1538 Exam 5 Intracranial
1538 Exam 5 Intracranial
Download as docx, pdf, or txt
You might also like
- Ati Comprehensive Predictor 2019 ADocument51 pagesAti Comprehensive Predictor 2019 Aanahmburu966No ratings yet
- Fatime Sanogo Vsim Steps - HTMLDocument6 pagesFatime Sanogo Vsim Steps - HTMLJhunnieEy ReyesNo ratings yet
- ATI IV TherapyDocument8 pagesATI IV Therapylisa100% (1)
- Traumaticbraininjury: An Overview of Epidemiology, Pathophysiology, and Medical ManagementDocument26 pagesTraumaticbraininjury: An Overview of Epidemiology, Pathophysiology, and Medical ManagementAndre SiahaanNo ratings yet
- Fluids and ElectrolytesDocument128 pagesFluids and Electrolytesmd6ztpydckNo ratings yet
- Intrapartum PeriodDocument19 pagesIntrapartum Periodanon_915924422No ratings yet
- Psychiatry NotesDocument8 pagesPsychiatry NotesAabraNo ratings yet
- Reponse of Brain Tissue To Trauma: Intracranial PressureDocument29 pagesReponse of Brain Tissue To Trauma: Intracranial Pressurevijaykadam_ndaNo ratings yet
- Fall 2023, 1R8 - Maternal Newborn Study Guide (Comprehensive)Document16 pagesFall 2023, 1R8 - Maternal Newborn Study Guide (Comprehensive)Tia Liveandlearn0% (1)
- CH 14 Wardand HInsley Maternity Power PointDocument25 pagesCH 14 Wardand HInsley Maternity Power PointJonalyn ChewacheoNo ratings yet
- Fetal MonitorDocument8 pagesFetal Monitoriqbal hedkeyNo ratings yet
- Critical CareDocument21 pagesCritical Carepaulzilicous.artNo ratings yet
- Immune SystemDocument19 pagesImmune Systempaulzilicous.artNo ratings yet
- All ConditionsDocument6 pagesAll ConditionsJoya Ruben CamposNo ratings yet
- Dysrhythmias: Se Admin Anticoagulante, Cardioversion As PrescribedDocument10 pagesDysrhythmias: Se Admin Anticoagulante, Cardioversion As Prescribedyaneidys perezNo ratings yet
- Med AdministrationDocument14 pagesMed Administrationpaulzilicous.artNo ratings yet
- Health Assessment: NeuroDocument34 pagesHealth Assessment: Neuroiamjennykim76No ratings yet
- Administration Eye DropsDocument13 pagesAdministration Eye DropsyaraNo ratings yet
- Hematologic System2Document70 pagesHematologic System2Jesus Mario LopezNo ratings yet
- Pressure Sore or Decubitus Ulcer or Bed SoreDocument20 pagesPressure Sore or Decubitus Ulcer or Bed SorePrecious Blessing100% (1)
- Worksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Document3 pagesWorksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Emerald SpanglerNo ratings yet
- Admission NotesDocument16 pagesAdmission NotesCaisar Dewi MaulinaNo ratings yet
- The Respiratory SystemDocument40 pagesThe Respiratory SystemAdriana ChasiguanoNo ratings yet
- Dexmedetomidine Drug SummaryDocument3 pagesDexmedetomidine Drug SummarySydney JenningsNo ratings yet
- Chapter 19 Introduction To Nerves and The Nervous SystemDocument27 pagesChapter 19 Introduction To Nerves and The Nervous SystemFugado Mica illaNo ratings yet
- Diets and NutritionDocument19 pagesDiets and Nutritionpaulzilicous.artNo ratings yet
- PREPUMASTERKEY (Repaired)Document2,031 pagesPREPUMASTERKEY (Repaired)surviving nursing schoolNo ratings yet
- Fluids and Electrolytes: Irene L. Gardiner, MDDocument48 pagesFluids and Electrolytes: Irene L. Gardiner, MDGabriel Carlo FranciscoNo ratings yet
- ISBAR Worksheet Olivia Jones Jasgou1752Document1 pageISBAR Worksheet Olivia Jones Jasgou1752Jasmyn Rose100% (1)
- ClinicalOwl-PharmacologyLastMinuteNotesFullBundleDocument121 pagesClinicalOwl-PharmacologyLastMinuteNotesFullBundleShammah Cecilia NassaliNo ratings yet
- 6 Nursing Assessment MnemonicsDocument4 pages6 Nursing Assessment MnemonicsEunice Angela FulguerasNo ratings yet
- Task Delegations For NclexDocument3 pagesTask Delegations For Nclexjenn_028No ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Shock, Sepsis, and Multiple Organ Dysfunction Syndrome Key Points ShockDocument5 pagesLewis: Medical-Surgical Nursing, 10 Edition: Shock, Sepsis, and Multiple Organ Dysfunction Syndrome Key Points Shockann forsyNo ratings yet
- If Symptoms Are Not Recognized and Treated in A Timely Manner, Complications That CharlieDocument5 pagesIf Symptoms Are Not Recognized and Treated in A Timely Manner, Complications That Charliesalman ahmedNo ratings yet
- Pediatric Nursing Edited)Document1 pagePediatric Nursing Edited)Dominique RamosNo ratings yet
- TransesDocument5 pagesTransesTintin HonraNo ratings yet
- 6Document100 pages6layanebfspNo ratings yet
- Nervous System AlterationsDocument45 pagesNervous System AlterationsMajesty ParkerNo ratings yet
- Risk Factors Pathophysiology Concept Potential ComplicationsDocument1 pageRisk Factors Pathophysiology Concept Potential ComplicationsiamdarnNo ratings yet
- Ob Final ReviewDocument13 pagesOb Final Reviewraquel maniegoNo ratings yet
- Fluids and ElectrolytesDocument9 pagesFluids and Electrolytespaulzilicous.artNo ratings yet
- Fundamentals Note TakingDocument3 pagesFundamentals Note TakingJero BallesterosNo ratings yet
- Hepatobiliary Disorders: Katrina Saludar Jimenez, R. NDocument42 pagesHepatobiliary Disorders: Katrina Saludar Jimenez, R. NKatrinaJimenezNo ratings yet
- Care of Patients With Noninfectious Lower Respiratory ProblemsDocument46 pagesCare of Patients With Noninfectious Lower Respiratory Problemsjrflores1284No ratings yet
- Draft: Jurisprudence Learning Module & ExaminationDocument45 pagesDraft: Jurisprudence Learning Module & ExaminationDeepanshi RajputNo ratings yet
- Chapter 18 Intrapartum Nursing AssessmentDocument4 pagesChapter 18 Intrapartum Nursing AssessmentMary LowryNo ratings yet
- Solutions For Maternity, Newborn, and WomenS Health Nursing 2nd Us Edition by O'MearaDocument19 pagesSolutions For Maternity, Newborn, and WomenS Health Nursing 2nd Us Edition by O'Mearat.estbankyNo ratings yet
- Memory Trick For NCLEXDocument60 pagesMemory Trick For NCLEXpaulzilicous.artNo ratings yet
- CH 14 Antepartum Nursing Assessment NotesDocument8 pagesCH 14 Antepartum Nursing Assessment NotesMary LowryNo ratings yet
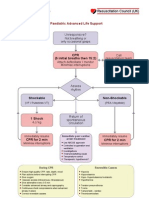
- PalsDocument1 pagePalslordroentgenNo ratings yet
- Fundamental QuestionsDocument5 pagesFundamental QuestionsSheshe0% (3)
- Nervous SystemDocument23 pagesNervous SystemAlliyah SalindoNo ratings yet
- Clinical Case Study - Online Discussion Form Fall 2020-1Document14 pagesClinical Case Study - Online Discussion Form Fall 2020-1Sabrina Odies100% (1)
- Ob Ati StudyDocument22 pagesOb Ati Studylpirman0580% (5)
- A-T-I Endocrine NotesDocument3 pagesA-T-I Endocrine NotesKelseyAnnBarnesNo ratings yet
- Commonly Asked Emergency DrugsDocument17 pagesCommonly Asked Emergency DrugsThierd Cañete III100% (1)
- Approach To Acutely Ill PatientDocument22 pagesApproach To Acutely Ill PatientSarah RamliNo ratings yet
- Dysrhythmia Instructor 2018 2 PDFDocument105 pagesDysrhythmia Instructor 2018 2 PDFtvrossyNo ratings yet
- Drugs Affecting Blood PressureDocument54 pagesDrugs Affecting Blood PressureJeremy VivitNo ratings yet
- 1538 Exam 2 Human DevelpomentDocument20 pages1538 Exam 2 Human DevelpomentJade EdanoNo ratings yet
- 1538 Exam 1 ReproductionDocument22 pages1538 Exam 1 ReproductionJade EdanoNo ratings yet
- 1538 Exam 2 Human DevelpomentDocument19 pages1538 Exam 2 Human DevelpomentJade EdanoNo ratings yet
- 1538 Exam 4 Cell Reg & GriefDocument35 pages1538 Exam 4 Cell Reg & GriefJade EdanoNo ratings yet
- Pediatric Nursing Post TestDocument24 pagesPediatric Nursing Post Testjohneric010408No ratings yet
- The Use of Svo2 Monitoring in The Cardiac Intensive Care UnitDocument60 pagesThe Use of Svo2 Monitoring in The Cardiac Intensive Care UnitAnthony RossiNo ratings yet
- HTLV ArcDocument6 pagesHTLV Arctesteste testeNo ratings yet
- Triada de CharcotDocument1 pageTriada de Charcotdanitza pilcoNo ratings yet
- NCP 2 Addison's DiseaseDocument4 pagesNCP 2 Addison's DiseaseRenee RoSeNo ratings yet
- Intertrigo and Secondary Skin InfectionsDocument5 pagesIntertrigo and Secondary Skin Infectionskhalizamaulina100% (1)
- Complete Download Revmed 300 Sbas In Clinical Specialties 1st Edition Lasith Ranasinghe PDF All ChaptersDocument75 pagesComplete Download Revmed 300 Sbas In Clinical Specialties 1st Edition Lasith Ranasinghe PDF All Chaptersmtyuturrudho100% (2)
- Kidney Failure (Reference Summary) : AnatomyDocument3 pagesKidney Failure (Reference Summary) : AnatomyUSMP FN ARCHIVOSNo ratings yet
- Hepatitis B Profile InterpretationDocument43 pagesHepatitis B Profile InterpretationSAMMYNo ratings yet
- Q.P. CODE: 223010 Reg. No: ... Second Semester B.SC Nursing Degree Regular/Supplementary Examinations November 2023 Nursing Foundations (I & II)Document2 pagesQ.P. CODE: 223010 Reg. No: ... Second Semester B.SC Nursing Degree Regular/Supplementary Examinations November 2023 Nursing Foundations (I & II)usatesting21No ratings yet
- Algorithm Febrile SeizuresDocument32 pagesAlgorithm Febrile SeizuresSi Puput100% (1)
- Case Report: Hemophilia ADocument20 pagesCase Report: Hemophilia ABintang Ruth Cecilia FebrinaNo ratings yet
- BrochureDocument2 pagesBrochureapi-238213388No ratings yet
- Staff Health Form: Demographic ProfileDocument3 pagesStaff Health Form: Demographic ProfileAaron Jay MondayaNo ratings yet
- Endometrial CarcinomaDocument10 pagesEndometrial CarcinomaAlbert Jonathan PelleNo ratings yet
- Acute Kidney Injury in Interstitial Nephritis.5 PDFDocument7 pagesAcute Kidney Injury in Interstitial Nephritis.5 PDFFIA SlotNo ratings yet
- Giray, Noriel N. 3b (Pre-Activity)Document10 pagesGiray, Noriel N. 3b (Pre-Activity)Noriel GirayNo ratings yet
- (BEVMED) Quiz 1 2nd Semester AY 2018-2019Document2 pages(BEVMED) Quiz 1 2nd Semester AY 2018-2019KAREN MAE PADILLANo ratings yet
- Test Editor 1Document213 pagesTest Editor 1Ibrahim AbueltaifNo ratings yet
- Assignment 5Document2 pagesAssignment 5SutangaNo ratings yet
- Genetics of Hearing Loss DR NayyarDocument56 pagesGenetics of Hearing Loss DR NayyarSuprit SnNo ratings yet
- PNLE - Community Health Nursing Exam 2 - RNpediaDocument15 pagesPNLE - Community Health Nursing Exam 2 - RNpediaJoshua UveroNo ratings yet
- NBME 19 BreakdownDocument23 pagesNBME 19 BreakdownDaniel SotoNo ratings yet
- Cardiac Meds Sheet1Document1 pageCardiac Meds Sheet1Amna Kazmi Shehzad100% (1)
- Risk For BleedingDocument2 pagesRisk For Bleedingirithel markasNo ratings yet
- Maxillary Sinus in Health and DiseaseDocument36 pagesMaxillary Sinus in Health and Diseasedaw022No ratings yet
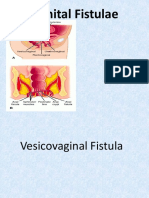
- Fistula GenitaliaDocument35 pagesFistula GenitaliaFifi FruitasariNo ratings yet
- Drug Template CHPT 30-33Document2 pagesDrug Template CHPT 30-33Jamie SimsNo ratings yet
- Genogram Diagram - Part 1Document1 pageGenogram Diagram - Part 1api-609737816No ratings yet