1107398b-09a0 - Salaam Health Claim Form
1107398b-09a0 - Salaam Health Claim Form
Download as pdf or txt
You might also like
- Sail Ipd FormDocument2 pagesSail Ipd Formshami67% (12)
- QIC - NAS Claim FormDocument1 pageQIC - NAS Claim FormIvan80% (5)
- Nas Claim FormDocument1 pageNas Claim Formehtsham007No ratings yet
- SC Health and Welfare FormDocument4 pagesSC Health and Welfare FormLeandro Tamayo25% (8)
- Male and Female Reproductive SystemDocument9 pagesMale and Female Reproductive SystemRein Aldou Panao Enfermo100% (2)
- Claim Form: Important Instructions: (Please Read Carefully)Document2 pagesClaim Form: Important Instructions: (Please Read Carefully)Worlds CrushNo ratings yet
- Claim Form-Salaam TakafulDocument2 pagesClaim Form-Salaam TakafulNiaz Ali0% (1)
- Takaful Claim Form - NewDocument2 pagesTakaful Claim Form - NewmagillaniNo ratings yet
- Pak Takaful Claim FormDocument2 pagesPak Takaful Claim FormRoger Eli Paul100% (1)
- Health Premium PlatinumDocument3 pagesHealth Premium Platinumகமலேஷ் குமார்No ratings yet
- claimformIP_NewRevised (1)Document2 pagesclaimformIP_NewRevised (1)RehanAikMusalmanNo ratings yet
- Claim Form (Out Patient + Hospitalisation)Document2 pagesClaim Form (Out Patient + Hospitalisation)ahsan_hayat28660% (1)
- Group and Individual Medical Claims FormDocument3 pagesGroup and Individual Medical Claims FormSheikh Alif Amzar BuxNo ratings yet
- Medi AssistDocument4 pagesMedi AssistRishi VermaNo ratings yet
- REV - Outpatient Claim Form - AIADocument2 pagesREV - Outpatient Claim Form - AIAYen SylvaniNo ratings yet
- REV - Inpatient Claim Form - AIADocument2 pagesREV - Inpatient Claim Form - AIAYen SylvaniNo ratings yet
- Statement of Claim Form (OP IP CLAIM) (Hospitalization)Document1 pageStatement of Claim Form (OP IP CLAIM) (Hospitalization)Dreyfus MicianoNo ratings yet
- I Health CareDocument1 pageI Health Caredisk_la_poduNo ratings yet
- Hospitalization Reimbursment Claim FormDocument4 pagesHospitalization Reimbursment Claim FormFarhan aliNo ratings yet
- 1 Claim FormDocument36 pages1 Claim Formkarmayukh1No ratings yet
- GMC Claim Form How To File A ClaimDocument4 pagesGMC Claim Form How To File A ClaimtweetknotNo ratings yet
- Hospital Cash Claim FormDocument5 pagesHospital Cash Claim FormVivek UmbreNo ratings yet
- Hospitalisation Claim Form: Borang Tuntutan HospitalDocument2 pagesHospitalisation Claim Form: Borang Tuntutan HospitalMohd Azizee Bin SukorNo ratings yet
- Gulfcare Insurancec Claim FormDocument1 pageGulfcare Insurancec Claim FormrishijaveriNo ratings yet
- Adamjee In-Patient Claim Reimbursement FormDocument2 pagesAdamjee In-Patient Claim Reimbursement Formhashamqazi100% (1)
- Claim - Form - MediassitDocument4 pagesClaim - Form - MediassitKashish BangaloreNo ratings yet
- Hospital Treatment Form: Anumediclaim PoliciesDocument1 pageHospital Treatment Form: Anumediclaim PoliciesSubhadip MaityNo ratings yet
- Head Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.Document5 pagesHead Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.gaddipati_ramuNo ratings yet
- Pre Authorization FormDocument2 pagesPre Authorization Formdisk_la_poduNo ratings yet
- Claim Form Page1 & 2Document2 pagesClaim Form Page1 & 2anwarshahphd2021No ratings yet
- HMRM RECORD DoccDocument13 pagesHMRM RECORD DoccBharath BeeNo ratings yet
- CuepacscareDocument2 pagesCuepacscarefazudliNo ratings yet
- In-Patient Claim Form: (To Be Filled by Claimant Employee)Document2 pagesIn-Patient Claim Form: (To Be Filled by Claimant Employee)Khan LalaNo ratings yet
- Form 2Document1 pageForm 2info.arnts100% (1)
- QIC Claim Form ReimbursementDocument1 pageQIC Claim Form ReimbursementJec Amrac25% (4)
- Health Suraksha Claim FormDocument2 pagesHealth Suraksha Claim FormAnna MalaiNo ratings yet
- Mumbai Claim FormDocument5 pagesMumbai Claim FormsunsangraNo ratings yet
- Attending Physicians Statement Crisis Cover Muscular Dystrophy - 041222Document2 pagesAttending Physicians Statement Crisis Cover Muscular Dystrophy - 041222laraNo ratings yet
- Medicare Insurance Claim Form: PolicyholderDocument2 pagesMedicare Insurance Claim Form: PolicyholdertagashiiNo ratings yet
- OPD Claim Form - IGI GeneralDocument1 pageOPD Claim Form - IGI GeneralAmeen Khan NiaziNo ratings yet
- 08 Claim FormDocument4 pages08 Claim Formanurag1309No ratings yet
- BSIB GHS Claim FormDocument3 pagesBSIB GHS Claim FormmuhsinmohammedNo ratings yet
- Ahmedabad Claim FormDocument5 pagesAhmedabad Claim FormFirdaus PanthakyNo ratings yet
- Lonpac Maid Medical ClaimDocument3 pagesLonpac Maid Medical ClaimYl EdianonNo ratings yet
- OVHC Claim Form 102017 PDFDocument3 pagesOVHC Claim Form 102017 PDFtarmudiNo ratings yet
- Reimbursement Reimbursement Reimbursement Claim Form Claim FormDocument2 pagesReimbursement Reimbursement Reimbursement Claim Form Claim FormKris ArceoNo ratings yet
- SG Worldcare Pre AuthorisationDocument3 pagesSG Worldcare Pre Authorisationbernardlim86No ratings yet
- Hospitalisation Claim FormsDocument6 pagesHospitalisation Claim FormspritamNo ratings yet
- Preauthorization Request Form - FinalDocument3 pagesPreauthorization Request Form - FinalRiya GhayelNo ratings yet
- OIC Claim FormDocument4 pagesOIC Claim FormPrashant SinghNo ratings yet
- Nas Reimbursement Claim FormDocument2 pagesNas Reimbursement Claim Formerika100% (1)
- Proposal Form Ashakiran PDFDocument6 pagesProposal Form Ashakiran PDFSreejith Rajendran PillaiNo ratings yet
- EnglishDocument10 pagesEnglishsimonklkamNo ratings yet
- AXA Reimbursement Claim FormDocument2 pagesAXA Reimbursement Claim Formrajkamal eshwarNo ratings yet
- Intellicare Reimbursement Form UPDATEDDocument2 pagesIntellicare Reimbursement Form UPDATEDPhilip Sardan100% (3)
- Medical CliamDocument2 pagesMedical Cliamsgowda64No ratings yet
- Medical Insurance Hospitalisation Surgical Claim FormDocument2 pagesMedical Insurance Hospitalisation Surgical Claim FormAustin KeungNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- A Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsFrom EverandA Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsNo ratings yet
- Aryan Nursing FormDocument3 pagesAryan Nursing FormFarhan AliNo ratings yet
- Electronic Ticket Receipt, January 06 For MR BADARUDDIN SOLANGIDocument3 pagesElectronic Ticket Receipt, January 06 For MR BADARUDDIN SOLANGIFarhan AliNo ratings yet
- Certificate FormDocument2 pagesCertificate FormFarhan AliNo ratings yet
- New Microsoft Office Publisher DocumentDocument1 pageNew Microsoft Office Publisher DocumentFarhan AliNo ratings yet
- Erpoc CmeDocument20 pagesErpoc CmeSharon J StephenNo ratings yet
- Fertilitas AnovulatoriDocument17 pagesFertilitas AnovulatoriAnonymous hXh1WNSZwNo ratings yet
- Homoeopathic Management of Ovarian Cyst - A Case RDocument7 pagesHomoeopathic Management of Ovarian Cyst - A Case RB. B.No ratings yet
- Kochi EchsDocument10 pagesKochi EchsDeepak KarnavarNo ratings yet
- Infertility InvestigationDocument13 pagesInfertility InvestigationMella MadsprNo ratings yet
- AbortionDocument35 pagesAbortionstudent_019No ratings yet
- Laparoscopic Hemihysterectomy On Rudimentary Non Communicating Functional Horn in Unicornuate Uterus On Virgo Intacta FULL PAPERDocument5 pagesLaparoscopic Hemihysterectomy On Rudimentary Non Communicating Functional Horn in Unicornuate Uterus On Virgo Intacta FULL PAPERJoko WinarnoNo ratings yet
- Screening For Female Genital Tract MalignancyDocument40 pagesScreening For Female Genital Tract MalignancyLili Uisa Rahmasari100% (1)
- Feeding of Healthy Newborn BabiesDocument37 pagesFeeding of Healthy Newborn BabiesSulfie HarsNo ratings yet
- Chiranjeevi Jaipur HospitalDocument13 pagesChiranjeevi Jaipur HospitalseyedbrothersNo ratings yet
- Negative IonDocument2 pagesNegative IonDekzie Flores MimayNo ratings yet
- Science 10 Module 1 3qDocument7 pagesScience 10 Module 1 3qDionil CabilanNo ratings yet
- Natural Family Planning MethodsDocument9 pagesNatural Family Planning MethodsJeff LibaoNo ratings yet
- Displacement of UtreusDocument13 pagesDisplacement of UtreusswethashakiNo ratings yet
- Final - Sustainability and Affordabilty of Menstrual ProductsDocument1 pageFinal - Sustainability and Affordabilty of Menstrual Productsjennalynmanreza59No ratings yet
- 2014 - HSC Core 3 - Parenting and Caring Student BookletDocument50 pages2014 - HSC Core 3 - Parenting and Caring Student Bookletapi-262253799No ratings yet
- Endoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and ComplicationsDocument16 pagesEndoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and Complicationsselatur100% (1)
- 312 - Breast & Testicular Self-ExaminationDocument2 pages312 - Breast & Testicular Self-Examinationjocieangelmendoza01No ratings yet
- Physiology of Female Reproductive SystemDocument22 pagesPhysiology of Female Reproductive Systemswera zainabNo ratings yet
- Hysteroscopic Fallopian Tube Recanalization Using A Exible Guide Cannula and Hydrophilic Guide WireDocument5 pagesHysteroscopic Fallopian Tube Recanalization Using A Exible Guide Cannula and Hydrophilic Guide WireAswathy KumaranNo ratings yet
- Penggunaan Jus Kulit Buah Naga Untuk Mengatasi Nyeri Saat Menstruasi (Dismenorea)Document6 pagesPenggunaan Jus Kulit Buah Naga Untuk Mengatasi Nyeri Saat Menstruasi (Dismenorea)ayun manisNo ratings yet
- Benign Breast DiseasesDocument35 pagesBenign Breast DiseasesBhim Nath KharelNo ratings yet
- Learning Journal (Unit 8) English CompositionDocument5 pagesLearning Journal (Unit 8) English CompositionAnna AkoladeNo ratings yet
- Screening For Cervical Cancer - UpToDateDocument40 pagesScreening For Cervical Cancer - UpToDateEvelin AlmeidaNo ratings yet
- Department of Education: Learning Activity Sheet in Science 6Document4 pagesDepartment of Education: Learning Activity Sheet in Science 6Tampok ES (Region III - Bulacan)No ratings yet
- Menstrual Cycle Graphing LabDocument3 pagesMenstrual Cycle Graphing LabArkrayNo ratings yet
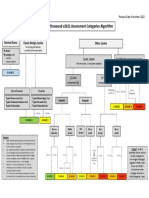
- O-RADS US v2022 Assessment Categories AlgorithmDocument1 pageO-RADS US v2022 Assessment Categories AlgorithmCarolina MagañaNo ratings yet
- Morning Report Fatimah Kamis, 1 Desember 2022Document8 pagesMorning Report Fatimah Kamis, 1 Desember 2022Kevin NoyaNo ratings yet
- EMQ Paper1with Answers Jan 2012Document9 pagesEMQ Paper1with Answers Jan 2012Hasan DahamshehNo ratings yet