33. Greinacher A. Heparin-induced thrombocytopenia. N Engl J Med 2015;373(19):1883-1884. 2013;121(25):4985-4996,5105. https://doi.org/10.1182/blood-2012-09-311381
34. Arepally GM. Heparin-induced thrombocytopenia. Blood 2017;129(21):2864-2872. https://doi. 38. Tritschler T, Kraaijpoel N, le Gal G, Wells PS. Venous thromboembolism: Advances in diagnosis and
org/10.1056/NEJMc1510993 treatment. JAMA 2018;320(15):1583-1594. https://doi.org/10.1001/jama.2018.14346
35. Cuker A, Arepally GM, Chong BH, et al. American Society of Hematology 2018 guidelines for
management of venous thromboembolism: Heparin-induced thrombocytopenia. Blood Adv
2018;2(22):3360-3392. https://doi.org/10.1182/bloodadvances.2018024489 Accepted 31 January 2020.
187 March 2020, Vol. 110, No. 3
You might also like
- Instant Download Ebook PDF Exploring Biology in The Laboratory PDF ScribdDocument41 pagesInstant Download Ebook PDF Exploring Biology in The Laboratory PDF Scribdida.clemmons523100% (45)
- Unit IG2: Risk Assessment: You Should Aim To Complete This Section in 150 - 200 WordsDocument17 pagesUnit IG2: Risk Assessment: You Should Aim To Complete This Section in 150 - 200 WordsMuhammad FaiSal100% (7)
- DSR Aor For Wet Riser and Sprinkler System 2019Document110 pagesDSR Aor For Wet Riser and Sprinkler System 2019Sambit Pattanaik50% (2)
- PAR in Hemostasis 5Document8 pagesPAR in Hemostasis 5Saddam FuadNo ratings yet
- Physiology of Hemostasis - Dr. Rahmat Dani Satria PH.D., SP - PK (K)Document27 pagesPhysiology of Hemostasis - Dr. Rahmat Dani Satria PH.D., SP - PK (K)Viand NugrohoNo ratings yet
- Ane 0b013e31819bceb1Document6 pagesAne 0b013e31819bceb1Buthaina HusseinNo ratings yet
- HIS1-K38 Obat-Obat Pada Gangguan Koagulasi (Antikoagulan)Document40 pagesHIS1-K38 Obat-Obat Pada Gangguan Koagulasi (Antikoagulan)Ega FlorenceNo ratings yet
- Review Article: Factor V Leiden and InflammationDocument11 pagesReview Article: Factor V Leiden and InflammationSarra KlaiNo ratings yet
- Mackman and Grover 2018 - ReviewDocument17 pagesMackman and Grover 2018 - ReviewBharani tharanNo ratings yet
- Lesson 24Document16 pagesLesson 24Anshika BhargavaNo ratings yet
- CoagulationDocument13 pagesCoagulationpinedaalexa758No ratings yet
- PerfusionDocument4 pagesPerfusionmistry govindNo ratings yet
- Lecture HemostasisDocument28 pagesLecture HemostasisЛариса ТкачеваNo ratings yet
- The Effects of Pituitary and Thyroid Disorders On Haemostasis, Potential Clinical ImplicationsDocument12 pagesThe Effects of Pituitary and Thyroid Disorders On Haemostasis, Potential Clinical ImplicationsTamara Silva FabresNo ratings yet
- Tissue Factor: An Essential Mediator of Hemostasis and Trigger of ThrombosisDocument19 pagesTissue Factor: An Essential Mediator of Hemostasis and Trigger of ThrombosisFatah Jati PNo ratings yet
- Articulo PDFDocument11 pagesArticulo PDFmartin najeraNo ratings yet
- Labmed33 0948Document6 pagesLabmed33 0948VKTNNo ratings yet
- Merged 2022 11 30 21-19-53Document45 pagesMerged 2022 11 30 21-19-53DTM FHKNo ratings yet
- Disseminated Intravascular Coagulation: Keith Lewis, MDDocument37 pagesDisseminated Intravascular Coagulation: Keith Lewis, MDRitamaria100% (1)
- DivitiDocument36 pagesDivitiMarLeniRNNo ratings yet
- P.08 BLEEDING Dr. Buliyat 09 03 18Document5 pagesP.08 BLEEDING Dr. Buliyat 09 03 18Raymund Dan AldabaNo ratings yet
- 33-Hemostasis and Coagulation ProfileDocument40 pages33-Hemostasis and Coagulation ProfileOsman Mohamed MuhumedNo ratings yet
- SF Ms Encoded Notes Compilation PDFDocument86 pagesSF Ms Encoded Notes Compilation PDFkayekristine2001No ratings yet
- (Pedia 3B) Hematology B (Dra. Rondilla) ?Document12 pages(Pedia 3B) Hematology B (Dra. Rondilla) ?Andrea GuidoteNo ratings yet
- 6 Hemostasis & ThrombosisDocument38 pages6 Hemostasis & Thrombosisجهاد مالك حاتم حسينNo ratings yet
- CoagulationDocument3 pagesCoagulationHerho-nyl CesNo ratings yet
- PT & Aptt: Manish PandeyDocument42 pagesPT & Aptt: Manish PandeyMarj MendezNo ratings yet
- 2020 Therapeutic Strategies For Thrombosis - New Targets and ApproachesDocument20 pages2020 Therapeutic Strategies For Thrombosis - New Targets and ApproachesVladimir BasurtoNo ratings yet
- Blood Vessels and Endothelial CellsDocument4 pagesBlood Vessels and Endothelial CellsJemmy FandriNo ratings yet
- Hemostasis 1Document24 pagesHemostasis 1novriadi suhendraNo ratings yet
- Hemostasis: Overview of Normal Hemostasis 3Document23 pagesHemostasis: Overview of Normal Hemostasis 3Joce Maripangui100% (1)
- Disseminated Intravascular Coagulation: Current Concepts: R. Kumar and V. GuptaDocument6 pagesDisseminated Intravascular Coagulation: Current Concepts: R. Kumar and V. GuptantnquynhproNo ratings yet
- DIC Pada AnakDocument6 pagesDIC Pada AnakRizky LumalessilNo ratings yet
- Chapter 119_ Sickle Cell DiseaseDocument35 pagesChapter 119_ Sickle Cell Diseasemcoghill3No ratings yet
- Coagulation DisordersDocument9 pagesCoagulation DisordersIS99057No ratings yet
- Hemostatic Physiology: Mansyur Arif Dept. of Clinical Pathology Faculty of Medicine, Hasanuddin University, MakassarDocument67 pagesHemostatic Physiology: Mansyur Arif Dept. of Clinical Pathology Faculty of Medicine, Hasanuddin University, Makassarnurliah armandNo ratings yet
- Platelets PDFDocument65 pagesPlatelets PDFLana AmerieNo ratings yet
- Periodonta MX of Bleediing DisordersDocument21 pagesPeriodonta MX of Bleediing Disordersjosee aminNo ratings yet
- Hema - PointersDocument5 pagesHema - PointersLUALHATI VILLASNo ratings yet
- Hemostasis and Hemostatic DisordersDocument7 pagesHemostasis and Hemostatic DisordersBlitzen BusaingNo ratings yet
- HemostasisDocument58 pagesHemostasisRade GrbićNo ratings yet
- Hemostasis Practice: State-Of-The-Art: Giuseppe Lippi, Emmanuel J. FavaloroDocument6 pagesHemostasis Practice: State-Of-The-Art: Giuseppe Lippi, Emmanuel J. FavaloroRilia IrianiNo ratings yet
- Hemostasis and Coagulation: Miklós MolnárDocument67 pagesHemostasis and Coagulation: Miklós MolnárHamzaNo ratings yet
- 29 Bleeding Tendency-4Document66 pages29 Bleeding Tendency-4Youssef Refaat RaoofNo ratings yet
- Coagulation - Intrinsic - Extrinsic - Fibrinolysis - TeachMePhysiologyDocument3 pagesCoagulation - Intrinsic - Extrinsic - Fibrinolysis - TeachMePhysiologymaroua boukhechbaNo ratings yet
- Hemostasis in The Surgical PatientDocument39 pagesHemostasis in The Surgical Patientninjahattori1No ratings yet
- HemostasisDocument14 pagesHemostasisGowtham SelvarajNo ratings yet
- Drug Moa PK Use Se Ci Blood Coagulation: AnticoagulantsDocument4 pagesDrug Moa PK Use Se Ci Blood Coagulation: AnticoagulantsYusoff RamdzanNo ratings yet
- Mekanisme Hemostasis & Koagulasi (Prof. Dr. Mansyur Arif, PH.D, SP - PK (K) )Document55 pagesMekanisme Hemostasis & Koagulasi (Prof. Dr. Mansyur Arif, PH.D, SP - PK (K) )ikram hanafiNo ratings yet
- 143 - HaemostasisDocument6 pages143 - HaemostasisRahul DhulipalaNo ratings yet
- Chapter 35 Part 1Document31 pagesChapter 35 Part 1Gordon JamesonNo ratings yet
- Topical Hemostatic Agents in Surgery PDFDocument10 pagesTopical Hemostatic Agents in Surgery PDFFernanda SouzaNo ratings yet
- Multiple TraumaDocument10 pagesMultiple TraumaAurelia AlexandraNo ratings yet
- Biochemistry of The Blood Coagulation SystemDocument4 pagesBiochemistry of The Blood Coagulation Systemabc007200100% (1)
- Aspek Laboratorium Kelainan HemostasisDocument48 pagesAspek Laboratorium Kelainan HemostasisriskypiradeNo ratings yet
- Bleeding in Children SmsDocument65 pagesBleeding in Children SmsAnastasiafynnNo ratings yet
- Normal HemostasisDocument34 pagesNormal Hemostasisمصطفي خندقاويNo ratings yet
- Normal HaemostasisDocument36 pagesNormal HaemostasisReem EshraNo ratings yet
- HaematologyDocument3 pagesHaematologyrileyNo ratings yet
- Tissue Factor and Tissue Factor Pathway InhibitorDocument10 pagesTissue Factor and Tissue Factor Pathway Inhibitorfranciscrick69No ratings yet
- ClottingDocument25 pagesClottingAtalabi AdebusolaNo ratings yet
- Chapter 4 Hemostasis, Surgical Bleeding, and Transfusion 35Document13 pagesChapter 4 Hemostasis, Surgical Bleeding, and Transfusion 35Vladimir OstriaNo ratings yet
- Proofs BM GT 5 2Document38 pagesProofs BM GT 5 2Iqra NazirNo ratings yet
- Construction Technology & Project Management: Dr. V Srinivasa ReddyDocument111 pagesConstruction Technology & Project Management: Dr. V Srinivasa Reddychaudhari prajaktaNo ratings yet
- Slnoempno Category Name Grade Designation Sbu Function Address Telephone NoDocument10 pagesSlnoempno Category Name Grade Designation Sbu Function Address Telephone NoAARTINo ratings yet
- Surat Offers ListDocument3 pagesSurat Offers List19-004 AKSHAYKUMARNo ratings yet
- PQA Australia 1Document6 pagesPQA Australia 1Mary Ann SantosNo ratings yet
- Restaurant Management System DatabaseDocument25 pagesRestaurant Management System DatabaseahrmzdhNo ratings yet
- Zt400 Series Parts Catalog en UsDocument11 pagesZt400 Series Parts Catalog en UsangevilessNo ratings yet
- Act 2 Head On Collision Convergent-2018 (3) XsxsxsDocument4 pagesAct 2 Head On Collision Convergent-2018 (3) XsxsxsKelly Sheine SisonNo ratings yet
- Service Manual Fe-1: KV-29X5A KV-29X5B KV-29X5D KV-29X5E KV-29X5K KV-29X5L KV-29X5R KV-29X5UDocument7 pagesService Manual Fe-1: KV-29X5A KV-29X5B KV-29X5D KV-29X5E KV-29X5K KV-29X5L KV-29X5R KV-29X5USofia MendesNo ratings yet
- Math Ni LykaDocument4 pagesMath Ni LykaAnonymous 6gq4mhINo ratings yet
- Boilere Solare BSTDocument8 pagesBoilere Solare BSTTirla AlexandraNo ratings yet
- Elite Paint and Chemical Industries LimitedDocument52 pagesElite Paint and Chemical Industries Limitedtanthu nagNo ratings yet
- Space Factors AreaDocument4 pagesSpace Factors AreajadeNo ratings yet
- Social Studies Lesson PlanDocument3 pagesSocial Studies Lesson Planapi-219095854No ratings yet
- Thesis Land Use ChangeDocument6 pagesThesis Land Use Changeafazapfjl100% (1)
- Cs LabDocument10 pagesCs LabsreeragNo ratings yet
- Settlement For Cohesive SoilDocument9 pagesSettlement For Cohesive SoilQuach TuanNo ratings yet
- SECO 02-2022-04 UpdateDocument13 pagesSECO 02-2022-04 UpdateJoachim HagegeNo ratings yet
- Case #3Document47 pagesCase #3Elaiza Jamez PucateNo ratings yet
- Presentation ResultsDocument39 pagesPresentation ResultsPayal JainNo ratings yet
- REDRAGON Distributers 14.3.2021Document52 pagesREDRAGON Distributers 14.3.2021Ahmed Abd ElwanessNo ratings yet
- BS 300Document3 pagesBS 300Kristina PodolyakoNo ratings yet
- Wooden Adjustable Measuring SpoonDocument3 pagesWooden Adjustable Measuring SpoonArchita GogoiNo ratings yet
- Envato 16 June v6.0Document7 pagesEnvato 16 June v6.0Нурасыл АртыкбайNo ratings yet
- Rincian Harga CCTV: Paket All Dahua 4 ChannelDocument2 pagesRincian Harga CCTV: Paket All Dahua 4 ChannelazharNo ratings yet
- Mobil Delvac Super 1300 15W-40 (Old CG4)Document2 pagesMobil Delvac Super 1300 15W-40 (Old CG4)Muhammad Abdul RehmanNo ratings yet
- Catalytic Oxidation FormularsDocument1 pageCatalytic Oxidation FormularsUmesh Kumar Sharma RamamoorthiNo ratings yet