Nca1 Health Assessment Notes
Nca1 Health Assessment Notes
Download as pdf or txt
You might also like
- Health and Physical Assessment in Nursing 3rd Edition DAmico Test Bank DownloadDocument27 pagesHealth and Physical Assessment in Nursing 3rd Edition DAmico Test Bank DownloadSharon Reper100% (24)
- Physical Assessment SampleDocument6 pagesPhysical Assessment Samplecarlylove33% (3)
- Inspection of Hair, Skin and NailsDocument3 pagesInspection of Hair, Skin and NailsMhelle PalangdaoNo ratings yet
- Тopic 4.2. Auscultation of the lungs. Additional sounds.Document7 pagesТopic 4.2. Auscultation of the lungs. Additional sounds.Donia HnainiaNo ratings yet
- Concept Map Finished 2Document6 pagesConcept Map Finished 2api-352785497100% (1)
- Integumentary Assessment: Skin, Hair, and NailsDocument42 pagesIntegumentary Assessment: Skin, Hair, and NailsSIR ONENo ratings yet
- Name: - AgeDocument15 pagesName: - Agebbasya eihynaNo ratings yet
- Health AssessmentDocument14 pagesHealth AssessmentRui Si GbNo ratings yet
- Physical AssessmentDocument13 pagesPhysical Assessmentdesh_dacanay100% (1)
- PA Jennifer PaglingayenDocument27 pagesPA Jennifer PaglingayenJm PecadizoNo ratings yet
- J C2 VeterinaryDocument45 pagesJ C2 Veterinaryapi-3853285100% (1)
- Instructions For Skin, Hair and Nails Assessment (2024-2025) - TaggedDocument2 pagesInstructions For Skin, Hair and Nails Assessment (2024-2025) - Taggedtwhdgtgxt4No ratings yet
- 9 Physical Assessment OsmaDocument29 pages9 Physical Assessment OsmaKate ChavezNo ratings yet
- WK8 9 Skin Hair Nails Head and NeckDocument9 pagesWK8 9 Skin Hair Nails Head and NeckTrisha Mae BalladNo ratings yet
- Assessing Skin, Hair and NailsDocument4 pagesAssessing Skin, Hair and NailsJa Dimas50% (2)
- Ha SL NotesDocument9 pagesHa SL NotesmaylenekitongNo ratings yet
- Physical Assessment Body Parts Assessment Method Use Normal Findings Actual Findings Analysis and InterpretationDocument12 pagesPhysical Assessment Body Parts Assessment Method Use Normal Findings Actual Findings Analysis and InterpretationCleoville OrdonaNo ratings yet
- Physical Examination SaDocument5 pagesPhysical Examination Sashin_2173No ratings yet
- HA 2nd Skin AssessmentDocument12 pagesHA 2nd Skin AssessmentChilled Moo MooNo ratings yet
- SkinDocument78 pagesSkinSamantha SansanoNo ratings yet
- STIMULI AND RESPONSEDocument28 pagesSTIMULI AND RESPONSEnurainizuki94No ratings yet
- Skin AssessmentDocument32 pagesSkin AssessmentMahmoud SherifNo ratings yet
- PADocument7 pagesPAHydie Mae AlcabedosNo ratings yet
- Head-To-Toe Assessment GuideDocument14 pagesHead-To-Toe Assessment GuideNathalie kate petallarNo ratings yet
- Skills # 10: The Male Genitalia: Breast and Lymphatic VesselsDocument3 pagesSkills # 10: The Male Genitalia: Breast and Lymphatic VesselsAlyssa Ashley A. ImamNo ratings yet
- Physical Health ExaminationDocument85 pagesPhysical Health ExaminationBryan Lloyd RayatNo ratings yet
- Physical AssessmenttDocument199 pagesPhysical AssessmenttleaangelasanpedrotongolNo ratings yet
- Rle Skin Hair Nails Head OnlyDocument2 pagesRle Skin Hair Nails Head OnlyArabiah AbdullahNo ratings yet
- Collecting Objective DataDocument6 pagesCollecting Objective DataLili M.No ratings yet
- Management of Client With Integumentary DisordersDocument97 pagesManagement of Client With Integumentary Disordersduday76100% (1)
- Assessment of SkinDocument16 pagesAssessment of SkinmakathrinasanchezNo ratings yet
- Health AssessmentDocument9 pagesHealth AssessmentJESSMAR GRACE PARMOSANo ratings yet
- Thorax, Skin, Hair, Nails ObjectivesDocument3 pagesThorax, Skin, Hair, Nails Objectivesctramel001100% (1)
- finals-ITPDocument11 pagesfinals-ITPq4brmtkbjvNo ratings yet
- Inpsyc Unit 3Document7 pagesInpsyc Unit 3mrnxakeiraNo ratings yet
- Physical Assessment of Family GDocument151 pagesPhysical Assessment of Family GDianneNo ratings yet
- Physical Assessment RevDocument11 pagesPhysical Assessment Revpsyche.ladicaNo ratings yet
- Somattic Sensation NotesDocument13 pagesSomattic Sensation Notesrrkn9njjhzNo ratings yet
- La Salle University: College of Nursing Ozamiz CityDocument12 pagesLa Salle University: College of Nursing Ozamiz CityKristine NacuaNo ratings yet
- Skin. Hair Scalp and Nails With RationaleDocument3 pagesSkin. Hair Scalp and Nails With Rationalehatdog hatdogNo ratings yet
- E3 Chap 01 6upDocument7 pagesE3 Chap 01 6upatif murtazaNo ratings yet
- Cns SensoryDocument18 pagesCns Sensoryshebus123No ratings yet
- Neonatal Assessment Guide / Independent StudyDocument10 pagesNeonatal Assessment Guide / Independent StudyoapsdoaksdokaNo ratings yet
- TLOY CLIN MED HEENT - Head Face NeckDocument11 pagesTLOY CLIN MED HEENT - Head Face NeckTRINIDAD, ALYANNA V.No ratings yet
- Activity No. 3 LabDocument3 pagesActivity No. 3 LabGwyneth Dane LaranangNo ratings yet
- Drug NameDocument4 pagesDrug Namecheanne003No ratings yet
- Case FonteDocument22 pagesCase FontereizelsamaniegoNo ratings yet
- Integumentary System: Most Predominant Structure Epidermis DermisDocument6 pagesIntegumentary System: Most Predominant Structure Epidermis DermisANGEL JANELLE ANGELESNo ratings yet
- PA Hyperthyroidism 1 - 071245Document6 pagesPA Hyperthyroidism 1 - 071245Eben Alameda-PalapuzNo ratings yet
- Health Assessment - LecDocument18 pagesHealth Assessment - Lecrhainjordan30No ratings yet
- Physical Assessment of The IntegumentDocument75 pagesPhysical Assessment of The IntegumentDiane BaunsitNo ratings yet
- Tagum Doctor'S College, Inc. Mahogany St. Rabe Subdivision, Tagum City Bachelor of Science in NursingDocument6 pagesTagum Doctor'S College, Inc. Mahogany St. Rabe Subdivision, Tagum City Bachelor of Science in NursingreginawilsonNo ratings yet
- HA PreparingForTheExaminationDocument4 pagesHA PreparingForTheExaminationkrixiededios7No ratings yet
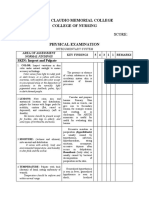
- Name: Score:: Tomas Claudio Memorial College College of NursingDocument31 pagesName: Score:: Tomas Claudio Memorial College College of NursingOng, IvanNo ratings yet
- Sensory EvaluationDocument6 pagesSensory EvaluationNicole Andrea GarciaNo ratings yet
- Week 3 Ha-Msn Assessment TechniquesDocument35 pagesWeek 3 Ha-Msn Assessment Techniquesanabelle BuranNo ratings yet
- Health AssessmentDocument11 pagesHealth AssessmentKikay VillarenNo ratings yet
- Environmental EmergencyDocument4 pagesEnvironmental EmergencyJUDE MARIANO JR. ALBANCES CARLOSNo ratings yet
- Sensory Chap 3 LatestDocument93 pagesSensory Chap 3 LatestAhmed khanNo ratings yet
- Seven Easy and Cheap Methods for Preparing, Tanning, Dressing, Scenting and Renovating all Wool and Fur Peltries: Also all Fine Leather as Adapted to the Manufacture of Robes, Mats, Caps, Gloves, Mitts, OvershoesFrom EverandSeven Easy and Cheap Methods for Preparing, Tanning, Dressing, Scenting and Renovating all Wool and Fur Peltries: Also all Fine Leather as Adapted to the Manufacture of Robes, Mats, Caps, Gloves, Mitts, OvershoesNo ratings yet
- Physical Examinations Respiratory System: InspectionDocument5 pagesPhysical Examinations Respiratory System: InspectionAzizan HannyNo ratings yet
- Respiratory Sounds: by Oluwaseun OlaiyaDocument16 pagesRespiratory Sounds: by Oluwaseun OlaiyaOlaiya OluwaseunNo ratings yet
- EXAMINATION OF RESPIRATORY SYSTEM - -Document159 pagesEXAMINATION OF RESPIRATORY SYSTEM - -iqbalnaushad26No ratings yet
- J Smallrumres 2010 04 020Document6 pagesJ Smallrumres 2010 04 020Tauseef Ahmad MalikNo ratings yet
- Perform Nursing AssessmentDocument81 pagesPerform Nursing AssessmentAhmanur Sule100% (1)
- Chest and LungsDocument4 pagesChest and LungsDale Ros CollamatNo ratings yet
- Family Case Study GarciaJ Khate Zaira SDocument16 pagesFamily Case Study GarciaJ Khate Zaira Salbert delos santosNo ratings yet
- Semio RespDocument52 pagesSemio RespNayara CasagrandeNo ratings yet
- Local Chest Examination AMM2Document37 pagesLocal Chest Examination AMM2saeedoofNo ratings yet
- Nursing Assesment 2019Document17 pagesNursing Assesment 2019Jemmy KherisnaNo ratings yet
- 2020thoraxlungs Neckheart VesselsDocument171 pages2020thoraxlungs Neckheart VesselsFaith madayagNo ratings yet
- Clinical Examinations by DR - Shamol MMCDocument1,174 pagesClinical Examinations by DR - Shamol MMCsadiaafrin66523100% (1)
- Thorax and Lungs AssessmentDocument107 pagesThorax and Lungs Assessmentyanna aNo ratings yet
- Inspection, Palpation, Percussion, Auscultation (IPPA) TipsDocument10 pagesInspection, Palpation, Percussion, Auscultation (IPPA) TipsMarjorie Joy GreciaNo ratings yet
- DR Amsalu Bekele Ass - Professor of Medicine Head of Chest Unit Department of Internal Medicine Addis Ababa University, School of Medicine Addis Ababa, EthiopiaDocument81 pagesDR Amsalu Bekele Ass - Professor of Medicine Head of Chest Unit Department of Internal Medicine Addis Ababa University, School of Medicine Addis Ababa, EthiopiaBethelhem BirhanuNo ratings yet
- Respiratory Examination OSCE GuideDocument33 pagesRespiratory Examination OSCE GuideAgleema AhmedNo ratings yet
- Lung Sounds 2Document1 pageLung Sounds 2Kyle LatayanNo ratings yet
- Lung ExaminationDocument16 pagesLung ExaminationShams AtrashNo ratings yet
- NRLTL QuizletDocument6 pagesNRLTL QuizletReniella HidalgoNo ratings yet
- Practical Notes - Clinical Examination of The Respiratory SystemDocument3 pagesPractical Notes - Clinical Examination of The Respiratory SystemPRASANTH KRISHNANo ratings yet
- 2.health AssessmentDocument7 pages2.health Assessment2BGrp3Plaza, Anna MaeNo ratings yet
- 11 Respiratory System Lesson PlanDocument5 pages11 Respiratory System Lesson Planchandan Singh100% (1)
- 07 - Lung Sounds - LearnerDocument2 pages07 - Lung Sounds - LearnerRafaelNo ratings yet
- Thorax and Lungs AnswersDocument3 pagesThorax and Lungs AnswersHazel Anne Dela CruzNo ratings yet
- Physical Exam - Chest 2006Document84 pagesPhysical Exam - Chest 2006api-19916399No ratings yet
- Thorax and Lungs ScriptDocument5 pagesThorax and Lungs ScriptThe GreatNo ratings yet
- Respiratory Video ScriptDocument3 pagesRespiratory Video ScriptNav KovNo ratings yet