Jana Swasthya 2nd Issue (May - June 23)
Jana Swasthya 2nd Issue (May - June 23)
Download as docx, pdf, or txt
You might also like
- SAGE Vancouver Reference StyleDocument2 pagesSAGE Vancouver Reference StyledharmpalNo ratings yet
- "Medicine Man" (1992) Film ReviewDocument2 pages"Medicine Man" (1992) Film Reviewirish x100% (1)
- Lab Report Alka-SeltzerDocument2 pagesLab Report Alka-SeltzerHingaffersNo ratings yet
- Sinking Flagships and HealthDocument4 pagesSinking Flagships and HealthIraSinghalNo ratings yet
- HealthcareDocument10 pagesHealthcareTanish DhandNo ratings yet
- A Comprehensive Analysis of Ayushman BharatDocument12 pagesA Comprehensive Analysis of Ayushman BharatMahika Gandhi100% (1)
- Healthcare Delivery in India-CRISIL-Report-January-8-2022Document52 pagesHealthcare Delivery in India-CRISIL-Report-January-8-2022adikabraNo ratings yet
- Budgeting in Health Care System in IndiaDocument16 pagesBudgeting in Health Care System in IndiaABINASHNo ratings yet
- MM Project 111Document33 pagesMM Project 111yaswanthmangalagiri16No ratings yet
- Budget and Eco PackageDocument6 pagesBudget and Eco PackageMeghan PaulNo ratings yet
- Boost Expenditure, Strengthen NRHM To Become Atmanirbhar' in HealthcareDocument1 pageBoost Expenditure, Strengthen NRHM To Become Atmanirbhar' in HealthcareSunny SahayNo ratings yet
- AYushman Bharat AnalysisDocument12 pagesAYushman Bharat Analysisravi767457507No ratings yet
- Impact of Covid 19 in BangladeshDocument20 pagesImpact of Covid 19 in BangladeshShadowNo ratings yet
- Health CareDocument18 pagesHealth CareRaghav BishtNo ratings yet
- Healthcare Industry UpdatesDocument3 pagesHealthcare Industry Updatesgopal krishan kumarNo ratings yet
- STPIwswDocument10 pagesSTPIwswmotivationals.life.stylesNo ratings yet
- Healthcare Industry: (Document Subtitle)Document19 pagesHealthcare Industry: (Document Subtitle)Raghav BishtNo ratings yet
- Economics of Health and HealthcareDocument21 pagesEconomics of Health and HealthcareJai KumarNo ratings yet
- Union Budget 2019 ExpectationsDocument6 pagesUnion Budget 2019 Expectationssantosh kumarNo ratings yet
- Health Infrastucture in IndiaDocument8 pagesHealth Infrastucture in IndiaBinit kumarNo ratings yet
- 5. Philippine National Health Accounts 2022 (PSA)Document47 pages5. Philippine National Health Accounts 2022 (PSA)haynnaNo ratings yet
- Industrial EconomicsDocument14 pagesIndustrial EconomicsGaurav AgarwalNo ratings yet
- Fy 2023 Budget in BriefDocument174 pagesFy 2023 Budget in BriefTim BrownNo ratings yet
- Health Sector of BangladeshDocument5 pagesHealth Sector of BangladeshAlo StudentNo ratings yet
- Compare Budget 2023 With 2022Document8 pagesCompare Budget 2023 With 2022Vartika VNo ratings yet
- Budget Briefs: Ayushman BharatDocument12 pagesBudget Briefs: Ayushman BharatAbhishek RavikumarNo ratings yet
- National Health Policy, 2017: Revealing Public Health ChicaneryDocument12 pagesNational Health Policy, 2017: Revealing Public Health ChicaneryRohan RegiNo ratings yet
- Indian HealthcareDocument2 pagesIndian Healthcarenisha SomasekharanNo ratings yet
- Croatia - Health System Summary 2022Document22 pagesCroatia - Health System Summary 2022Orosanu LauraNo ratings yet
- Public Health Development and Economic Growth Evidence From Chinese CitiesDocument26 pagesPublic Health Development and Economic Growth Evidence From Chinese CitiesFala RafaNo ratings yet
- National Health Accounts Report 2014Document24 pagesNational Health Accounts Report 2014Anonymous UpWci5No ratings yet
- The Financing Health System Problem in AlgeriaDocument6 pagesThe Financing Health System Problem in AlgeriaPavelNo ratings yet
- GCSR Nagaland - GTU ReportDocument10 pagesGCSR Nagaland - GTU ReportSatish J. MakwanaNo ratings yet
- Impact of Pradhan Mantri Jan Arogya Yojnaa On Indian EconomyDocument41 pagesImpact of Pradhan Mantri Jan Arogya Yojnaa On Indian EconomyyashNo ratings yet
- Mkhize Tables R62bn Budget For 2021/22Document13 pagesMkhize Tables R62bn Budget For 2021/22Jacaranda FM NewsNo ratings yet
- Eco Government BudgetDocument18 pagesEco Government Budgetananya29420No ratings yet
- Man Environment Interaction of Naz BasinDocument28 pagesMan Environment Interaction of Naz BasinTp TpNo ratings yet
- Health Budget 2020: - Presented byDocument11 pagesHealth Budget 2020: - Presented byShahdab SagariNo ratings yet
- Ealth Nsurance IN Ndia: R M - 05PH2010Document6 pagesEalth Nsurance IN Ndia: R M - 05PH2010api-26832469No ratings yet
- Regression AnalysisDocument10 pagesRegression AnalysisHarsh DiwakarNo ratings yet
- Health Care Services in India: Problems and Prospects: B. S. Ghuman Akshat MehtaDocument15 pagesHealth Care Services in India: Problems and Prospects: B. S. Ghuman Akshat MehtaPaul PriyarajNo ratings yet
- Espinosa Et Al. (2023) - Predictability and Financial Sufficiency in Colombia - Bayesian ApproachDocument18 pagesEspinosa Et Al. (2023) - Predictability and Financial Sufficiency in Colombia - Bayesian ApproachMauricio FerreiraNo ratings yet
- Analysis of The Union Budget, Fiscal Year 2023-24Document12 pagesAnalysis of The Union Budget, Fiscal Year 2023-24gorgeous1986No ratings yet
- EPWDocument6 pagesEPWSASWATINo ratings yet
- Health Law ProjectDocument22 pagesHealth Law ProjectVarun MittalNo ratings yet
- Future of Jobs HealthcareDocument7 pagesFuture of Jobs Healthcareincrediblerr14No ratings yet
- Economic Growth and Health Expenditure Analysis For Turkey: Evidence From Time SeriesDocument15 pagesEconomic Growth and Health Expenditure Analysis For Turkey: Evidence From Time SeriesHuy Lê ThanhNo ratings yet
- Ayushman Bharat Yojana A Memorable Health InitiatiDocument2 pagesAyushman Bharat Yojana A Memorable Health InitiatiPiyush ChaturvediNo ratings yet
- NHM AssignmentDocument15 pagesNHM AssignmentNatalia PatnaikNo ratings yet
- Union Budget ReportDocument25 pagesUnion Budget ReportSUBHAM KUMAR PANDANo ratings yet
- Economic and Political WeeklyDocument13 pagesEconomic and Political WeeklyRotariu AlexandruNo ratings yet
- 11 13 LT HealthDocument36 pages11 13 LT HealthChristian_Azae_6813No ratings yet
- Concept of Health and DiseaseDocument7 pagesConcept of Health and DiseaseA.JONAH ELISA SHINYNo ratings yet
- Zhang 2023 Public Health Development and Economic Growth Evidence From Chinese CitiesDocument26 pagesZhang 2023 Public Health Development and Economic Growth Evidence From Chinese CitiesHuy Lê ThanhNo ratings yet
- Report On The High Healthcare Costs in IndiaDocument3 pagesReport On The High Healthcare Costs in IndiaSydkoNo ratings yet
- Pi Is 0140673619308414Document28 pagesPi Is 0140673619308414VitaNo ratings yet
- Gender Budget 2023-24Document56 pagesGender Budget 2023-24ppanda14No ratings yet
- Evidence Based Field Work ReportDocument16 pagesEvidence Based Field Work ReportSuraj MauryaNo ratings yet
- Salient Features of National Health Policy 2017Document7 pagesSalient Features of National Health Policy 2017rajsandhu25No ratings yet
- Emergency & Trauma: Amar.N Vaishnavi.D Vamshi.K B.Sc. EmcctDocument15 pagesEmergency & Trauma: Amar.N Vaishnavi.D Vamshi.K B.Sc. Emcctkota vamshiNo ratings yet
- Fpubh 09 795869Document11 pagesFpubh 09 795869Raysa AndreiNo ratings yet
- State Led Innovations For Achieving UnivDocument8 pagesState Led Innovations For Achieving UnivPragyan MonalisaNo ratings yet
- Connecting care: Global best Practices & The Rise of Indian Digital Health EcosystemFrom EverandConnecting care: Global best Practices & The Rise of Indian Digital Health EcosystemNo ratings yet
- SME Management - 1Document19 pagesSME Management - 1MaQsud AhMad SaNdhuNo ratings yet
- Marketing Research and Its LimitationsDocument54 pagesMarketing Research and Its LimitationsDhani Shanker ChaubeyNo ratings yet
- Cepeda-Carrion Et Al. 2012 BJMDocument21 pagesCepeda-Carrion Et Al. 2012 BJMmassmurNo ratings yet
- FAC4764 Study Pack 2Document41 pagesFAC4764 Study Pack 2Muvhusi NethonondaNo ratings yet
- Credit Scoring: Beyond The NumbersDocument34 pagesCredit Scoring: Beyond The NumbersramssravaniNo ratings yet
- Alps Alpine SPVMDocument4 pagesAlps Alpine SPVMJose Carlos SoaresNo ratings yet
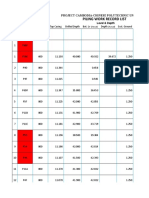
- Piling Work Record List: No Pile Code Diameter Level & Depth (MM)Document7 pagesPiling Work Record List: No Pile Code Diameter Level & Depth (MM)Nhoek Ren100% (1)
- Ohm'sDocument4 pagesOhm'snmcNo ratings yet
- Oop 11 (Exception Handling)Document20 pagesOop 11 (Exception Handling)Ahtisham MalikNo ratings yet
- RDBMS To MongoDB MigrationDocument20 pagesRDBMS To MongoDB Migrationabu1882No ratings yet
- 10 Sa1 English Sample Paper2Document11 pages10 Sa1 English Sample Paper2ashmitharajaNo ratings yet
- Hire Purchase, Lease, and Instalment Purchase SystemDocument10 pagesHire Purchase, Lease, and Instalment Purchase SystemVipin Mandyam KadubiNo ratings yet
- Pix Plus and Mepiquat Chloride Effects o PDFDocument8 pagesPix Plus and Mepiquat Chloride Effects o PDFgiorgosNo ratings yet
- The TerminatorDocument2 pagesThe TerminatordfgdfNo ratings yet
- Gửi SV. POA - CÂU HỎI NGẮN 1Document2 pagesGửi SV. POA - CÂU HỎI NGẮN 1Minh Hạnh NguyễnNo ratings yet
- ACI E802 Davis IRDocument15 pagesACI E802 Davis IRamroNo ratings yet
- Notes On Foreign Exchange Markets - Gr12Document22 pagesNotes On Foreign Exchange Markets - Gr12lwazindlovu468No ratings yet
- Mohammed Ashraf Sr. Data Analyst (216) 230-3332 Professional SummaryDocument4 pagesMohammed Ashraf Sr. Data Analyst (216) 230-3332 Professional SummarySrikanth ReddyNo ratings yet
- Sterilization of Compendial Articles: Background and ScopeDocument6 pagesSterilization of Compendial Articles: Background and Scopemolder.chenNo ratings yet
- Stock Jabar 21 Oktober 2022Document607 pagesStock Jabar 21 Oktober 2022Andre Putra PratamaNo ratings yet
- Lna100112c MDocument5 pagesLna100112c MS SelvarajNo ratings yet
- 1.4 Plant Structure and FunctionsDocument15 pages1.4 Plant Structure and Functionsaddy prairieNo ratings yet
- Assignment 3 Unit 11 Design and Test A Computer Network by Andrea SubdenDocument11 pagesAssignment 3 Unit 11 Design and Test A Computer Network by Andrea Subdenapi-348096893100% (1)
- University of Cambridge International Examinations International General Certificate of Secondary EducationDocument8 pagesUniversity of Cambridge International Examinations International General Certificate of Secondary Educationyassinn275No ratings yet
- KiSS DVD PLAYER Manual DP 508 3966 PDFDocument1 pageKiSS DVD PLAYER Manual DP 508 3966 PDFGurkan12No ratings yet
- 3D Printing of Core and Cavity InsertsDocument15 pages3D Printing of Core and Cavity InsertsSushmaNo ratings yet
- BLOWENGINEERING PLASTIC MACHINES Blow Molding Machine Manufacturer PDFDocument6 pagesBLOWENGINEERING PLASTIC MACHINES Blow Molding Machine Manufacturer PDFJoenetDarmawanNo ratings yet