Group 9 - DYING AND BEREAVEMENT
Group 9 - DYING AND BEREAVEMENT
Download as pdf or txt
You might also like
- Nbde Ii - Test Packet II-m (2000-2008)Document35 pagesNbde Ii - Test Packet II-m (2000-2008)yalahopa95% (19)
- Palliative Dr. WinemakerDocument32 pagesPalliative Dr. WinemakerEzhil Vendhan PalanisamyNo ratings yet
- Death Dying and BereavementDocument5 pagesDeath Dying and BereavementImmatureBastardNo ratings yet
- Chapter 15 PsychDocument2 pagesChapter 15 Psychkelemadu.15No ratings yet
- Dignity in Death and Dying: Garah Dae N. Diocos, RNDocument33 pagesDignity in Death and Dying: Garah Dae N. Diocos, RNLinang EchanisNo ratings yet
- Health Care Ethics-Wks.78Document50 pagesHealth Care Ethics-Wks.78Majestic RavenNo ratings yet
- GROUP 3 DIGINITY IN DYING AND DEATH - CompressedDocument35 pagesGROUP 3 DIGINITY IN DYING AND DEATH - CompressedSHANIAH PARCHAMENTONo ratings yet
- Death and Human Dignity NotesDocument20 pagesDeath and Human Dignity Noteshvjt5snvr2No ratings yet
- Ensuring Competent Care at The End of Life - A Life Long ProcessDocument32 pagesEnsuring Competent Care at The End of Life - A Life Long ProcessmatrixtrinityNo ratings yet
- Care of Dying and DeadDocument10 pagesCare of Dying and Deadd1choosenNo ratings yet
- Gero ReportDocument6 pagesGero ReportLen PinedaNo ratings yet
- 8-Lesson 8 Grief and BereavementDocument9 pages8-Lesson 8 Grief and Bereavementamnapsy1122No ratings yet
- Dignity in Death and Dying: BioethicsDocument14 pagesDignity in Death and Dying: BioethicsMichelle Bigcas100% (1)
- Euthanasia LatestDocument8 pagesEuthanasia LatestDenessaLugoNo ratings yet
- Notes - EthicsDocument9 pagesNotes - EthicsJajangNo ratings yet
- Notes - EthicsDocument9 pagesNotes - EthicsJajangNo ratings yet
- Euthanasia Slide NotesDocument4 pagesEuthanasia Slide NotesTeo Ji QiNo ratings yet
- End of Life Issues(1)Document21 pagesEnd of Life Issues(1)Justin FluidityNo ratings yet
- DNR GuidelinesDocument20 pagesDNR GuidelinesVirendar Pal SinghNo ratings yet
- Research Paper Final DraftDocument11 pagesResearch Paper Final Draftapi-239376109No ratings yet
- 00EUTHANASIADocument2 pages00EUTHANASIAShenn DollosoNo ratings yet
- Research Paper Draft 1Document11 pagesResearch Paper Draft 1api-239376109No ratings yet
- L14 Reading Reflections Study GuideDocument5 pagesL14 Reading Reflections Study GuideMaria Camila Vangh-egas JNo ratings yet
- 7 Important Euthanasia Pros and ConsDocument2 pages7 Important Euthanasia Pros and ConsChristian ArbolerasNo ratings yet
- Group 2 Dignity in Death and Dying EthicsDocument8 pagesGroup 2 Dignity in Death and Dying EthicsNicole BartolomeNo ratings yet
- Mercy KillingDocument7 pagesMercy KillingAlmairah EliasNo ratings yet
- FMCH3 Applied Health Ethics InfographicsDocument5 pagesFMCH3 Applied Health Ethics InfographicsOdy GatesNo ratings yet
- Etics in The ICU - NewDocument9 pagesEtics in The ICU - NewGhinter MariusNo ratings yet
- Hospice CareDocument31 pagesHospice CareQuennie Abellon QuimanNo ratings yet
- Palliative Care Module 1Document104 pagesPalliative Care Module 1ورد خواطر100% (1)
- End of Life IssuesDocument11 pagesEnd of Life Issuesjhommmmm100% (1)
- Cahpter 19 NotesDocument3 pagesCahpter 19 NoteslleeaannllssNo ratings yet
- Ethics PaperDocument6 pagesEthics Paperapi-250341699No ratings yet
- Lecture BioethicsDocument51 pagesLecture BioethicsElvis obajeNo ratings yet
- week-10-PPT-NCM108-HEALTH-ETHICS (20241010101554)Document52 pagesweek-10-PPT-NCM108-HEALTH-ETHICS (20241010101554)stephanie Ann PlanciaNo ratings yet
- Patient-Centered Care at The End of Life.07Document52 pagesPatient-Centered Care at The End of Life.07api-3755169100% (1)
- 10 WKDocument15 pages10 WKEmely V.No ratings yet
- The Debate: Wouldn't Do All That You Are Doing and Would Allow Her To Die Peacefully"Document9 pagesThe Debate: Wouldn't Do All That You Are Doing and Would Allow Her To Die Peacefully"Aekagra SaxenaNo ratings yet
- Richie Euthanasia PDFDocument64 pagesRichie Euthanasia PDFJanet GawareNo ratings yet
- Thesis Paper On EuthanasiaDocument5 pagesThesis Paper On Euthanasialidzckikd100% (1)
- End of Life CareDocument19 pagesEnd of Life CareArjumand ZargarNo ratings yet
- Euthanasia: I. A. Basic InformationDocument4 pagesEuthanasia: I. A. Basic InformationRica Mae Agasen SalazarNo ratings yet
- EuthanasiaDocument2 pagesEuthanasiaPaula Andrea Fonseca BaronNo ratings yet
- End of Life CommunicationDocument27 pagesEnd of Life CommunicationjintuNo ratings yet
- Ethical Issues in The Care of Older PersonsDocument3 pagesEthical Issues in The Care of Older PersonsGodwin Babista GonzalesNo ratings yet
- 2 Psychological Issues in Advancing IllnessDocument11 pages2 Psychological Issues in Advancing IllnessBhoomejaa SKNo ratings yet
- Dr. Ram Manohar Lohiya National Law University, Lucknow: Death PsychologyDocument11 pagesDr. Ram Manohar Lohiya National Law University, Lucknow: Death PsychologyArpit UpadhyayNo ratings yet
- Causes of Death in Adults Ages 65 and OlderDocument9 pagesCauses of Death in Adults Ages 65 and OlderKaren Joyce Costales MagtanongNo ratings yet
- Final Draft - EssayDocument12 pagesFinal Draft - Essayapi-549319751No ratings yet
- Ethics Death and DyingDocument15 pagesEthics Death and DyingJerbs Llames100% (1)
- Justine Magbual Aiu Sociology and Aging Unit 2 Individual ProjectDocument8 pagesJustine Magbual Aiu Sociology and Aging Unit 2 Individual ProjectjustineaprilbaldozmagbualNo ratings yet
- Lesson 12Document39 pagesLesson 12Rizalyn Padua ReyNo ratings yet
- Physician Assisted Death NotesDocument10 pagesPhysician Assisted Death NotesJoel CurtisNo ratings yet
- Group Presentation - The Right To DieDocument26 pagesGroup Presentation - The Right To DieYuki WilliamsNo ratings yet
- Dignity in Death and Dying - BioethicsDocument14 pagesDignity in Death and Dying - BioethicsCyrvince Mahipus Bastasa100% (1)
- Euthanasia Paper ThesisDocument6 pagesEuthanasia Paper Thesislisabrownomaha100% (3)
- Ethical Dilemma Debate - Assisted SuicideDocument23 pagesEthical Dilemma Debate - Assisted SuicidepetitepetalsNo ratings yet
- Euthanasia: Which "M" Is It? Mercy or Murder?From EverandEuthanasia: Which "M" Is It? Mercy or Murder?Rating: 5 out of 5 stars5/5 (1)
- Extraction of Primary Teeth in Children: An Observational StudyDocument6 pagesExtraction of Primary Teeth in Children: An Observational StudyhayiarNo ratings yet
- Understanding The Impact of HIV-Associated Bone Marrow Alterations On ErythropoiesisDocument11 pagesUnderstanding The Impact of HIV-Associated Bone Marrow Alterations On ErythropoiesisKIU PUBLICATION AND EXTENSIONNo ratings yet
- Abbott HPV RealTime AssayDocument2 pagesAbbott HPV RealTime AssayIbrehimaNo ratings yet
- # Patella PDFDocument4 pages# Patella PDFikhosasihNo ratings yet
- Fanny Nabiilah - 21040079 - Main Idea and Implied ExercisesDocument7 pagesFanny Nabiilah - 21040079 - Main Idea and Implied Exercisesbagas semNo ratings yet
- Pulmonary Function TestDocument77 pagesPulmonary Function TestMohammed Saad NabhanNo ratings yet
- Week 2 Pathfit 3 Lesson 1 Introduction To Sports - Health - WellnessDocument5 pagesWeek 2 Pathfit 3 Lesson 1 Introduction To Sports - Health - WellnessAgapay Princess MerylleNo ratings yet
- Mapeh 6 1st Quarter ExamDocument7 pagesMapeh 6 1st Quarter ExamMARIBETH GUALNo ratings yet
- Green SerumDocument1 pageGreen SerumDocAxi Maximo Jr AxibalNo ratings yet
- Multicultural Nursing Care of Patients - NWS1665191866 - NRSE 4570 - Care Plan - 1Document4 pagesMulticultural Nursing Care of Patients - NWS1665191866 - NRSE 4570 - Care Plan - 1Carlos I. RomeroNo ratings yet
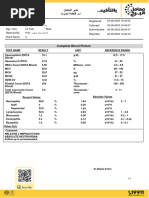
- Complete Blood Picture: DR - Magda SultanDocument4 pagesComplete Blood Picture: DR - Magda Sultanosama1000000No ratings yet
- Sustaine 10Document10 pagesSustaine 10Ivan Dario Hernandez ErazoNo ratings yet
- The Effects of SmokingDocument2 pagesThe Effects of SmokingNino-prexy AcdalNo ratings yet
- 2022 Virtual Eprs ForumDocument122 pages2022 Virtual Eprs ForumAljhan LingaNo ratings yet
- 3RD Quarter Exam in ENGLISH 10Document3 pages3RD Quarter Exam in ENGLISH 10Juvelyn LifanaNo ratings yet
- Totalpsa ArcDocument8 pagesTotalpsa Arctesteste testeNo ratings yet
- Fsu Dissertation FormatDocument6 pagesFsu Dissertation FormatPaperWritingServiceCollegeUK100% (2)
- KamiasDocument3 pagesKamiasIrene Carla Lacson Medina0% (1)
- Assignment On Antibiotics - ViosDocument8 pagesAssignment On Antibiotics - ViosIra Velle ViosNo ratings yet
- Cardiac DysrhythmiasDocument3 pagesCardiac DysrhythmiasWilbert GuerreroNo ratings yet
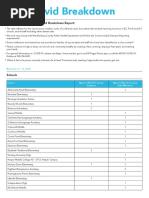
- CMS Covid BreakdownDocument2 pagesCMS Covid BreakdownEmma KoryntaNo ratings yet
- DAR 2023 (Aisa)Document7 pagesDAR 2023 (Aisa)Almira NadiaNo ratings yet
- Broiler Disease Reference GuideDocument70 pagesBroiler Disease Reference Guideebabo.1408No ratings yet
- ICU Management of Acute PancreatitisDocument77 pagesICU Management of Acute PancreatitisAndriy SubieNo ratings yet
- Cobas 4000 Menu PDFDocument3 pagesCobas 4000 Menu PDF林圣贺No ratings yet
- AyushiPatel - A044 - Impact of Covid-19 Pandemic On Indian Economy - .Document9 pagesAyushiPatel - A044 - Impact of Covid-19 Pandemic On Indian Economy - .Ayushi PatelNo ratings yet
- Bioidentical Hormones-2-1Document2 pagesBioidentical Hormones-2-1api-2068477050% (1)
- Deep Blue Ocean - RafeDocument6 pagesDeep Blue Ocean - Rafeexm68150No ratings yet
- Shapes and Arrangements of BacteriaDocument22 pagesShapes and Arrangements of BacteriaCarl Elexer Cuyugan Ano100% (3)