Acute Kidney Injury
Acute Kidney Injury
Download as pdf or txt
You might also like
- Wilson Disease - Treatment and Prognosis - UpToDateDocument13 pagesWilson Disease - Treatment and Prognosis - UpToDatericanoy191No ratings yet
- The Urinary Sediment by UriSed Technology G.B. Fogazzi - G. GarigaliDocument123 pagesThe Urinary Sediment by UriSed Technology G.B. Fogazzi - G. GarigaliALMA ROSA PEREZ MORALES100% (2)
- Viteri2018 Prevalensi 5Document17 pagesViteri2018 Prevalensi 5adrian revoNo ratings yet
- AKI in SepsisDocument45 pagesAKI in SepsisIkeBundaAdellulaNo ratings yet
- Definingacutekidney Injury: Siddharth Verma,, John A. KellumDocument16 pagesDefiningacutekidney Injury: Siddharth Verma,, John A. KellumNicolas Peña RiveraNo ratings yet
- Craniosacral Care1Document6 pagesCraniosacral Care1Anonymous 7R6n0f9BY100% (2)
- Pediatric Acute Kidney Injury (AKI) Indications, Timing, and Choice of ModalityDocument32 pagesPediatric Acute Kidney Injury (AKI) Indications, Timing, and Choice of ModalityCarolineNo ratings yet
- Diagnosis and Management of Myocarditis in Child AHA 2021Document13 pagesDiagnosis and Management of Myocarditis in Child AHA 2021Carlos Peña PaterninaNo ratings yet
- Dka, Cerebral Edema, HhsDocument90 pagesDka, Cerebral Edema, HhsNazafNo ratings yet
- Nephrology and HypertensionDocument33 pagesNephrology and HypertensionCarlos HernándezNo ratings yet
- Inter'Medic CKDDocument31 pagesInter'Medic CKDMAHEJS HD100% (1)
- FINAL NephMadness 2023 Classroom Slides PDFDocument100 pagesFINAL NephMadness 2023 Classroom Slides PDFDIANA LAURA MUNOZ MONTES DE OCANo ratings yet
- AAH v2 Acute AsthmaDocument81 pagesAAH v2 Acute AsthmaEssa SmjNo ratings yet
- Heart Disease in Children 2018Document12 pagesHeart Disease in Children 2018Carlos Peña PaterninaNo ratings yet
- Pediatric Coag Disorders PDFDocument15 pagesPediatric Coag Disorders PDFFATIMA LAVADIANo ratings yet
- Chronic Dyspnea Afp20200501p542Document7 pagesChronic Dyspnea Afp20200501p542Philippe Ceasar C. BascoNo ratings yet
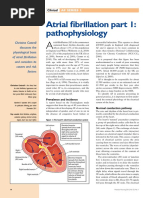
- Atrial Fibrilliation Part 1 Pathophysiology C CottrellDocument5 pagesAtrial Fibrilliation Part 1 Pathophysiology C CottrellA Farid WajdyNo ratings yet
- Pediatrics 2012 780 92Document15 pagesPediatrics 2012 780 92ERICKNo ratings yet
- BTS Sarcoidosis Clinical StatementDocument17 pagesBTS Sarcoidosis Clinical StatementDarrin WiebeNo ratings yet
- Initial Presentation and Management of Pediatric Heart FailureDocument7 pagesInitial Presentation and Management of Pediatric Heart FailurePrasenjitRaneNo ratings yet
- DIC in PregnancyDocument24 pagesDIC in PregnancySergio Alberto Sulub NavarreteNo ratings yet
- Pediatric Diabetes - 2022Document27 pagesPediatric Diabetes - 2022Samira tNo ratings yet
- Last Look Nephrology & Rheumatology (Medicine Must Know)Document43 pagesLast Look Nephrology & Rheumatology (Medicine Must Know)rohankananiNo ratings yet
- Onconephrology Core Curriculum 2023Document19 pagesOnconephrology Core Curriculum 2023jogutiro01100% (1)
- Alcoholic Hepatitis Diagnosis and ManagementDocument10 pagesAlcoholic Hepatitis Diagnosis and ManagementGW GeistNo ratings yet
- AAFP DRC and DiabetesDocument9 pagesAAFP DRC and DiabetesThaysa LimaNo ratings yet
- Platelet Disorders: Practice GapsDocument14 pagesPlatelet Disorders: Practice GapsMichelleHanNo ratings yet
- 07 Pediatrics in Review July20 PDFDocument66 pages07 Pediatrics in Review July20 PDFAndrea PederziniNo ratings yet
- TTN AafpDocument9 pagesTTN Aafpsiti nur rachmaniNo ratings yet
- Managing Hypertension Using Combination Therapy - AAFPDocument18 pagesManaging Hypertension Using Combination Therapy - AAFPtorome4979No ratings yet
- Management of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesDocument7 pagesManagement of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesdaypranitaNo ratings yet
- Case PediatricsDocument6 pagesCase PediatricsHarsh NimavatNo ratings yet
- Update On Diarrhea - Peds in Rev 2016Document12 pagesUpdate On Diarrhea - Peds in Rev 2016TriLightNo ratings yet
- Community-Acquired Pneumonia in Adults - Rapid Evidence ReviewDocument6 pagesCommunity-Acquired Pneumonia in Adults - Rapid Evidence ReviewpachomdNo ratings yet
- Nac 2017Document18 pagesNac 2017Nataly CortesNo ratings yet
- JR Ppi 3Document8 pagesJR Ppi 3Bombong Nurpagino100% (1)
- A Timeline History of NephrologyDocument32 pagesA Timeline History of NephrologyxguerratNo ratings yet
- Management of COPD ExacerbationsDocument7 pagesManagement of COPD ExacerbationsAmalia Nurul UlumNo ratings yet
- 2nd Edition of Malaysian COPD Clinical Practice GuidelineDocument67 pages2nd Edition of Malaysian COPD Clinical Practice GuidelineFay Fanny FlanneryNo ratings yet
- Clinical Pracice Guideline For The Treatment of Pediatric Acute Gastroenteritis in The Outpatient SettingDocument8 pagesClinical Pracice Guideline For The Treatment of Pediatric Acute Gastroenteritis in The Outpatient SettingLaura Anghel-MocanuNo ratings yet
- Peripheral Neuropathy: Evaluation and Differential DiagnosisDocument8 pagesPeripheral Neuropathy: Evaluation and Differential DiagnosisBintu Searching-FriendNo ratings yet
- An Approach To Anemic PatientDocument79 pagesAn Approach To Anemic PatientHussain Azhar100% (1)
- NR March2014Document44 pagesNR March2014Susana Jacqueline Echeverria Muñoz100% (1)
- Assessment and Management of Acute Disseminated Encephalomyelitis (ADEM) in The Pediatric Patient - s40272-021-00441-7 21.56.43Document9 pagesAssessment and Management of Acute Disseminated Encephalomyelitis (ADEM) in The Pediatric Patient - s40272-021-00441-7 21.56.43Neni NirmalaNo ratings yet
- Inotropic and Vasoactive Drugs in Pediatric ICUDocument6 pagesInotropic and Vasoactive Drugs in Pediatric ICUCandy RevolloNo ratings yet
- Infective EndocarditisDocument18 pagesInfective EndocarditisLee Foo WengNo ratings yet
- Diagnosis of Gastrointestinal Bleeding in AdultsDocument8 pagesDiagnosis of Gastrointestinal Bleeding in AdultsSaeed Al-YafeiNo ratings yet
- Noel A. Villanueva, MD, FPCP, FPSNDocument62 pagesNoel A. Villanueva, MD, FPCP, FPSNagilNo ratings yet
- Use of C-Reactive Protein and Ferritin Biomarkers in Daily Pediatric PracticeDocument14 pagesUse of C-Reactive Protein and Ferritin Biomarkers in Daily Pediatric PracticeMichelleHanNo ratings yet
- RAAS CKD ProgressionDocument86 pagesRAAS CKD ProgressionNikesh DoshiNo ratings yet
- Anemia of PrematurityDocument14 pagesAnemia of PrematurityMariel HuamancayoNo ratings yet
- Ksap 3Document92 pagesKsap 3shahid mahmoodNo ratings yet
- Evaluation and Treatment of Nonmonosymptomatic EnuresisDocument11 pagesEvaluation and Treatment of Nonmonosymptomatic EnuresisastrogliaNo ratings yet
- Thyroid NodulesDocument7 pagesThyroid Noduleshossein kasiriNo ratings yet
- The Neurologic ExamDocument7 pagesThe Neurologic ExamGabriel ArizaNo ratings yet
- Urticaria AnaphylaxisDocument12 pagesUrticaria AnaphylaxismanchalunaNo ratings yet
- Glomerulonephritis Dwi Fin PDFDocument108 pagesGlomerulonephritis Dwi Fin PDFOvyanda Eka MItraNo ratings yet
- Gamapatia Monoclonal Significado RenalDocument11 pagesGamapatia Monoclonal Significado RenalAlejandroNarvaezNo ratings yet
- Therapeutic Hypothermia - Principles, Indications, Practical ApplicationFrom EverandTherapeutic Hypothermia - Principles, Indications, Practical ApplicationNo ratings yet
- Acrf CDocument70 pagesAcrf CHussain AzharNo ratings yet
- College of Nursing: Civil HospitalDocument15 pagesCollege of Nursing: Civil HospitalDipal Jignesh PatelNo ratings yet
- Lo Week 2-1Document8 pagesLo Week 2-1Martien Silviandy SetiawanNo ratings yet
- (Optima) Sopem Optima THT-KL Sep'19Document333 pages(Optima) Sopem Optima THT-KL Sep'19Ory LarasNo ratings yet
- Diagnosing Migraine in Primary Care Practice-Simple Tips To Overcome Difficult Clinical ScenariosDocument3 pagesDiagnosing Migraine in Primary Care Practice-Simple Tips To Overcome Difficult Clinical ScenariosDara Daula MumtazaNo ratings yet
- AmelogenezaDocument9 pagesAmelogenezaRuxandra FitaNo ratings yet
- Pathology Handwritten NotesDocument210 pagesPathology Handwritten Notespangulvedant46No ratings yet
- Management of Migraine OET ReadingDocument21 pagesManagement of Migraine OET ReadingKush Gurung67% (6)
- DR Agus Sulistyono, SpOG, Subsp KFM - Breech Presentation and After Coming HeadDocument47 pagesDR Agus Sulistyono, SpOG, Subsp KFM - Breech Presentation and After Coming Headklinikharapanbunda61No ratings yet
- Activ - Final - Danilo QuinteroDocument4 pagesActiv - Final - Danilo QuinterodaniloNo ratings yet
- Septic Shock Simulation: ICU After SurgeryDocument4 pagesSeptic Shock Simulation: ICU After SurgeryMorvinNo ratings yet
- PHLN TNLDocument5 pagesPHLN TNLShoyuna PutriNo ratings yet
- Dun Nick 2008Document2 pagesDun Nick 2008Dian Andi PrastiyoNo ratings yet
- Ethical of NursesDocument16 pagesEthical of NursesAida Ida100% (1)
- Cochlear Implant in A Developing CountryDocument6 pagesCochlear Implant in A Developing CountryWaqar AhmedNo ratings yet
- HSE-CA - StyreneDocument3 pagesHSE-CA - StyreneRobert PilloraNo ratings yet
- ZWEIHANDER ATTACK Flow ChartDocument3 pagesZWEIHANDER ATTACK Flow ChartJosh SalyersNo ratings yet
- FDAR Charting NICUDocument1 pageFDAR Charting NICUYuvi LuardoNo ratings yet
- Tuberculosis - StatPearls - NCBI BookshelfDocument10 pagesTuberculosis - StatPearls - NCBI BookshelfDhany karubuyNo ratings yet
- CASE DISCUSSION - ASCITES, TRANSUDATE Vs EXCUDATE AND SHOCKDocument51 pagesCASE DISCUSSION - ASCITES, TRANSUDATE Vs EXCUDATE AND SHOCKAparna ValsanNo ratings yet
- ELISA Test For The Quantitative Determination of Follicle Stimulating Hormone (FSH) in Human SerumDocument2 pagesELISA Test For The Quantitative Determination of Follicle Stimulating Hormone (FSH) in Human SerumLemi MaluluNo ratings yet
- Herbs BookDocument46 pagesHerbs BookLay RaykundaliaNo ratings yet
- Management of Open Bite: Dr. Madhura Jayant Pednekar Iii MdsDocument75 pagesManagement of Open Bite: Dr. Madhura Jayant Pednekar Iii MdsDrKamran MominNo ratings yet
- Ophthalmology Emergencies HandoutDocument9 pagesOphthalmology Emergencies HandoutMutiara SazkiaNo ratings yet
- CAGULADA (BSN 2 - NB) Expanded Program On Immunization ProjectDocument1 pageCAGULADA (BSN 2 - NB) Expanded Program On Immunization ProjectTrisha Mikaela CaguladaNo ratings yet
- Ciulla HemastasisDocument12 pagesCiulla HemastasisLancer BlazeNo ratings yet
- Cancer Take Papaya As Often As You CanDocument6 pagesCancer Take Papaya As Often As You Canchampak100% (1)
- Non-Pharmacological Treatment of DepressionDocument38 pagesNon-Pharmacological Treatment of Depressionjuan_bacha_1No ratings yet
- Canine Infectious Diseases PDFDocument149 pagesCanine Infectious Diseases PDFSándor Holdas67% (3)
- PDF Takayasu Arteritis 2 PDFDocument5 pagesPDF Takayasu Arteritis 2 PDFPadmaja PriyadarshiniNo ratings yet
- Homeo First AidDocument4 pagesHomeo First AidRamesh KumarNo ratings yet