GIT Nursing
GIT Nursing
Download as pdf or txt
You might also like
- Ecomm Sales DashboardDocument4 pagesEcomm Sales Dashboardkumar100% (1)
- Nicu Must KnowsDocument7 pagesNicu Must KnowsCyfern100% (3)
- Healthy Pancreas, Healthy You. Part 3. How to Improve the Exocrine Pancreatic Function, Postpone Pancreatic Deterioration, and Heal Digestive (Pancreatic) DisordersFrom EverandHealthy Pancreas, Healthy You. Part 3. How to Improve the Exocrine Pancreatic Function, Postpone Pancreatic Deterioration, and Heal Digestive (Pancreatic) DisordersRating: 5 out of 5 stars5/5 (1)
- Death of A Salesman Scene Breakdown With Sound CuesDocument1 pageDeath of A Salesman Scene Breakdown With Sound CuesEricka AlvarezNo ratings yet
- Healthy Pancreas, Healthy You. Part II. Healing Foods in the Digestive (Pancreatic) DisordersFrom EverandHealthy Pancreas, Healthy You. Part II. Healing Foods in the Digestive (Pancreatic) DisordersRating: 4.5 out of 5 stars4.5/5 (2)
- Healthy Pancreas, Healthy You. Part 1: Structure, Function, and Disorders of the PancreasFrom EverandHealthy Pancreas, Healthy You. Part 1: Structure, Function, and Disorders of the PancreasRating: 4.5 out of 5 stars4.5/5 (4)
- PEDIATRICS DISORDER PART 2 LECTURE MergedDocument33 pagesPEDIATRICS DISORDER PART 2 LECTURE MergedErika CadawanNo ratings yet
- Sweat Chloride Test: 1. Splenic Rupture 2. Avoid Sports and Physical Activity 3. Atypical LymphocytesDocument7 pagesSweat Chloride Test: 1. Splenic Rupture 2. Avoid Sports and Physical Activity 3. Atypical LymphocytesAnonymous GfqHQ5SNwNo ratings yet
- Top Communicable Diseases in The Philippines 2019Document4 pagesTop Communicable Diseases in The Philippines 2019Nicole cuencosNo ratings yet
- ENT - Salivary Gland Diseases (Almazan)Document4 pagesENT - Salivary Gland Diseases (Almazan)Tj Kevin P-DoctorNo ratings yet
- Soil Transmitted HelminthiasesDocument6 pagesSoil Transmitted HelminthiasesJemimah MejiaNo ratings yet
- HCC Exam 4Document20 pagesHCC Exam 4Sheri BarlingNo ratings yet
- Haad RN QuestionDocument7 pagesHaad RN Questionsabu0099100% (1)
- NCMB 312 Finals!Document25 pagesNCMB 312 Finals!Justine Dinice MunozNo ratings yet
- NCMB 312 Finals! (2.0)Document25 pagesNCMB 312 Finals! (2.0)Justine Dinice MunozNo ratings yet
- NCMB 312 Finals! (2.0)Document25 pagesNCMB 312 Finals! (2.0)Justine Dinice MunozNo ratings yet
- Microbio Exam 3Document13 pagesMicrobio Exam 3Cathy LyNo ratings yet
- Midterm Nucama 460Document7 pagesMidterm Nucama 460Reysel MonteroNo ratings yet
- Week 13 NCMB 312 Lect NotesDocument18 pagesWeek 13 NCMB 312 Lect NotesAngie BaylonNo ratings yet
- OB OutlineDocument3 pagesOB Outlinejisoo100% (1)
- MIDTERM EL. 109aDocument13 pagesMIDTERM EL. 109aYla MontealtoNo ratings yet
- MEDII-6.4a Peptic-Ulcer-DiseaseDocument9 pagesMEDII-6.4a Peptic-Ulcer-DiseaseCC Samson, Caesar AnthonyNo ratings yet
- Handbook of PEDIATRIC SURGERY PDFDocument43 pagesHandbook of PEDIATRIC SURGERY PDFPETERNo ratings yet
- Health Education - DiarrheaDocument7 pagesHealth Education - DiarrheaRashmi Devrani VyasNo ratings yet
- Self Learning (Computerized)Document10 pagesSelf Learning (Computerized)watchNo ratings yet
- Presentation 1Document6 pagesPresentation 1Sherylou Kumo SurioNo ratings yet
- Case Study AGE With DehydrationDocument12 pagesCase Study AGE With Dehydrationmwdlc_22100% (2)
- Gastrointestinal Disorders in Children Part Ii: Dra. Ruby Ann PunongbayanDocument8 pagesGastrointestinal Disorders in Children Part Ii: Dra. Ruby Ann PunongbayanMaikka IlaganNo ratings yet
- It Is Caused By:: Definition of TyphusDocument2 pagesIt Is Caused By:: Definition of TyphusAshima Viie BassamahNo ratings yet
- Amoebiasis TranseesDocument2 pagesAmoebiasis TranseesurgrlyennnNo ratings yet
- Pruritusani:Etiology Andmanagement: Katharine W. Markell,, Richard P. BillinghamDocument11 pagesPruritusani:Etiology Andmanagement: Katharine W. Markell,, Richard P. BillinghamSinue PumaNo ratings yet
- Unit 2 Care of Child .EditedDocument20 pagesUnit 2 Care of Child .EditedGian Delos SantosNo ratings yet
- 10 Communicable Disease Control Program IDocument9 pages10 Communicable Disease Control Program IJennica JaoNo ratings yet
- Bacillary DysenteryDocument2 pagesBacillary Dysenteryzynahmaegomez8No ratings yet
- Medical Significance of Understanding BacteriaDocument13 pagesMedical Significance of Understanding BacteriaChazlyn Mae Ronilda ArevaloNo ratings yet
- Infections Dr. Mowafy 2nd EditionDocument26 pagesInfections Dr. Mowafy 2nd EditionMohammed RisqNo ratings yet
- DISTURBANCES IN ABSORPTION AND ELIMINATION NotesDocument7 pagesDISTURBANCES IN ABSORPTION AND ELIMINATION NotesHoneylette Darunday100% (1)
- Complications of LABORDocument9 pagesComplications of LABORCharity Myles Dela cruzNo ratings yet
- Review NTS..NCM 109Document11 pagesReview NTS..NCM 109Celline Isabelle ReyesNo ratings yet
- Presented By: Dave Jay S. Manriquez RN.Document1 pagePresented By: Dave Jay S. Manriquez RN.anthropusNo ratings yet
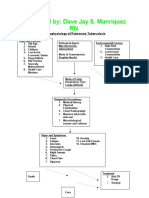
- Pa Tho Physiology of Pulmonary Tuberculosis 1233558918868912 1Document1 pagePa Tho Physiology of Pulmonary Tuberculosis 1233558918868912 1Anna Lorraine NavarroNo ratings yet
- Pa Tho Physiology of Pulmonary Tuberculosis 1233558918868912 1Document1 pagePa Tho Physiology of Pulmonary Tuberculosis 1233558918868912 1Melanie PardoNo ratings yet
- PP PPK BedahDocument10 pagesPP PPK Bedahyohanisrassang1979No ratings yet
- Communicable Diseases 1Document11 pagesCommunicable Diseases 1Glaiza Mae GamatanNo ratings yet
- Module 3B.2 Puerperial InfectionDocument17 pagesModule 3B.2 Puerperial InfectionEmmanuel BillenaNo ratings yet
- Maternal Notes Part IDocument21 pagesMaternal Notes Part Iabbycruz012No ratings yet
- Placenta Previa Case StudyDocument7 pagesPlacenta Previa Case StudyKing NavsunNo ratings yet
- Vector Borne Diseases: Malaria (Ague)Document20 pagesVector Borne Diseases: Malaria (Ague)Nina OaipNo ratings yet
- Oncomelania Quadrasi (Tiny Snail)Document7 pagesOncomelania Quadrasi (Tiny Snail)JoshuaNo ratings yet
- PARASITOSES and MYCOSESDocument7 pagesPARASITOSES and MYCOSESGeriel QuidesNo ratings yet
- Nursing Lecture RespiratoryDocument13 pagesNursing Lecture RespiratoryAedge010100% (1)
- Appendicitis JoyDocument15 pagesAppendicitis JoyJoy Rachel TabernillaNo ratings yet
- Asthma PathophysiologyDocument4 pagesAsthma Pathophysiologysmitha lakkavallyNo ratings yet
- Trauma Survey ReviewerDocument5 pagesTrauma Survey ReviewerRigel Kent C. TobiasNo ratings yet
- PediatricsDocument80 pagesPediatricsmohamed muhsinNo ratings yet
- Surgery 2.01.3 Omentum, Mesentery and Retroperitoneum - Dr. MendozaDocument8 pagesSurgery 2.01.3 Omentum, Mesentery and Retroperitoneum - Dr. MendozaJorge De VeraNo ratings yet
- Fermented Foods for Health: Use the Power of Probiotic Foods to Improve Your Digestion, Strengthen Your Immunity, and Prevent IllnessFrom EverandFermented Foods for Health: Use the Power of Probiotic Foods to Improve Your Digestion, Strengthen Your Immunity, and Prevent IllnessRating: 4.5 out of 5 stars4.5/5 (4)
- The CervixFrom EverandThe CervixJoseph JordanNo ratings yet
- Diverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandDiverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesRating: 1 out of 5 stars1/5 (1)
- The Antibiotic Alternative: The Natural Guide to Fighting Infection and Maintaining a Healthy Immune SystemFrom EverandThe Antibiotic Alternative: The Natural Guide to Fighting Infection and Maintaining a Healthy Immune SystemRating: 5 out of 5 stars5/5 (1)
- 17 2024 NLE Respi HandoutsDocument66 pages17 2024 NLE Respi HandoutsBasa, Rica Mae P.No ratings yet
- Day1 Obped I HandoutsDocument34 pagesDay1 Obped I HandoutsBasa, Rica Mae P.No ratings yet
- 2 Psy Nle HandoutsDocument135 pages2 Psy Nle HandoutsBasa, Rica Mae P.No ratings yet
- DAY1 OBPED I HANDOUTS OkiDocument34 pagesDAY1 OBPED I HANDOUTS OkiBasa, Rica Mae P.No ratings yet
- DAY2 OBPED HANDOUT OkiDocument19 pagesDAY2 OBPED HANDOUT OkiBasa, Rica Mae P.No ratings yet
- 1 Psy Nle HandoutsDocument70 pages1 Psy Nle HandoutsBasa, Rica Mae P.No ratings yet
- Day2 Obped HandoutDocument19 pagesDay2 Obped HandoutBasa, Rica Mae P.No ratings yet
- 3 Psy Nle HandoutsDocument106 pages3 Psy Nle HandoutsBasa, Rica Mae P.No ratings yet
- Mazo Basa NuptialDocument2 pagesMazo Basa NuptialBasa, Rica Mae P.No ratings yet
- Nelly Ombao NCM 112 Lecture Fluid ElectrolytesDocument16 pagesNelly Ombao NCM 112 Lecture Fluid ElectrolytesBasa, Rica Mae P.No ratings yet
- CASE-STUDY-SIR-MARCIAL Mesias V PART 2Document4 pagesCASE-STUDY-SIR-MARCIAL Mesias V PART 2Basa, Rica Mae P.No ratings yet
- Case Study Sir Marcial Mesias VDocument5 pagesCase Study Sir Marcial Mesias VBasa, Rica Mae P.No ratings yet
- Chapter 1-5. EditedDocument34 pagesChapter 1-5. EditedBasa, Rica Mae P.100% (1)
- ACKNOWLEDGEMENT. EditedDocument7 pagesACKNOWLEDGEMENT. EditedBasa, Rica Mae P.No ratings yet
- RABE 1 CHN 2semDocument6 pagesRABE 1 CHN 2semBasa, Rica Mae P.No ratings yet
- Code of EthicsDocument3 pagesCode of EthicsBasa, Rica Mae P.No ratings yet
- RABE 3 CHN 2sem 22Document5 pagesRABE 3 CHN 2sem 22Basa, Rica Mae P.No ratings yet
- Copar Oct 2020Document130 pagesCopar Oct 2020Basa, Rica Mae P.100% (1)
- Rabe 4 CHN NutriDocument7 pagesRabe 4 CHN NutriBasa, Rica Mae P.No ratings yet
- Areva FBX 24kV Tu Trung The RMU 24kV GIS Thanh Cai Cach Dien SF6Document40 pagesAreva FBX 24kV Tu Trung The RMU 24kV GIS Thanh Cai Cach Dien SF6Minh PhuocNo ratings yet
- ALH-901x Firmware Release Notes 2015-02Document3 pagesALH-901x Firmware Release Notes 2015-02Tiranran BakrieNo ratings yet
- Manual de Partes 426Document691 pagesManual de Partes 426Андрей Аникин100% (1)
- Dcu UgDocument34 pagesDcu UgSaed CattywampusNo ratings yet
- Technical: Engine Blueprinting 101 - Part OneDocument4 pagesTechnical: Engine Blueprinting 101 - Part OneRussell GouldenNo ratings yet
- Pastry, Cakes and CookiesDocument9 pagesPastry, Cakes and CookiesMheg Sophia HockkinsNo ratings yet
- Lesson Plan Math ARegrouping1Document2 pagesLesson Plan Math ARegrouping1France BejosaNo ratings yet
- Ag010ksvajh - Ag010ksvajhaa Exploded Parts ViewDocument15 pagesAg010ksvajh - Ag010ksvajhaa Exploded Parts ViewKarthikeyan VisvakNo ratings yet
- DB3 (Diac) DatasheetDocument5 pagesDB3 (Diac) DatasheetMartinez AurelioNo ratings yet
- New ZealandDocument49 pagesNew ZealandElla GAbrielNo ratings yet
- 1.1 Intro To Computer System - COMP111L 1Document27 pages1.1 Intro To Computer System - COMP111L 1Rebecca MarasiganNo ratings yet
- Lab 12 Introduction To Simulink ObjectiveDocument16 pagesLab 12 Introduction To Simulink Objectivesaran gulNo ratings yet
- ME2353 Finite Element Analysis Lecture NotesDocument34 pagesME2353 Finite Element Analysis Lecture Notespgkaero100% (2)
- Digital Graphic Equalizer Implemented Using An FPGADocument122 pagesDigital Graphic Equalizer Implemented Using An FPGAbois_olivierNo ratings yet
- Thlang MarketingDocument17 pagesThlang MarketingPhuc HoangNo ratings yet
- Strategic Compensation in Canada Canadian 5th Edition Long Solutions ManualDocument10 pagesStrategic Compensation in Canada Canadian 5th Edition Long Solutions Manualrobertmahoneycsaymrqnzk100% (16)
- Civil Engineering MCQ'sDocument1 pageCivil Engineering MCQ'sNISHIKANTA MONDALNo ratings yet
- UT Dallas Syllabus For Geos2409.001.09s Taught by William Manton (Manton)Document5 pagesUT Dallas Syllabus For Geos2409.001.09s Taught by William Manton (Manton)UT Dallas Provost's Technology GroupNo ratings yet
- Ethics - Module 7Document5 pagesEthics - Module 7king diyawNo ratings yet
- Bullous Disease Presented By:-Roaa Salah MohammedDocument60 pagesBullous Disease Presented By:-Roaa Salah MohammedIbrahim Sidahmed AliNo ratings yet
- Import Procurement Process in SAP MMDocument2 pagesImport Procurement Process in SAP MMKrishnavel R100% (4)
- ArevaTD PowerTransformersReactors PTR Overview EngDocument12 pagesArevaTD PowerTransformersReactors PTR Overview EngMarcWorldNo ratings yet
- Song For The Mouse (1 and 2 Grade) Song For The Fox (1 and 2 Grade)Document10 pagesSong For The Mouse (1 and 2 Grade) Song For The Fox (1 and 2 Grade)Buse AyvazNo ratings yet
- Index: Primary Production of Milk 1Document10 pagesIndex: Primary Production of Milk 1afefNo ratings yet
- AWT Q & ADocument22 pagesAWT Q & AMasoom RezaNo ratings yet
- GSM Phone Anatomy LatestDocument11 pagesGSM Phone Anatomy LatestabhineetkumarNo ratings yet
- Advanced Systems in Combined Cycle PlantsDocument62 pagesAdvanced Systems in Combined Cycle Plantsclaudia_baca_3100% (1)
- Philo 3rd WorksheetsDocument4 pagesPhilo 3rd WorksheetsAngelyn Lingatong0% (1)