Cincinnati Incision Approach for Posterior Ankle and Calcaneal Pathology:
Technique Tip
Zeev Feldbrin, MD1 and Lipkin Alexander, MD1
Ramat Aviv, Israel
Level of Evidence: V, Expert Opinion Beginning in 2000, we have used this incision mainly for the correction of Haglund’s disease and were very Key Words: Haglund’s Disease; Achilles; Cincinnati; satisfied with the operative technique and outcome. As Transverse Crawford et al.3 had stated, the transverse incision was based on a thorough study of the anatomy of the foot, including its INTRODUCTION neurovascular and lymphatic supply. Furthermore, we used only a small part of the possible length of this incision so Haglund’s disease can be approached by various incisions. that only the necessary section of the Achilles tendon and A review of the literature revealed that the traditional the retrocalcaneal area were exposed. The full incision such approach recommended currently by most authors2,6,9 used as one required in clubfoot surgery was not needed. This a longitudinal incision. For years we used the longitudinal transverse incision provided excellent exposure of Haglund’s incision either laterally or medially or combined, according disease, even the cases in which release and reattachment of to the primary affected area, which had been determined part of the Achilles was needed were done easily through by clinical examination. However, we experienced many this approach. problems with this longitudinal incision as described by others (Figure 1) including wound breakdown, iatrogenic SURGICAL TECHNIQUE nerve injury, hypertrophic scarring and keloid formation. The heel scars, which form after this incision, were especially The full extent of the incision, described by Crawford problematic as they often interfered with patient’s ability to et al.3 is not necessary. We use only part of the length wear shoes. according to the needs of a specific case with the length There have been sporadic reports of transverse plantar as long as necessary. Crawford et al.3 began the incision incision used for a calcaneal spur. Carmont and Maffulli1 on the medial aspect of the foot in the region of navicu- use the Cincinnati incision for treating insertional Achilles locuneiform joint and carried it posteriorly, gently curving tendinopathy with detachment of the Achilles. Crawford beneath the distal end of the medial malleolus, and then et al.3 ’s classic article, which popularized the use of the ascending slightly, passed transversely over the Achilles Cincinnati incision for correction of clubfoot in children, was tendon, approximately at the level of the tibiotalar joint. the inspiration for the use of this transverse incision for the From here, the incision continued over the lateral malle- posterior aspect of the ankle (Figure 2). olus until the sinus tarsi. Over the heel, there were three 1 to four transverse skin crests; the incision was made in one Department of Orthopedics, Wolfson Medical Center, Holon, affiliated with Sackler Faculty of Medicine, Tel Aviv University, Ramat Aviv, Israel. of those skin crests, usually in the first or second-most prox- No benefits in any form have been received or will be received from a commercial imal one. The skin crests are parallel with the Langer lines party related directly or indirectly to the subject of this article. so the incision was hidden in those skin crests. Once they Corresponding Author: mature they are difficult to identify and avoid the formation Zeev Feldbrin, MD of unsightly scars. The longitudinal incisions, which cross Wolfson Medical Center Orthopaedic Department the Langer lines, may result in formation of wide, ugly scars 6 Arie Sharon (Figure 1B).5 Tel Aviv, 69553 After making the transverse skin incision, we perform a Israel E-mail: feldbrin@netvision.net.il longitudinal incision along the border of the Achilles, either For information on pricings and availability of reprints, call 410-494-4994, x232. laterally or medially or on both sides as needed.
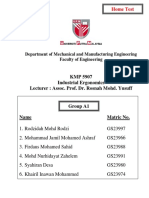
Fig. 5: Good visualization around the Achilles tendon.
2. Coughlin, MJ; Mann, RA: Surgery of the Foot and Ankle, Mosby, St. Fig. 4: Hair-line scar after transverse incision. Louis, 1999. 3. Crawford, AH; Marxen, JL; Osterfeld, DL: The Cincinnati incision: a comprehensive approach for surgical procedures of the foot and ankle and resection of tumors.3 Crawford et al.3 gives the credit for in childhood. J Bone Joint Surg Am. 64(9):1355 – 1358, 1982. this transverse incision to Dr. Nicholas J. Giannestras who 4. Freeman, BJC; Duff, S; Allen, PE; Nickolson, HD; Atkin, RM: The performed a correction of congenital vertical talus using this extended lateral approach to the hindfoot. Anatomic basis and surgical incision. implications. J Bone Joint Surg Br. 80(1):139 – 42, 1998. http://dx.doi. There are several advantages to this incision over the org/10.1302/0301-620X.80B1.7987 5. Gangopadhyay, SG; Packer, G: A comparative study between longi- longitudinal one. First, from the cosmetic point of view, the tudinal and T incision for dorsal plating of the distal radius. J of Hand transverse incision is made parallel to the skin crests. This Surgery. (British and European) 28B(6):568 – 70, 2003. http://dx.doi. type of incision often generates hair-like scars (Figure 4) org/10.1016/S0266-7681(03)00171-2 which are almost invisible after several months, as compared 6. Kitaoka, HB: The Foot and Ankle, Lippincott Williams & Wilkins, to much thicker and sometimes ugly, wide scars which Philadelphia, 2002. 7. Johnson, KW; Zalavras, C; Thordarson, DB: Surgical management remain after a longitudinal one. This transverse incision of insertional calcific achilles tendinosis with a central tendon splitting allows the ideal straightforward approach to both sides of the approach. Foot and ankle int. 27(4):245 – 50, 2006. Achilles tendon (Figure 5), as compared to the longitudinal 8. McGarvey, WC; Palumbo, RC; Baxter, DE; Leibman, BE: one, which provides good visualization of one side only. Insertional Achilles tendonosis: surgical treatment through a central Even when doing two longitudinal incisions simultaneously, tendon splitting approach. Foot Ankle Int., 23(1):19 – 25, 2002. 9. Myerson, MS: Foot and Ankle Disorders, Saunders, Philadelphia, 2000. one cannot approach the tendon itself easily. The sural nerve 10. Self, TC; Kunz, RE; Young, G: Transverse plantar incision for heel is out of danger with this transverse incision. Using this spur surgery. Four-year follow-up survey of 35 patients. J Am Podiatric incision we encountered only minor complications. Med Assoc. 83(5):259 – 62, 1993.
REFERENCES
1. Carmont, MR; Maffulli, N: Management of insertional Achilles
tendinopathy through a Cincinnati incision. BMC Musculoskeletal Disorders, 15(8)82, 2007. http://dx.doi.org/10.1186/1471-2474-8-82