Fluid and Electrolyte Disturbances
Fluid and Electrolyte Disturbances
Download as pdf or txt
You might also like
- BETA HCG Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pageBETA HCG Test Report Format Example Sample Template Drlogy Lab Reportseemaaingh1995No ratings yet
- NurseBossStore Nursing NotesDocument17 pagesNurseBossStore Nursing NotesMary Kimberly S. CaberteNo ratings yet
- 50 Most Commonly Prescribed Medications PDFDocument2 pages50 Most Commonly Prescribed Medications PDFChantelle Houston100% (1)
- MK Notes by YournursingspaceDocument60 pagesMK Notes by Yournursingspaceezinne obinna-uma100% (3)
- Pharm WorksheetsDocument29 pagesPharm Worksheetsj.siemens1d100% (2)
- ABGsDocument13 pagesABGsAmanda Maria100% (4)
- NCLEX Cram SheetDocument6 pagesNCLEX Cram Sheetaishwariyapokharel55No ratings yet
- Calendar of Days & Awareness DaysDocument2 pagesCalendar of Days & Awareness DaysAshfaque HossainNo ratings yet
- Medical Abbreviations: Beautiful Nursing LLCDocument2 pagesMedical Abbreviations: Beautiful Nursing LLCcarly100% (1)
- Med Surg Test 4 Study GuideDocument29 pagesMed Surg Test 4 Study GuideJess100% (2)
- Medication Work Sheet For MedSurgDocument5 pagesMedication Work Sheet For MedSurgRyanMitchell100% (3)
- Pharmacology Important Things To RememberDocument5 pagesPharmacology Important Things To RememberHydie100% (1)
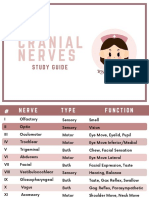
- Cranial NervesDocument6 pagesCranial Nervesvienny kayeNo ratings yet
- Analgesics: AnticonvulsantsDocument8 pagesAnalgesics: AnticonvulsantsGina Giammalvo100% (2)
- Blood Transfusions BN CopyrightDocument2 pagesBlood Transfusions BN CopyrightDENVER CARBON100% (1)
- DigitalPharmacologyBundle170Pages CompressedDocument170 pagesDigitalPharmacologyBundle170Pages Compressed98b5jc5hgtNo ratings yet
- Remembering Medication ClassificationsDocument2 pagesRemembering Medication ClassificationsGVHHNo ratings yet
- Mnemonics For NursingDocument35 pagesMnemonics For Nursingbetterdenthat100% (1)
- Pharmacology-ATI 150 Drug Cards PDFDocument4 pagesPharmacology-ATI 150 Drug Cards PDFholly100% (1)
- Lung SoundsDocument6 pagesLung SoundsAira KieNo ratings yet
- Electrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionDocument6 pagesElectrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionmkninnyNo ratings yet
- Med Surg BundleDocument82 pagesMed Surg BundleThe Treasure ChestNo ratings yet
- Med SurgDocument6 pagesMed SurgWANG PUPPYNo ratings yet
- Nero Drugs To KnowDocument14 pagesNero Drugs To KnowGina Giammalvo100% (2)
- CardionotesDocument5 pagesCardionotesNichole Coletta100% (3)
- Basic Drug Cards 3Document14 pagesBasic Drug Cards 3Karima Jones100% (1)
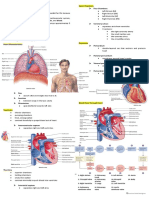
- Chapter 12: HEARTDocument2 pagesChapter 12: HEARTPrecious Faith RodriguezNo ratings yet
- Pharmacology FreebieDocument3 pagesPharmacology FreebieMohammad Farooq Khan50% (2)
- Lab Values - Chart by PriorityDocument2 pagesLab Values - Chart by Priorityashley100% (1)
- Clinical Med CardsDocument26 pagesClinical Med CardsLila Daniels100% (1)
- Pharm 1.11 Insulin Cheat SheetDocument1 pagePharm 1.11 Insulin Cheat SheetSanobar Charania100% (1)
- Understanding ElectrolytesDocument2 pagesUnderstanding Electrolytessurviving nursing schoolNo ratings yet
- Study BundleDocument188 pagesStudy Bundlenazbeen.ahmadi100% (1)
- Pharm SummaryDocument3 pagesPharm Summaryastorm0872No ratings yet
- MedicationsDocument27 pagesMedicationsThe Treasure ChestNo ratings yet
- Heart Blocks: "The Heart Block Poem"Document18 pagesHeart Blocks: "The Heart Block Poem"Bijay Kumar Mahato100% (1)
- Cardiac DrugsDocument4 pagesCardiac DrugsIbrahem Al100% (2)
- 17 Cardiac DrugsDocument6 pages17 Cardiac DrugshiwaralelataNo ratings yet
- IV Fluid Cheat SheetsDocument8 pagesIV Fluid Cheat SheetsNhietz SeraNo ratings yet
- Normal Lab ValuesDocument3 pagesNormal Lab ValuesHNo ratings yet
- Summary of Antidiabetic Drugs PDFDocument3 pagesSummary of Antidiabetic Drugs PDFZinc Yulo100% (1)
- Blood Transfusions : Beautiful NursingDocument1 pageBlood Transfusions : Beautiful NursingMs KillaNo ratings yet
- Endocrine NursingDocument2 pagesEndocrine Nursingsurviving nursing school100% (2)
- Arrythmia Name: Normal Sinus RhythmDocument7 pagesArrythmia Name: Normal Sinus RhythmJulx0100% (1)
- Ncle X Cheat SheetDocument24 pagesNcle X Cheat Sheet98b5jc5hgt100% (1)
- Lab Values Chart 120511 PDFDocument5 pagesLab Values Chart 120511 PDFVanessaMUeller100% (3)
- Clinical Care Plan GuideDocument13 pagesClinical Care Plan Guidej.siemens1d100% (1)
- Med Surg BundleDocument112 pagesMed Surg BundleCynthia Leyva100% (7)
- Urinary SystemDocument9 pagesUrinary SystemCailah Sofia SelausoNo ratings yet
- Pharmacology Bundle Study GuideDocument47 pagesPharmacology Bundle Study GuideAmisalu Nigusie100% (2)
- Mnemonics For NursesDocument52 pagesMnemonics For Nursessweetpearl27100% (3)
- IV Fluids Cheat Sheet Copyright BNDocument2 pagesIV Fluids Cheat Sheet Copyright BNJeshan Yanong BeltranNo ratings yet
- Electrolytes ImbalancesDocument4 pagesElectrolytes ImbalancesPeter John Ruiz100% (2)
- Nursing Pharmacology Perfusion Study GuideDocument9 pagesNursing Pharmacology Perfusion Study GuideChelsea SmithNo ratings yet
- Mnemonics PDFDocument15 pagesMnemonics PDFbeingfiredNo ratings yet
- Bundle Fundamentals of Nursing PDFDocument59 pagesBundle Fundamentals of Nursing PDFسلطان محمد فوزي سلمان100% (1)
- Cardiac Study GuideDocument11 pagesCardiac Study Guidesurviving nursing school100% (2)
- Common Drugs ChartDocument15 pagesCommon Drugs Chartforminsko100% (1)
- MedSurg and Pharm BonusDocument13 pagesMedSurg and Pharm BonusThe Treasure ChestNo ratings yet
- Electrolyte Imbalances TransDocument12 pagesElectrolyte Imbalances TransAndre AndradaNo ratings yet
- Fluid Electrolyte Imbalance n132 160210135651Document100 pagesFluid Electrolyte Imbalance n132 160210135651Shahan FarooqNo ratings yet
- Fluid Electrolyte Imbalance n132 160210135651Document99 pagesFluid Electrolyte Imbalance n132 160210135651Mala AninahNo ratings yet
- 13 Principles of Aseptic TechniqueDocument1 page13 Principles of Aseptic TechniqueMarie Antionette MondragonNo ratings yet
- Care of Clients With Gastrointestinal DisordersDocument4 pagesCare of Clients With Gastrointestinal DisordersMarie Antionette MondragonNo ratings yet
- Brown Abstract Things To Do List and PlannerDocument3 pagesBrown Abstract Things To Do List and PlannerMarie Antionette MondragonNo ratings yet
- NotesDocument4 pagesNotesMarie Antionette MondragonNo ratings yet
- Diagnostic Testing For Urinary System DisordersDocument3 pagesDiagnostic Testing For Urinary System DisordersMarie Antionette MondragonNo ratings yet
- D. NCM 234-Medical ConditionsDocument77 pagesD. NCM 234-Medical ConditionsMarie Antionette MondragonNo ratings yet
- Preop NotesDocument10 pagesPreop NotesMarie Antionette MondragonNo ratings yet
- Spot Mapping of Sitio KawayananDocument1 pageSpot Mapping of Sitio KawayananMarie Antionette MondragonNo ratings yet
- SIRITUAL NEEDS QUESTIONNAIRE (SPQN)Document3 pagesSIRITUAL NEEDS QUESTIONNAIRE (SPQN)Marie Antionette MondragonNo ratings yet
- Record of Newborn CareDocument1 pageRecord of Newborn CareMarie Antionette MondragonNo ratings yet
- B. NCM 234 - SEXUALLY TRANSMITTED DISEASES (Week 3)Document134 pagesB. NCM 234 - SEXUALLY TRANSMITTED DISEASES (Week 3)Marie Antionette MondragonNo ratings yet
- Classification of FatsDocument2 pagesClassification of FatsMarie Antionette MondragonNo ratings yet
- A. NCM 234 - REPRODUCTIVE FUNCTION DISORDERS (Week 3)Document57 pagesA. NCM 234 - REPRODUCTIVE FUNCTION DISORDERS (Week 3)Marie Antionette MondragonNo ratings yet
- Digital Scrapbook - Espina - n1Document15 pagesDigital Scrapbook - Espina - n1Marie Antionette MondragonNo ratings yet
- Fats DeficiencyDocument2 pagesFats DeficiencyMarie Antionette MondragonNo ratings yet
- Importance of LipidsDocument1 pageImportance of LipidsMarie Antionette MondragonNo ratings yet
- Functions of FatDocument2 pagesFunctions of FatMarie Antionette MondragonNo ratings yet
- 6 - The World of RegionsDocument38 pages6 - The World of RegionsMarie Antionette MondragonNo ratings yet
- Why Dragonpay?: Compared With Other Platforms, Fao Can Confirm and Verify Payments Faster Via DragonpayDocument10 pagesWhy Dragonpay?: Compared With Other Platforms, Fao Can Confirm and Verify Payments Faster Via DragonpayMarie Antionette MondragonNo ratings yet
- Line Dance ModuleDocument34 pagesLine Dance ModuleMarie Antionette MondragonNo ratings yet
- DefinitionDocument2 pagesDefinitionMarie Antionette MondragonNo ratings yet
- TimelineDocument12 pagesTimelineMarie Antionette MondragonNo ratings yet
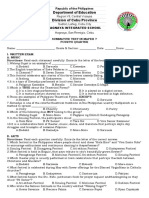
- Department of Education Division of Cebu ProvinceDocument5 pagesDepartment of Education Division of Cebu ProvinceNelsie FernanNo ratings yet
- Trauma - and Stressor-Related DisordersDocument34 pagesTrauma - and Stressor-Related DisordersjenNo ratings yet
- 704 Viet Nam Fact SheetsDocument2 pages704 Viet Nam Fact SheetsKhánh NgôNo ratings yet
- Amonoo 2019Document12 pagesAmonoo 2019zozNo ratings yet
- CD 2022 FundaICN Starters Basic - PDF - FOR REVIEWERDocument15 pagesCD 2022 FundaICN Starters Basic - PDF - FOR REVIEWERMeryville JacildoNo ratings yet
- SmokingDocument3 pagesSmokingKyle OrlanesNo ratings yet
- PEA Glaucoma TreatmentDocument9 pagesPEA Glaucoma TreatmentMenoddin shaikhNo ratings yet
- To Study 1Document69 pagesTo Study 1Alyssa RebeccaNo ratings yet
- ANTINYERIDocument12 pagesANTINYERINunuk HidayantiNo ratings yet
- Literature Review Diabetic Foot CareDocument6 pagesLiterature Review Diabetic Foot Careafdttjcns100% (1)
- Health History Form 03Document2 pagesHealth History Form 03IñakiNo ratings yet
- Colle's FractureDocument22 pagesColle's FractureAkshata HingeNo ratings yet
- Cvac 176Document18 pagesCvac 176Helder LezamaNo ratings yet
- The Blood Sugar Solution: The Ultrahealthy Program For Losing Weight, Preventing Disease, and Feeling Great Now! (The Dr. Mark Hyman Library, 1)Document23 pagesThe Blood Sugar Solution: The Ultrahealthy Program For Losing Weight, Preventing Disease, and Feeling Great Now! (The Dr. Mark Hyman Library, 1)brigitteannemarietrr100% (10)
- Inp RbeDocument13 pagesInp RbeAllaiza CristilleNo ratings yet
- Lingering InjuriesDocument12 pagesLingering Injuriessunrei musicNo ratings yet
- MainDocument7 pagesMainRosul majeedNo ratings yet
- Finbarr C. Martin and Anette Hylen RanhoffDocument13 pagesFinbarr C. Martin and Anette Hylen RanhoffMessias FilhoNo ratings yet
- Recurrent MiscarriageDocument13 pagesRecurrent MiscarriageMerahit AberaNo ratings yet
- Faisal Yunus PIPKRA How Adherence To GOLD Improve The COPD Treatment and Economic Outcomes - 3 Feb 2023-1Document37 pagesFaisal Yunus PIPKRA How Adherence To GOLD Improve The COPD Treatment and Economic Outcomes - 3 Feb 2023-1Muhammad Khairul AfifNo ratings yet
- SBAR Patient CareDocument6 pagesSBAR Patient CareFreddie254No ratings yet
- Unit 1 - Understanding PsychopathologyDocument6 pagesUnit 1 - Understanding Psychopathologybiyaspsy9No ratings yet
- Wu 2017Document12 pagesWu 2017Rashellya RasyidaNo ratings yet
- Bhert Ex - OrderDocument3 pagesBhert Ex - OrderJoy Javier Abonita RazadoNo ratings yet
- Explanation 2021 July 1Document321 pagesExplanation 2021 July 1Reshma Shaji PnsNo ratings yet
- Emergency Nursing (Medical Emergencies - ABC) - StudentsDocument19 pagesEmergency Nursing (Medical Emergencies - ABC) - StudentsAngielyn Ramos OlorazaNo ratings yet
- Laporan Pasien Konsul Divisi Endokrin FauzanDocument2 pagesLaporan Pasien Konsul Divisi Endokrin Fauzanfauzan azhariNo ratings yet
- 8 - Disorders of The GallbladderDocument33 pages8 - Disorders of The Gallbladdersohaib salamehNo ratings yet