Fact Sheet PediatricAPTA Motor Development Variations Across Cultures
Fact Sheet PediatricAPTA Motor Development Variations Across Cultures
Download as pdf or txt
You might also like
- Functional Training Handbook (PDFDrive) (001-153)Document153 pagesFunctional Training Handbook (PDFDrive) (001-153)ssa.ptrainer100% (1)
- Vdoc - Pub The Muscular System Manual The Skeletal Muscles of The Human BodyDocument803 pagesVdoc - Pub The Muscular System Manual The Skeletal Muscles of The Human BodyNguyễn Thế Cường100% (14)
- Group 2 PPT RawDocument25 pagesGroup 2 PPT RawGil Sunpayco Jr.No ratings yet
- Childrearing Practices: Creating Programs Where Traditions and Modern Practices MeetDocument69 pagesChildrearing Practices: Creating Programs Where Traditions and Modern Practices MeetJayjeet BhattacharjeeNo ratings yet
- Transcultural Perspectives in The Nursing Care of ChildrenDocument23 pagesTranscultural Perspectives in The Nursing Care of Childrenceanbae.patajoNo ratings yet
- Transcultural Perspectives in The Nursing Care of Children (1) - MergedDocument81 pagesTranscultural Perspectives in The Nursing Care of Children (1) - Mergedceanbae.patajoNo ratings yet
- Children in A Culturally Diverse Society-ReportingDocument7 pagesChildren in A Culturally Diverse Society-ReportingyanduyoNo ratings yet
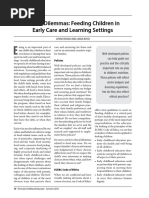
- Ethical Dilemmas: Feeding Children in Early Care and Learning SettingsDocument3 pagesEthical Dilemmas: Feeding Children in Early Care and Learning SettingsMishael AbogadoNo ratings yet
- Week 14 MCHNDocument5 pagesWeek 14 MCHNCyrille Kibbz DonatoNo ratings yet
- WCE - Inclusive Education RemymarDocument42 pagesWCE - Inclusive Education RemymarRemymar AnisNo ratings yet
- Pediatric ReviewerDocument3 pagesPediatric ReviewereannnicholleNo ratings yet
- CPP ManualDocument63 pagesCPP ManualLady Lyn NarsolesNo ratings yet
- Ob2 Sas 40Document7 pagesOb2 Sas 40????No ratings yet
- Final Hearth Book - PDF - CORE GroupDocument199 pagesFinal Hearth Book - PDF - CORE GroupRavishka Gunathilake100% (1)
- NAEYC Code PDFDocument4 pagesNAEYC Code PDFRoxana GhiațăuNo ratings yet
- IYCF - UNICEF Infant and Young Child Feeding Counselling Cards For Community WorkersDocument31 pagesIYCF - UNICEF Infant and Young Child Feeding Counselling Cards For Community WorkersJewelle Anne Estanilla LimenNo ratings yet
- Counselling_CardsDocument31 pagesCounselling_Cardsjulieannemanalo22No ratings yet
- Parental ChildDocument9 pagesParental ChildFadia Talia Salsabila HerviNo ratings yet
- Roles of A Child Development AssistantDocument1 pageRoles of A Child Development AssistantAngelica TronoNo ratings yet
- WK14 - Nursing Process for Promotion of Normal Growth and DevelopmentDocument4 pagesWK14 - Nursing Process for Promotion of Normal Growth and DevelopmentIanne InoueNo ratings yet
- Te Whāriki: He Whāriki Mātauranga Mō Ngā Mokopuna o Aotearoa: Early Childhood CurriculumDocument6 pagesTe Whāriki: He Whāriki Mātauranga Mō Ngā Mokopuna o Aotearoa: Early Childhood CurriculumIdol YoNo ratings yet
- YCFPDocument8 pagesYCFPMuskan ChadhaNo ratings yet
- Material Assessing children and young people health - Copy (2)Document42 pagesMaterial Assessing children and young people health - Copy (2)sesaeedhaniyah.dNo ratings yet
- Parental CareDocument2 pagesParental Care0-benk-0No ratings yet
- Developmental MilestoneDocument17 pagesDevelopmental MilestoneRafael MarvinNo ratings yet
- Project NajaDocument13 pagesProject NajaNatasha Jean CardonaNo ratings yet
- Focus On Child Health PDFDocument28 pagesFocus On Child Health PDFAbhishekNo ratings yet
- The Role of Schools in Preventing OverweightDocument11 pagesThe Role of Schools in Preventing Overweightceles83No ratings yet
- Summary OutlineDocument3 pagesSummary OutlineVy NguyễnNo ratings yet
- Savaliya Hiren - Ex.1Document7 pagesSavaliya Hiren - Ex.1Hiren SavaliyaNo ratings yet
- The Unstable Future and Health of The Youth Due To PovertyDocument3 pagesThe Unstable Future and Health of The Youth Due To PovertyOccasus DeirdreNo ratings yet
- Children and Young People's Nursing: A Philosophy of Care: Guidance For Nursing StaffDocument8 pagesChildren and Young People's Nursing: A Philosophy of Care: Guidance For Nursing Staffandreicmarin1981No ratings yet
- MATERNAL AND CHILD HEALTH NURSING SUMMARY Chapter 30-34 (Adelle Pillitteri)Document134 pagesMATERNAL AND CHILD HEALTH NURSING SUMMARY Chapter 30-34 (Adelle Pillitteri)CHRISTIE MONTANO100% (6)
- Go Baby GoDocument4 pagesGo Baby GobremuselNo ratings yet
- Pdhpe 7-10-2024 Parent and Carer GuideDocument2 pagesPdhpe 7-10-2024 Parent and Carer GuideAli MohammedNo ratings yet
- Bianka Part 2Document10 pagesBianka Part 2api-85429702No ratings yet
- H. Nursing Care Plan: Altered Parenting RoleDocument2 pagesH. Nursing Care Plan: Altered Parenting RoleClovie ArsenalNo ratings yet
- Palestine Case StudyDocument12 pagesPalestine Case StudyBashaer Abu KhadejaNo ratings yet
- Family With An Infant (Group 3)Document12 pagesFamily With An Infant (Group 3)Jessa Mae OhaoNo ratings yet
- Pediatrics 2008 High E1008 15Document10 pagesPediatrics 2008 High E1008 15Nanda Asyura RizkyaniNo ratings yet
- 120 m6Document26 pages120 m6k5gphk5pyxNo ratings yet
- Developmentally Appropriate Practice and Its Implication To K 12 (J. Ramos)Document54 pagesDevelopmentally Appropriate Practice and Its Implication To K 12 (J. Ramos)Lily Flores GauiranNo ratings yet
- Document From GreatDocument15 pagesDocument From GreatTaif SalimNo ratings yet
- Prioritizing Nutrition and Feeding in Alternative Care 1Document13 pagesPrioritizing Nutrition and Feeding in Alternative Care 1mehwishfarooq729No ratings yet
- Developmental MilestonesDocument17 pagesDevelopmental MilestonesSardono WidinugrohoNo ratings yet
- 11. Role of Nurses in Family welfare servicesDocument20 pages11. Role of Nurses in Family welfare servicesSWATHY P PNo ratings yet
- Adoption Literature ReviewDocument45 pagesAdoption Literature Reviewdanielalagrimas1No ratings yet
- The Positive Parent Raising Healthy Happy and Successful Children Birth Adolescence PDFDocument265 pagesThe Positive Parent Raising Healthy Happy and Successful Children Birth Adolescence PDFSyibly Avivy A. MulachelaNo ratings yet
- teams-IND-Nutrition-Knowledge@UNICEF (Nutrition) - UNICEF Reports-2024 Social Protection For Nutrition India A Proposed Framework-5.0Document14 pagesteams-IND-Nutrition-Knowledge@UNICEF (Nutrition) - UNICEF Reports-2024 Social Protection For Nutrition India A Proposed Framework-5.0proyecto223327No ratings yet
- 2018 Perceptions of Childcare SPMDocument9 pages2018 Perceptions of Childcare SPMDori OrtNo ratings yet
- Transes PHNDocument24 pagesTranses PHNimjuuNo ratings yet
- 06 Abr 09Document44 pages06 Abr 09plucichNo ratings yet
- ANEMIA Group LEARNING PROJECTDocument32 pagesANEMIA Group LEARNING PROJECTScribdTranslationsNo ratings yet
- Children Left BehindDocument10 pagesChildren Left BehindЛена ЩербинаNo ratings yet
- Study Guide 7 - Transcultural Perspectives in The Nursing Care of ChildrenDocument3 pagesStudy Guide 7 - Transcultural Perspectives in The Nursing Care of ChildrenTim john louie RancudoNo ratings yet
- Maece 202 Part 1Document47 pagesMaece 202 Part 1Khristine DusayenNo ratings yet
- African Socialization Goals Practices AnDocument63 pagesAfrican Socialization Goals Practices AnAngela AmoatwoNo ratings yet
- 658-Article Text-26098-2-10-20220428Document13 pages658-Article Text-26098-2-10-20220428Chloe SumalinogNo ratings yet
- Disability Awareness InfographicDocument3 pagesDisability Awareness Infographicapi-531068426No ratings yet
- Parenting Styles Decoded: Finding What Works Best for Your FamilyFrom EverandParenting Styles Decoded: Finding What Works Best for Your FamilyNo ratings yet
- Empowering Parents & Teachers: How Parents and Teachers Can Develop Collaborative PartnershipsFrom EverandEmpowering Parents & Teachers: How Parents and Teachers Can Develop Collaborative PartnershipsNo ratings yet
- OKC Vs CKC ExercisesDocument2 pagesOKC Vs CKC Exercises杨钦杰No ratings yet
- Scientific Principles of Sports RehabilitationDocument12 pagesScientific Principles of Sports RehabilitationRAJESH MALIKNo ratings yet
- Joselito Melendez CV 2 2Document2 pagesJoselito Melendez CV 2 2joselitomelendez9No ratings yet
- Resume 2023Document2 pagesResume 2023api-547385390No ratings yet
- Canada Books ReferanceDocument3 pagesCanada Books ReferanceRamkumar MurugesanNo ratings yet
- англійська 28.09.23Document1 pageанглійська 28.09.23ol.oleksandrivnaNo ratings yet
- Ankita KothariDocument5 pagesAnkita Kothariankita kothariNo ratings yet
- Sarhad University of Science & Information Technology, PeshawarDocument3 pagesSarhad University of Science & Information Technology, Peshawarkhan khanNo ratings yet
- Physical Rehabilitation Assessment MBBS5 2024Document3 pagesPhysical Rehabilitation Assessment MBBS5 2024mahfuza aliNo ratings yet
- Instant Download Canine Rehabilitation and Physical Therapy 1st Edition Darryl Millis Ms DVM PDF All ChapterDocument78 pagesInstant Download Canine Rehabilitation and Physical Therapy 1st Edition Darryl Millis Ms DVM PDF All Chapterwetalagacia100% (3)
- Sports Medicine Meets Musculoskeletal MeDocument3 pagesSports Medicine Meets Musculoskeletal MeMotea IoanaNo ratings yet
- Exploration of The History of PhysiotherapyDocument5 pagesExploration of The History of PhysiotherapyÑítíßh ÑíràlàNo ratings yet
- SIRA NumberDocument2 pagesSIRA NumberrianabeggNo ratings yet
- Assignment No. 13 - PCAMDocument1 pageAssignment No. 13 - PCAMMIPZI GAIL SILVANo ratings yet
- Defensible Documentation Quick ReferenceDocument3 pagesDefensible Documentation Quick ReferencecderdnaseNo ratings yet
- PSM RehabilitationDocument19 pagesPSM RehabilitationshivaniNo ratings yet
- Making Vision 2020 A Reality: Ben F Massey, JR, PT, MADocument4 pagesMaking Vision 2020 A Reality: Ben F Massey, JR, PT, MA杨钦杰No ratings yet
- Syllabus MPT 1 YrDocument38 pagesSyllabus MPT 1 YrShubham ChopadeNo ratings yet
- Spatial Temporal Parameters, Pelvic and Lower Limb Movements During Gait in Individuals With Reduced Passive Ankle DorsiflexionDocument7 pagesSpatial Temporal Parameters, Pelvic and Lower Limb Movements During Gait in Individuals With Reduced Passive Ankle DorsiflexionAriene RibeiroNo ratings yet
- Depression and Anxiety Symptoms Among Lebanese Lower Limb Traumatic Amputees Association With Education Employment Adjustment To Amputation and ProDocument15 pagesDepression and Anxiety Symptoms Among Lebanese Lower Limb Traumatic Amputees Association With Education Employment Adjustment To Amputation and ProResearch and Development DepartmentNo ratings yet
- Final Version of SynopsisDocument43 pagesFinal Version of Synopsisahmadalik525No ratings yet
- Evolution Healing Centre - Lived Experiences of Stroke For Bermuda 2022Document22 pagesEvolution Healing Centre - Lived Experiences of Stroke For Bermuda 2022BernewsAdminNo ratings yet
- Physical Therapy Books List (A) 01Document5 pagesPhysical Therapy Books List (A) 01Javed Noor Muhammad GabaNo ratings yet
- PPTX, 10-EffleurageDocument11 pagesPPTX, 10-EffleuragemeachieNo ratings yet
- Acceptedquals Feb 2022 UpdateDocument4 pagesAcceptedquals Feb 2022 UpdateEmma TheobaldNo ratings yet
- Biomechanical and Rehab FORDocument3 pagesBiomechanical and Rehab FORKenny ClayNo ratings yet
- Immediate download Writing Patient Client Notes Ensuring Accuracy in Documentation Fourth Edition Ginge Kettenbach ebooks 2024Document56 pagesImmediate download Writing Patient Client Notes Ensuring Accuracy in Documentation Fourth Edition Ginge Kettenbach ebooks 2024hamdanzaynah28100% (1)
- Scholarships For Physiotherapy StudentsDocument7 pagesScholarships For Physiotherapy Studentsusama jamilNo ratings yet