Pilot Testing Complex Care Coordination
Pilot Testing Complex Care Coordination
Download as pdf or txt
You might also like
- Comprehensive Health Care ServicesDocument18 pagesComprehensive Health Care ServicesHamisu Tafashiya100% (1)
- NCP For Disturbed Sleep Pattern and Impaired ComfortDocument7 pagesNCP For Disturbed Sleep Pattern and Impaired ComfortMaila Joy Pring Fuentes50% (2)
- Mushak-9.1 VAT Return On 19.NOV.2020 PDFDocument6 pagesMushak-9.1 VAT Return On 19.NOV.2020 PDFApexBD01100% (1)
- EITC PresentationDocument11 pagesEITC PresentationAlvin ChangNo ratings yet
- Care For Elderly PDFDocument10 pagesCare For Elderly PDFDzulfiqarNo ratings yet
- Press Release 12-09 - New Study Raises Health and Safety Concerns inDocument3 pagesPress Release 12-09 - New Study Raises Health and Safety Concerns inhealthoregonNo ratings yet
- Sister Blessing Project.Document41 pagesSister Blessing Project.ayanfeNo ratings yet
- Family and Parental Decision Making When Choosing A Paediatric General Practice Service What Factors Mattered MostDocument19 pagesFamily and Parental Decision Making When Choosing A Paediatric General Practice Service What Factors Mattered MoststarshineclinicinfoNo ratings yet
- Impact of Social Media On Nurses Service Delivery - EditedDocument14 pagesImpact of Social Media On Nurses Service Delivery - EditedMaina PeterNo ratings yet
- STACEY DLIS 20th MAyDocument22 pagesSTACEY DLIS 20th MAyStaceyNo ratings yet
- Thesis Health Care ReformDocument5 pagesThesis Health Care ReformKate Campbell100% (2)
- RESEARCHDocument16 pagesRESEARCHGloria Marisse BaclayNo ratings yet
- A Patient Information Management System (PIMS) For Health Care: A Case of Kampala International University Teaching Hospital, Ishaka-Bushenyi, UgandaDocument6 pagesA Patient Information Management System (PIMS) For Health Care: A Case of Kampala International University Teaching Hospital, Ishaka-Bushenyi, UgandaNamata Racheal SsempijjaNo ratings yet
- A Pilot Cohort Analytic Study of Family Integrated Care in A Canadian Neonatal Intensive Care UnitDocument8 pagesA Pilot Cohort Analytic Study of Family Integrated Care in A Canadian Neonatal Intensive Care Unit신정민No ratings yet
- 2005 Anonimo Linking Health Care InformationDocument73 pages2005 Anonimo Linking Health Care Informationsicario01No ratings yet
- Proposal For AbDocument6 pagesProposal For AbAfolabi OluwafemiNo ratings yet
- Innovation Awards Round 2 Batch 1Document7 pagesInnovation Awards Round 2 Batch 1iggybauNo ratings yet
- SSRN Id1992551Document28 pagesSSRN Id1992551jpkumarNo ratings yet
- Role of Health Surveys in National Health Information Systems: Best-Use ScenariosDocument28 pagesRole of Health Surveys in National Health Information Systems: Best-Use ScenariosazfarNo ratings yet
- Building Primary Care Research Infrastructure (2011)Document2 pagesBuilding Primary Care Research Infrastructure (2011)Jasmik SinghNo ratings yet
- ZERRUDO Funda-Endterm-Lesson-1-For-StudentsDocument11 pagesZERRUDO Funda-Endterm-Lesson-1-For-StudentsGlen DaleNo ratings yet
- Annotated Bibliography PDFDocument10 pagesAnnotated Bibliography PDFapi-296283530No ratings yet
- Drug Information Bulletin (Electronic) : Number: 32 20 November 2010Document4 pagesDrug Information Bulletin (Electronic) : Number: 32 20 November 2010amritaryaaligarghNo ratings yet
- Nursing Informatics: Bachelor of Science in NursingDocument5 pagesNursing Informatics: Bachelor of Science in NursingGiselle EstoquiaNo ratings yet
- TerrDocument3 pagesTerramsaline hutahaeanNo ratings yet
- Discharge Communication Practices in Pediatric Emergency Care - A Systematic Review and Narrative SynthesisDocument28 pagesDischarge Communication Practices in Pediatric Emergency Care - A Systematic Review and Narrative Synthesisleivaherre10No ratings yet
- Art 3A10.1186 2Fs12912 015 0097 3Document13 pagesArt 3A10.1186 2Fs12912 015 0097 3S LaimeheriwaNo ratings yet
- 404 03 Mentalhealth ES ENGDocument9 pages404 03 Mentalhealth ES ENGritanlanskyNo ratings yet
- MIDTERM Worksheet1Document5 pagesMIDTERM Worksheet1Jade GordoncilloNo ratings yet
- MIDTERM Worksheet1Document5 pagesMIDTERM Worksheet1Jade GordoncilloNo ratings yet
- Understanding The Factors Influencing The Implementation of Participatory Interventions To Improve Care Coordination. An Analytical Framework Based On An Evaluation in Latin AmericaDocument11 pagesUnderstanding The Factors Influencing The Implementation of Participatory Interventions To Improve Care Coordination. An Analytical Framework Based On An Evaluation in Latin AmericaGonzalo PachecoNo ratings yet
- Which Procedures Are Performed by General Internists Practicing Primary Care in Germany? - A Cross-Sectional StudyDocument10 pagesWhich Procedures Are Performed by General Internists Practicing Primary Care in Germany? - A Cross-Sectional StudytenzinthanggaNo ratings yet
- Pediatrics 2013 Clancy S210 4Document7 pagesPediatrics 2013 Clancy S210 4Timothy Eduard A. SupitNo ratings yet
- UHC Hesitancy by Mugas (2023)Document13 pagesUHC Hesitancy by Mugas (2023)Jet MasaNo ratings yet
- What's Next? Evidence-Based Nursing: How Far Have We Come?Document4 pagesWhat's Next? Evidence-Based Nursing: How Far Have We Come?benjaminshahzadNo ratings yet
- JURNAL Komunikasi Tren IssueDocument4 pagesJURNAL Komunikasi Tren Issuekelvin pradanaNo ratings yet
- Nursing Informatics in CanadaDocument8 pagesNursing Informatics in CanadaAb Staholic BoiiNo ratings yet
- Mhealth: Technology For Nursing Practice, Education, and ResearchDocument12 pagesMhealth: Technology For Nursing Practice, Education, and ResearchNandhini ShreeNo ratings yet
- Best Practices in Intercultural HealthDocument6 pagesBest Practices in Intercultural HealthSalud InmigrantesNo ratings yet
- Develop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenDocument8 pagesDevelop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenpsicoterapiavaldiviaNo ratings yet
- A Review of Literature On Access To Primary Health CareDocument5 pagesA Review of Literature On Access To Primary Health Careafmzsbzbczhtbd100% (1)
- Medical Liability GrantsDocument9 pagesMedical Liability GrantsCarter WoodNo ratings yet
- 110 A Midterm NotesDocument37 pages110 A Midterm NotesPark Yoon AeNo ratings yet
- Using Systems Thinking Methodologies To Address.2Document8 pagesUsing Systems Thinking Methodologies To Address.2tamru4239No ratings yet
- Case Studies Lecture 22042024 033948pmDocument7 pagesCase Studies Lecture 22042024 033948pmdrumerchheenaNo ratings yet
- HTM 680 OpendoorfamilymedicalcentercasestudyDocument6 pagesHTM 680 Opendoorfamilymedicalcentercasestudyapi-307874398No ratings yet
- Nursing Tics in EuropeDocument12 pagesNursing Tics in EuropeLiezl Mae MacaraegNo ratings yet
- Chapter 1 IntroductionDocument12 pagesChapter 1 IntroductionaerofanzNo ratings yet
- 10 1016@j Aogh 2017 09 005 PDFDocument6 pages10 1016@j Aogh 2017 09 005 PDFWaldi RahmanNo ratings yet
- 07 - Working With Health IT Systems - Unit 10 - HIT and Aspects of Patient-Centered Care - Lecture ADocument12 pages07 - Working With Health IT Systems - Unit 10 - HIT and Aspects of Patient-Centered Care - Lecture AHealth IT Workforce Curriculum - 2012No ratings yet
- Challenges and Barriers Faced by Home Care CentersDocument9 pagesChallenges and Barriers Faced by Home Care CentersAbdishakur Mohamud HassanNo ratings yet
- Tizon, R. - Assignment in NCM 112Document4 pagesTizon, R. - Assignment in NCM 112Royce Vincent TizonNo ratings yet
- Chapter 1-2 FosterDocument13 pagesChapter 1-2 FosterSuleiman ZakarNo ratings yet
- Introduction (Story1,2)Document6 pagesIntroduction (Story1,2)3500No ratings yet
- Nursing Informatics in CanadaDocument33 pagesNursing Informatics in CanadaKenNo ratings yet
- Standards and EHR InteroperabilityDocument26 pagesStandards and EHR InteroperabilityONC for Health Information TechnologyNo ratings yet
- Automated Pill Dispenser Nhs StudyDocument7 pagesAutomated Pill Dispenser Nhs StudyAdib Raza0% (1)
- Bommersbach (2021) - Mental Health Staff Perceptions of Improvement Opportunities Around Covid 19Document14 pagesBommersbach (2021) - Mental Health Staff Perceptions of Improvement Opportunities Around Covid 19Maximiliano AzconaNo ratings yet
- Improving Communication With Primary Care Physicians at The Time of Hospital DischargeDocument9 pagesImproving Communication With Primary Care Physicians at The Time of Hospital DischargeEmily MoriartyNo ratings yet
- Exploration of The Concept and Application of Home Care For Older Persons A Review of The LiteratureDocument61 pagesExploration of The Concept and Application of Home Care For Older Persons A Review of The LiteratureOnesiforus SopaterNo ratings yet
- Published Researches in The Year 2010Document16 pagesPublished Researches in The Year 2010hsrimediaNo ratings yet
- 2020 - Revisiting Health Information Technology ELSI Civid - 19Document17 pages2020 - Revisiting Health Information Technology ELSI Civid - 19Alberto Lecaros UrzúaNo ratings yet
- Cognitive Informatics: Reengineering Clinical Workflow for Safer and More Efficient CareFrom EverandCognitive Informatics: Reengineering Clinical Workflow for Safer and More Efficient CareKai ZhengNo ratings yet
- Health Care Transparency Should Be About Strategy, Not MarketingDocument3 pagesHealth Care Transparency Should Be About Strategy, Not MarketingRavi S GSRNo ratings yet
- Innovation Manager-JDDocument1 pageInnovation Manager-JDRavi S GSRNo ratings yet
- Using The Future Part 1 1Document48 pagesUsing The Future Part 1 1Ravi S GSRNo ratings yet
- SAMATVA N KASAT, AGE 16, Hyderabad: Appeared For 10 Grade IGCSE Boards in March 2022, Results Awaited ObjectiveDocument1 pageSAMATVA N KASAT, AGE 16, Hyderabad: Appeared For 10 Grade IGCSE Boards in March 2022, Results Awaited ObjectiveRavi S GSRNo ratings yet
- Digital Timer Modulator With Diagnostic Readout: Operating Instructions (701 10 Series)Document4 pagesDigital Timer Modulator With Diagnostic Readout: Operating Instructions (701 10 Series)Alex ConstantinescuNo ratings yet
- A Yan'an Pharmaceutical Co - 1 PDFDocument120 pagesA Yan'an Pharmaceutical Co - 1 PDF1123qazxsaqwNo ratings yet
- Ac 32Document16 pagesAc 32حِمْيَرْ مٌقْبِلْ الكَوْلِيNo ratings yet
- Physical Fitness Test Score CardDocument2 pagesPhysical Fitness Test Score CardDafchen Nio Mahasol100% (1)
- HRA at Capital CostDocument1 pageHRA at Capital Costsudhir mishraNo ratings yet
- Structured Question Form 4 Chapter 2: The Structure of The Atom Struktur Atom SUBTOPIC: Matter JirimDocument10 pagesStructured Question Form 4 Chapter 2: The Structure of The Atom Struktur Atom SUBTOPIC: Matter JirimbbbNo ratings yet
- Air Inlet and Exhaust SystemDocument10 pagesAir Inlet and Exhaust SystemRajaa XFNo ratings yet
- Bedside Handover PDFDocument20 pagesBedside Handover PDFshutekiNo ratings yet
- Daniel ADocument2 pagesDaniel AMuanchhana MizoNo ratings yet
- ZECCHI 05. All About Mothers. Pronatalist Discourses in Contemporary Spanish CinemaDocument20 pagesZECCHI 05. All About Mothers. Pronatalist Discourses in Contemporary Spanish CinemamonicasumoyNo ratings yet
- Independence Day SpeechDocument8 pagesIndependence Day SpeechSabir Mhd0% (1)
- A Major ProjectDocument16 pagesA Major ProjectRajuNo ratings yet
- ARTICULO Sintesis y Aplicacion de Dipetidos PDFDocument11 pagesARTICULO Sintesis y Aplicacion de Dipetidos PDFRosario PerezNo ratings yet
- Cannaflos - Auditplan BG Labs 2022-04!13!15 - Final Draft - CPDocument6 pagesCannaflos - Auditplan BG Labs 2022-04!13!15 - Final Draft - CPDemmin MorenoNo ratings yet
- Alano, Dhan Daryl B. Insurance Law Law 3DDocument5 pagesAlano, Dhan Daryl B. Insurance Law Law 3DJuan VillanuevaNo ratings yet
- Character Analysis: An Angel in Disguise. Thematic Analysis: The Cold WithinDocument5 pagesCharacter Analysis: An Angel in Disguise. Thematic Analysis: The Cold WithinHarshaditya KohliNo ratings yet
- GL-5 Gear Oil 85W-140 SDSDocument10 pagesGL-5 Gear Oil 85W-140 SDSDaniel Salazar CruzNo ratings yet
- Generic HACCP Models For FoodDocument18 pagesGeneric HACCP Models For FoodNatalia Lajca100% (1)
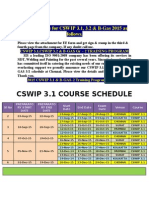
- Cswip 3.1 Course Schedule: New Schedule For CSWIP 3.1, 3.2 & B-Gas 2015 As FollowsDocument4 pagesCswip 3.1 Course Schedule: New Schedule For CSWIP 3.1, 3.2 & B-Gas 2015 As FollowsmuneeshwaraperumalNo ratings yet
- Tayag v. CA (Jacalne)Document2 pagesTayag v. CA (Jacalne)Jericho JacalneNo ratings yet
- Natural Treatments For Alzheimers 35ppDocument35 pagesNatural Treatments For Alzheimers 35ppaman_arora100% (1)
- Customer Satisfaction With The Service of Bed and Breakfast in Malaybalay City 2022-2023Document11 pagesCustomer Satisfaction With The Service of Bed and Breakfast in Malaybalay City 2022-2023Michaela Amor O. ManaloNo ratings yet
- How A Bill Becomes A LawDocument1 pageHow A Bill Becomes A LawNurseAmyNo ratings yet
- Sun PDFDocument10 pagesSun PDFmiguel.pelicano@gmail.comNo ratings yet
- Condilectomia Alta VS Condilectomia ProporcionalDocument6 pagesCondilectomia Alta VS Condilectomia ProporcionalJuan Carlos MeloNo ratings yet
- New ResumeDocument2 pagesNew ResumeDana McgrottyNo ratings yet
- Prosperity Power SignatureDocument26 pagesProsperity Power SignatureAndrew Horatio100% (2)