
Milta 4
Milta 4
Uploaded by
Victor RoticivCopyright:
Available Formats
Milta 4
Milta 4
Uploaded by
Victor RoticivOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
Milta 4
Milta 4
Uploaded by
Victor RoticivCopyright:
Available Formats
ED ITORIA LS
Editorials ence in cancer-specific or overall survival has yet been
found (Schroder FH: personal communication). The
Mayo Clinic series, which represents the largest ret-
rospective series, with a nonrandomized control group
and almost three decades of follow-up,5 found that the
E ARLY A NDROGEN D EPRIVATION survival advantage in favor of immediate androgen-
FOR P ROSTATE C ANCER ? deprivation therapy was limited to DNA diploid tu-
mors and became apparent only after 10 years.
T HE dependence of the growth of prostate cancer
on androgens is well documented. Androgen ab-
lation triggers a cascade of biologic events that ends
What explains this difference? It is possible that the
effect of the treatment in the study by Messing et
al. might have been overestimated purely by chance
in irreversible damage to the DNA of androgen-sensi- (a type I error). It seems very unlikely that other stud-
tive prostate-cancer cells.1 Such treatment, tradition- ies would have missed such a large effect, since the
ally reserved for men with metastatic disease, results in hazard ratios ranged from 3 to 12. One concern is
major objective and subjective benefits in most pa- that the study never realized its projected goal of 240
tients. However, in approximately 50 percent of pa- patients. This is important, because the outcome of
tients, disease progression occurs 12 to 18 months patients with nodal metastases is extremely variable
after the initiation of treatment, and as a result, surviv- and can be affected by a number of known and pos-
al rates have not increased over the past five decades.2 sibly unknown prognostic factors.7-9 Such effects on
Androgen ablation controls the tumor only tempo- the outcome of trials can be minimized by random-
rarily because prostate cancer consists of androgen- ization, but the study by Messing et al. was relatively
dependent and androgen-independent clones.1 Tumor small and might have been affected by imbalances of
progression after androgen ablation is due to the pro- factors that had not been identified at the time the
liferation of androgen-independent cells.1 At present, study began. One factor that might have influenced
there is no conclusive evidence that androgen-depri- the outcome is the lack of a central pathological re-
vation therapy improves survival. Undoubtedly, effec- view to assess the Gleason scores.5,7,8 The absence of
tive control of androgen-independent disease will be a correlation between histologic grade and survival
necessary for that to occur. suggests that an imbalance could have been present
A major unresolved issue regarding hormonal ther- but unrecognized.
apy is the optimal time to initiate treatment. In this How will the knowledge that immediate androgen-
issue of the Journal, Messing et al.3 report that men deprivation therapy may be beneficial in men with
with microscopical nodal metastasis (stage T1bN1M0 nodal metastases who have undergone radical prosta-
or T2N1M0) who underwent radical prostatectomy tectomy affect the treatment of prostate cancer? At
and in whom hormonal therapy was begun immedi- present, because of the shift toward earlier diagnosis
ately survived significantly longer than men who were with increased screening efforts, less than 5 percent of
initially treated by radical prostatectomy alone. To patients who undergo radical prostatectomy have pos-
our knowledge, this is the first prospectively ran- itive nodes. Furthermore, as indicated by Messing et
domized therapeutic study in such patients. Overall, al., the patterns of treatment have changed during the
it was well designed, conducted, and analyzed. The past decade, particularly after their study ended. Pa-
treatment groups appear to be reasonably balanced tients with evidence of microscopical nodal involve-
with regard to patient and disease characteristics, thus ment are now unlikely to undergo radical prostatecto-
supporting the likelihood that the estimate of the my. Although this point does not diminish the merits
treatment effect was unbiased. of the study, it may limit its clinical impact.
Nevertheless, the main result is rather surprising: How should physicians treat patients with asympto-
a fairly large difference in survival between groups was matic metastatic prostate cancer? No study has shown
found within a relatively short period. The cancer- conclusively that survival in patients given early andro-
specific survival rate in the observation group was only gen-deprivation therapy is longer than when treatment
62 percent at seven years, as compared with a rate of is deferred until the time of symptomatic progres-
approximately 80 percent in three contemporary se- sion. No advantage was found in the large randomized
ries of patients with microscopical nodal metastases study of patients with prostate cancer, with or with-
who were treated with radical prostatectomy alone.4-6 out extranodal metastases, that was conducted by the
In an ongoing study by the European Organization Veterans Administration Co-operative Urological Re-
for Research and Treatment of Cancer, 302 patients search Group in the 1960s.10 A more recent Medical
with stage D1 disease (which includes nodal but not Research Council study11 reported a significant trend
extranodal metastases) who did not undergo radical toward increased survival with early androgen-depri-
prostatectomy were randomly assigned to receive ei- vation therapy, largely in patients without extranodal
ther immediate or delayed androgen-deprivation ther- metastases. The incidence of spinal cord compression
apy. With a median follow-up of six years, no differ- and pathologic fractures doubled in the deferred-treat-
Vol ume 341 Numb e r 2 4 · 1837
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
ment group. The deferred-treatment group had 54 prostatectomy and pelvic lymphadenectomy in men with node-positive
prostate cancer. N Engl J Med 1999;341:1781-8.
more deaths than the immediate-treatment group. 4. Cadeddu JA, Partin AW, Epstein JI, Walsh PC. Stage D1 (T1-3,N1-3,M0)
However, 29 of these men never received hormonal prostate cancer: a case-controlled comparison of conservative treatment
therapy, indicating that treatment was often initiated versus radical prostatectomy. Urology 1997;50:251-5.
5. Zincke H, Bergstralh EJ, Larson-Keller JJ, et al. Stage D1 prostate cancer
too late or not at all.12 treated by radical prostatectomy and adjuvant hormonal treatment: evi-
Data from other clinical trials indicate that the out- dence for favorable survival in patients with DNA diploid tumors. Cancer
1992;70:Suppl:311-23.
come among patients with metastatic disease who have 6. deKernion JB, Neuwirth H, Stein A, et al. Prognosis of patients with
never received hormonal therapy depends heavily on stage D1 prostate cancer following radical prostatectomy with and without
the extent of disease; this factor may have influenced early endocrine therapy. J Urol 1990;144:700-3.
7. Scrignoli AR, Walsh PC, Steinberg GD, Steiner MS, Epstein JI. Prog-
the outcome of the Medical Research Council trial.13 nostic factors in men with stage D1 prostate cancer: identification of pa-
We need more data on patients with metastatic disease tients less likely to have prolonged survival after radical prostatectomy.
before standards of practice can be clearly delineated. J Urol 1994;152:1077-81.
8. Cheng L, Bergstralh EJ, Cheville JC, et al. Cancer volume of lymph
How should the results of this study affect the treat- node metastasis predicts progression in prostate cancer. Am J Surg Pathol
ment of patients who have elevated serum prostate- 1998;22:1491-500.
9. Bauer JJ, Connelly RR, Sesterhenn IA, et al. Biostatistical modeling us-
specific antigen (PSA) levels after radical prostatecto- ing traditional variables and genetic biomarkers for predicting the risk of
my? In the study by Messing et al., 80 percent of the prostate carcinoma recurrence after radical prostatectomy. Cancer 1997;79:
patients had undetectable serum levels of PSA at the 952-62.
10. Byar DP. Proceedings: the Veterans Administration Co-operative Uro-
time androgen-deprivation therapy was initiated. In logical Research Group’s studies of cancer of the prostate. Cancer 1973;32:
a recent report, Pound et al.14 described the natural 1126-30.
history of 304 patients with an elevated PSA level as 11. The Medical Research Council Prostate Cancer Working Party Inves-
tigators Group. Immediate versus deferred treatment for advanced prostatic
the sole evidence of relapse after radical prostatecto- cancer: initial results of the Medical Research Council Trial. Br J Urol
my. The time at which the PSA level first rose after 1997;79:235-46.
12. Walsh PC. Immediate versus deferred treatment for advanced prostatic
surgery, the Gleason score, and the length of time cancer: initial results of the Medical Research Council Trial. J Urol 1997;
required for PSA levels to double all predicted the 158:1623-4.
probability of distant metastasis. The algorithm that 13. Eisenberger MA, Crawford ED, Wolf M, et al. Prognostic factors in
stage D2 prostate cancer: important implications for future trials: results of
these authors used identifies patients at high risk for a cooperative intergroup study (INT-0036). Semin Oncol 1994;21:613-9.
distant metastasis and death due to prostate cancer 14. Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD,
who should be enrolled in randomized clinical trials Walsh PC. Natural history of progression after PSA elevation following rad-
ical prostatectomy. JAMA 1999;281:1591-7.
of androgen-deprivation therapy and nonhormonal 15. Pollack A, Zagars GK, Kavadi VS. Prostate specific antigen doubling
treatments. It also identifies men with a high prob- time and disease relapse after radiotherapy for prostate cancer. Cancer
1994;74:670-8.
ability of a favorable outcome, for whom watchful
waiting is the most appropriate approach. Although
©1999, Massachusetts Medical Society.
less extensively evaluated, the data on patients with
a biochemical relapse (defined as detectable serum
PSA levels) after radiation therapy appear to be sim-
ilar to those obtained after surgery.15
In summary, the study by Messing et al. is impor- R EDUCING C ARDIAC R ISK
tant because it touches on critical issues concerning IN N ONCARDIAC S URGERY
the treatment of prostate cancer. The most important
message of this study is that although it suggests an
advantage for early androgen-deprivation therapy, that
conclusion is not definitive. It should provide the im-
“A VOID hypotension.” That recommendation
has appeared at the end of many preoperative
consultation notes for patients undergoing major non-
petus for a vigorous exploration of the role of endo- cardiac surgery. This not-so-helpful advice has reflect-
crine and nonendocrine approaches to the adjuvant ed the state of the science of perioperative cardiac risk
treatment of prostate cancer. reduction. A great deal of research provides insight
into how to identify patients at moderate and high
MARIO A. EISENBERGER, M.D. risk.1-4 Very little is known about strategies that might
PATRICK C. WALSH, M.D. improve their outcomes.
Johns Hopkins Medical Institutions The era in which physicians can only guess at how
Baltimore, MD 21287-2101 to reduce a patient’s risk of perioperative cardiac com-
plications seems to be ending, however, as demon-
REFERENCES
strated by the study by Poldermans et al.5 in this is-
1. Denmeade SR, Lin XS, Isaacs JT. Role of programmed (apoptotic) cell sue of the Journal. This randomized trial provides the
death during the progression and therapy for prostate cancer. Prostate
1996;28:251-65. [Erratum, Prostate 1996;28:414.]
first strong evidence that any intervention — medical
2. Schröder FH. Endocrine treatment of prostate cancer. In: Walsh PC, or surgical — reduces the risk of short-term cardiac
Retik AB, Vaughan ED, Wein AJ, eds. Campbell’s urology. 7th ed. Vol. 3. complications associated with vascular surgery. The
Philadelphia: W.B. Saunders, 1998:2627-44.
3. Messing EM, Manola J, Sarosdy M, Wilding G, Crawford ED, Trump results apply most directly to the patients at highest
D. Immediate hormonal therapy compared with observation after radical risk as they undergo the highest-risk vascular proce-
1838 · Dec em b er 9 , 19 9 9
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
ED ITORIA LS
dures. Nevertheless, these findings justify rethinking tagonist bisoprolol? These questions can and should
current strategies of perioperative care for patients un- be addressed in future research.
dergoing major noncardiac procedures in general.6-8 In the meantime, the findings of this study have
All this change may seem surprising, since it results profound implications for the evaluation and treatment
from a study in which just 112 patients were random- of patients undergoing major noncardiac surgery. Cur-
ly assigned to treatment groups and followed for only rent guidelines encourage the use of noninvasive tests
30 days after surgery. The trial was actually designed for ischemia in patients considered to have an inter-
to enroll a total of 266 patients, but it was halted early mediate risk of complications on the basis of clinical
by an independent safety committee according to a data.6-8 Coronary catheterization and revascularization
predetermined rule for stopping the trial. Relatively are commonly performed in patients who have abnor-
few patients were required because the investigators mal test results, despite a lack of data demonstrating
studied a population at unusually high risk (patients that this strategy improves outcomes.12 It seems like-
with abnormal results on stress echocardiography with ly that the cumulative morbidity resulting from three
dobutamine) as they underwent elective abdominal sequential procedures (coronary angiography, coro-
aortic or infrainguinal arterial reconstruction. These nary revascularization, and then a major vascular pro-
researchers had previously found that such patients cedure) would be higher than the 3.4 percent rate of
have a 28 percent rate of perioperative death from major cardiac complications in this study among pa-
cardiac causes or nonfatal myocardial infarction9; 34 tients given bisoprolol. If other investigations confirm
percent of the patients randomly assigned to standard similarly low rates of cardiac complications with beta-
care in the current study had these complications. blocker therapy in such patients, the role of coro-
However, patients randomly assigned to standard care nary angiography and revascularization before non-
plus perioperative treatment with bisoprolol, a selec- cardiac surgery will be greatly diminished.
tive b1-adrenergic–receptor antagonist, had a compli- A subtle but intriguing possibility raised by this
cation rate of only 3.4 percent. study is that the role of noninvasive testing for ische-
This extraordinary 91 percent reduction in the risk mia may also be reduced in the future. Beta-blockers
of cardiac events sounds too good to be true, and per- are generally safe and inexpensive, and they offer
haps future research will show that to be the case. many long-term benefits for patients with coronary
But the findings are consistent with data showing artery disease. Why not just give these drugs to pa-
reductions in perioperative ischemia with beta-block- tients whose risk of cardiac complications, as indicat-
ade10 and similar in direction to those of the only pre- ed by the clinical data, is intermediate or high? This
vious randomized, controlled study of beta-blockers strategy was suggested in 1996 by Bodenheimer,13
in patients undergoing major noncardiac surgery.11 who recommended a decrease in emphasis on pre-
In that trial, Mangano et al. tested the effects of aten- operative risk stratification by means of noninvasive
olol as compared with placebo in a lower-risk group tests. Instead, he advocated increased efforts to pre-
of patients undergoing elective noncardiac surgery. vent, detect, and reduce postoperative ischemia.
Patients randomly assigned to receive atenolol had 55 There are several important controversies still to be
percent lower mortality over two years, but the ben- resolved. Nonetheless, I will suggest some possible
efit became apparent only after the hospitalization. themes for the next generation of guidelines for peri-
Why was the effect of beta-blockade in the study by operative evaluation and risk reduction for patients
Poldermans et al. so much greater — and seen so undergoing major noncardiac surgery:
soon? The reason may be that, in this investigation, an Preoperative risk stratification should be based on
extremely high base-line risk was predicted by both clinical data. My colleagues and I recently described
the characteristics of the patients and the nature of a simple, prospectively validated index for the predic-
the procedures that they underwent. Consequently, tion of cardiac risk in patients undergoing major non-
the opportunity to improve the outcome was con- cardiac surgery.2 It assigns one point to each of six
siderable. clinical factors: a high-risk surgical procedure, a his-
Most patients who undergo noncardiac surgery are tory of ischemic heart disease, a history of congestive
at much lower risk, of course — thus raising the ques- heart failure, a history of cerebrovascular disease, pre-
tion of whether these findings can be generalized to operative treatment with insulin, and a preoperative
other populations. Does beta-blockade reduce risk for serum creatinine concentration greater than 2.0 mg
patients who do not have positive results on nonin- per deciliter (177 µmol per liter).2 This Revised Car-
vasive tests for ischemia? Can this strategy improve diac Risk Index has proved to be more accurate than
outcomes after nonvascular procedures, which carry other published algorithms1,3,4 and has identified a
a lower risk of complications? Is the minimal one-week larger percentage of patients as having intermediate
period of preoperative treatment with a beta-blocker or high risk.
that was used in this study necessary to achieve full Exercise electrocardiography and other noninvasive
protection? Do other beta-blockers offer benefits sim- tests for myocardial ischemia should not be used for peri-
ilar to those of the b1-selective (cardioselective) an- operative risk stratification. These tests are cost effec-
Vol ume 341 Numb e r 2 4 · 1839
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
tive for the outpatient care of patients with chest pain 9. Poldermans D, Amese M, Fioretti PM, et al. Improved cardiac risk strat-
ification in major vascular surgery with dobutamine-atropine stress echo-
syndromes, because they help identify those with high- cardiography. J Am Coll Cardiol 1995;26:648-53.
risk coronary disease who might benefit from revas- 10. Stone JG, Foëx P, Sear JW, Johnson LL, Khambatta HJ, Triner L.
cularization.14,15 However, there is no evidence that Myocardial ischemia in untreated hypertensive patients: effect of a single
small oral dose of a beta-adrenergic blocking agent. Anesthesiology 1988;
the routine use of these tests can improve periopera- 68:495-500.
tive care. They may be an appropriate part of the pre- 11. Mangano DT, Layug EL, Wallace A, Tateo I. Effect of atenolol on
mortality and cardiovascular morbidity after noncardiac surgery. N Engl
operative evaluation of patients whose exercise toler- J Med 1996;335:1713-20. [Erratum, N Engl J Med 1997;336:1039.]
ance is limited or whose clinical risk is unclear. 12. Mangano DT, Goldman L. Preoperative assessment of patients with
Coronary revascularization before noncardiac surgery known or suspected coronary disease. N Engl J Med 1995;333:1750-6.
13. Bodenheimer MM. Noncardiac surgery in the cardiac patient: what
should be recommended only for patients with unstable is the question? Ann Intern Med 1996;124:763-6.
myocardial ischemic syndromes or results indicating a 14. Kuntz KM, Fleischmann KE, Hunink MG, Douglas PS. Cost-effec-
high risk on noninvasive tests for ischemia. There are no tiveness of diagnostic strategies for patients with chest pain. Ann Intern
Med 1999;130:709-18.
data showing that coronary revascularization reduces 15. Garber AM, Solomon NA. Cost-effectiveness of alternative test strat-
complications among patients undergoing elective egies for the diagnosis of coronary artery disease. Ann Intern Med 1999;
130:719-28.
noncardiac surgery; hence, coronary revascularization
should be reserved for patients in whom it would be
©1999, Massachusetts Medical Society.
considered appropriate as part of their routine long-
term care.
In the absence of major contraindications, therapeu-
tic doses of beta-adrenergic antagonists should be given M ILTEFOSINE — T HE
to patients with an intermediate or high risk of cardiac
complications. Patients who are not already receiving L ONG -A WAITED T HERAPY
beta-blockers should be given one of these agents. FOR V ISCERAL L EISHMANIASIS ?
Even if the drug causes complications, such as fatigue
or impotence, these side effects can be tolerated dur-
ing the perioperative period. Patients who are already
receiving a beta-blocker should be evaluated to en-
M ILTEFOSINE was originally developed as an
antineoplastic drug, but it has the potential to
become the first highly effective, orally administered
sure that therapeutic serum concentrations have been drug for treating visceral leishmaniasis, a life-threaten-
achieved. ing parasitic disease. We do not know whether addi-
In summary, the study by Poldermans et al. sug- tional clinical trials and experience with miltefosine
gests that, in the future, perioperative care will be will support the encouraging findings of the phase 2
characterized by fewer tests, fewer coronary revascu- study described by Jha et al. in this issue of the Jour-
larization procedures, more use of beta-blockers — nal.1 However, the prospect of a new drug that is ad-
and fewer complications. ministered orally rather than parenterally is good news
indeed, because the drug could markedly facilitate
THOMAS H. LEE, M.D. the treatment of patients.
Partners Community HealthCare Although asymptomatic or subclinical infection is
Boston, MA 02199 common in some settings, patients with clinically ev-
ident visceral leishmaniasis (or kala-azar, which is Hin-
REFERENCES di for “black sickness” or “black fever”) are typically
1. Goldman L, Caldera DL, Nussbaum SR, et al. Multifactorial index of heavily infected throughout the reticuloendothelial
cardiac risk in noncardiac surgical procedures. N Engl J Med 1977;297: system.2 These patients have fever, cachexia, spleno-
845-50. megaly, and pancytopenia, which can be severe. Ulti-
2. Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and pro-
spective validation of a simple index for prediction of cardiac risk of major mately, the patients die of the disease or of complicat-
noncardiac surgery. Circulation 1999;100:1043-9. ing conditions if they are not treated appropriately.
3. Detsky AS, Abrams HB, McLaughlin JR, et al. Predicting cardiac com-
plications in patients undergoing non-cardiac surgery. J Gen Intern Med
Worldwide, there are estimated to be approximately
1986;1:211-9. 500,000 cases of visceral leishmaniasis per year, and
4. L’Italien GJ, Paul SD, Hendel RC, et al. Development and validation of many of them are associated with epidemics, partic-
a Bayesian model for perioperative cardiac risk assessment in a cohort of
1,081 vascular surgical candidates. J Am Coll Cardiol 1996;27:779-86. ularly in the Indian subcontinent and Sudan.2,3 The
5. Poldermans D, Boersma E, Bax JJ, et al. The effect of bisoprolol on peri- epidemics underscore the need for therapy that not
operative mortality and myocardial infarction in high-risk patients under- only is highly effective and safe, even in patients who
going vascular surgery. N Engl J Med 1999;341:1789-94.
6. Guidelines for perioperative cardiovascular evaluation for noncardiac are critically ill from leishmaniasis and coexisting ill-
surgery: report of the American College of Cardiology/American Heart nesses (e.g., tuberculosis or dysentery), but also is
Association Task Force on Practice Guidelines. Circulation 1996;93:1278-
317.
easily administered and affordable for treating large
7. American College of Physicians. Guidelines for assessing and managing numbers of impoverished patients.
the perioperative risk from coronary artery disease associated with major The latest in the series of epidemics centered in
noncardiac surgery. Ann Intern Med 1997;127:309-12.
8. Palda VA, Detsky AS. Perioperative assessment and management of risk northeastern India flared up in the 1970s, probably
from coronary artery disease. Ann Intern Med 1997;127:313-28. in part because of the discontinuation of insecticide
1840 · Decem b er 9 , 19 9 9
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
ED ITOR IA LS
spraying for malaria, which also affected the phlebot- antileishmanial activity.6,7 On the basis of the success
omine sandflies that transmit leishmaniasis. The ep- of this early work and the safety of the drug in pa-
idemic, which is caused by Leishmania donovani, con- tients with cancer, several phase 1 and 2 clinical trials
tinues to generate as many as hundreds of thousands have been conducted to assess the role of miltefosine
of cases annually.2,3 In recent years, the treatment of as therapy for Indian visceral leishmaniasis.1,8,9 The first
patients with Indian visceral leishmaniasis has been two trials included 30 and 45 patients.8,9 The report
complicated by both the large number of infected peo- by Jha et al. 1 describes the third and largest trial pub-
ple and the declining effectiveness of conventional lished to date. This phase 2 trial, which was con-
parenteral therapy with pentavalent antimonial com- ducted in 1998 and 1999 in India, included 120
pounds.2 Although the lipid formulations of ampho- HIV-negative patients at least 12 years of age, 71 per-
tericin B are an important recent advance in treating cent of whom were male, with mild-to-moderate vis-
visceral leishmaniasis,2 their high cost precludes their ceral leishmaniasis. They were sequentially enrolled in
use where they are most needed, and they require in- four treatment groups, which received regimens that
travenous administration. The availability of an afford- varied according to dose and schedule. The cure rate
able oral agent would benefit patients even in rural was high (95 percent overall), even among patients in
areas and could also serve as a control measure, be- whom antimonial therapy had failed. Twenty-nine of
cause humans are the reservoir hosts of this infection 30 patients (97 percent) were cured with the four-
in India. week regimen of 100 mg of miltefosine per day, which
The excess mortality from an epidemic of L. dono- is now being evaluated further in India in a phase 3
vani infection in the 1980s and 1990s in southern trial (in which the regimen is 50 mg of miltefosine
Sudan, which has been affected by a civil war, has twice daily, with patients who weigh less than 25 kg
been estimated to be about 100,000 deaths among receiving 50 mg once daily). Unpublished data sug-
300,000 persons at risk.4 The availability of an oral gest that three weeks of therapy may be as effective
agent such as miltefosine would have been particu- as four weeks (Sundar S, Murray HW: personal com-
larly helpful during the height of the epidemic, when munication).
Médecins Sans Frontières–Holland treated patients, In the various clinical trials, the toxic effects asso-
sometimes more than 1000 at a time, with daily injec- ciated with miltefosine have usually been tolerable and
tions of pentavalent antimony in outdoor clinics un- reversible, although the therapeutic window appears
der shade trees.4 Although antimonial therapy has re- to be narrow. Gastrointestinal symptoms, such as vom-
mained highly effective in Sudan, there are obvious iting and diarrhea, although common, have typical-
logistic difficulties in providing a month-long course ly been brief and of only mild-to-moderate severity.
of parenteral therapy in such settings. An oral agent Some patients have had reversible hepatotoxicity or
that is effective even for severely debilitated and criti- nephrotoxicity. Although the toxicity associated with
cally ill patients could facilitate patient care in remote miltefosine sounds milder than that with some par-
and difficult-to-serve areas of the world such as Sudan. enteral therapies, gastrointestinal symptoms could be
Visceral leishmaniasis is also problematic in other of more consequence in severely ill patients, such as
settings. For example, in northeastern Brazil, where those who are malnourished or dehydrated, than they
L. chagasi is the etiologic agent and domestic dogs were in the patients in the clinical trials. The treatment
are reservoir hosts, the disease is now found not only of women is complicated by the fact that pregnancy
in rural areas but also in periurban shanty settlements. is a contraindication to the use of miltefosine because
Visceral leishmaniasis has emerged as an AIDS-asso- it is a teratogen in animals.
ciated opportunistic infection, particularly in south- Will miltefosine continue to be highly effective and
ern Europe, where it is caused by L. infantum and acceptably tolerated when more patients are treated?
where 25 to 70 percent of the adults with visceral How broadly applicable will miltefosine therapy be
leishmaniasis are also infected with the human immu- for the diversity encompassed by human leishmania-
nodeficiency virus (HIV) and 1.5 to 9.0 percent of sis, which includes several clinical syndromes, caused
patients with AIDS have newly acquired or reactivat- by about 21 leishmanial species in 88 countries?2,3 Will
ed visceral leishmaniasis.2,5 An oral agent for primary miltefosine become one more option for treating a
and maintenance treatment of patients with visceral particular type of patient, or will it become the drug
leishmaniasis who also have HIV infection would rep- of choice for most patients who require systemic an-
resent an important step forward, particularly if the tileishmanial therapy? We do not know yet. For In-
therapy were effective despite the patients’ immuno- dian visceral leishmaniasis, the ongoing phase 3 trial
suppression and safe despite concomitant treatment will involve 300 HIV-negative adults and adolescents
of other conditions. who will be treated with miltefosine. A phase 1 and 2
Enter the candidate oral agent, miltefosine. Miltef- escalating-dose study in children is also under way.
osine was first investigated in vitro and in animal Studies of other leishmanial syndromes, including
models of visceral leishmaniasis because of the hy- American cutaneous leishmaniasis, are in progress or
pothesis that alkylphospholipid derivatives might have are being planned. Studies of visceral leishmaniasis
Vol ume 341 Numb e r 2 4 · 1841
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
outside India are still needed, as are clinical trials L ESSONS FROM S ECRETIN
that include severely debilitated patients and patients
infected with HIV. In vivo studies are encouraging,
because they indicate that the activity of miltefosine
against L. donovani does not require host T cells or
I N this issue of the Journal, Sandler and colleagues
report the negative results of a double-blind, pla-
cebo-controlled trial of a single intravenous dose of
mechanisms mediated by activated macrophages.10 synthetic human secretin in children with autism or
Could miltefosine, the fruit of careful basic-science pervasive developmental disorder.1 Autistic disorder is
and clinical research, be the long-awaited orally ad- a serious neuropsychiatric disorder with onset in the
ministered drug for treating visceral leishmaniasis? It first years of life that is characterized by delayed and
could be. Optimism tempered by caution is warrant- deviant social and communication skills, associated
ed. Miltefosine could join the list of agents that ap- with various forms of unusual behavior (e.g., repetitive
peared promising but fell by the wayside. However, behavior and unusual responses to the environment).2
the best-case scenario is that miltefosine becomes a The term pervasive developmental disorder not oth-
licensed antileishmanial agent (in 2001, at the earli- erwise specified refers to a condition with symptoms
est), is affordably priced so that it can benefit the pa- suggestive of autism but that does not meet the full
tients who need it the most, proves effective and safe criteria for autism.2
in actual use after licensure, and fundamentally chang- In the years immediately after the first description
es our approach to treating visceral leishmaniasis and of autism in 1943,3 there was speculation that the con-
perhaps other leishmanial syndromes, such that par- dition might be a form of schizophrenia, that it was
enteral therapy is rarely needed. Dare we also hope more frequent in families with higher socioeconomic
for a future in which effective prevention and control status, and that it was not associated with other med-
measures markedly reduce the need for antileishma- ical conditions. Subsequent research has clarified that
nial therapy? autism and related conditions are distinctive disorders,
are seen in all social classes, and are strongly associated
BARBARA L. HERWALDT, M.D., M.P.H.
with some medical conditions, notably seizure disor-
Centers for Disease Control and Prevention der, for which persons with autism are at increased
Atlanta, GA 30341-3724
risk.4,5 Recent work has strongly implicated genetic
REFERENCES factors in causing the disease; it appears that several
genes are probably involved, and several promising
1. Jha TK, Sundar S, Thakur CP, et al. Miltefosine, an oral agent, for the leads have been identified.6
treatment of Indian visceral leishmaniasis. N Engl J Med 1999;341:1795-
800. Studies of treatments for autism and related condi-
2. Herwaldt BL. Leishmaniasis. Lancet 1999;354:1191-9. tions support the importance of structured behavioral
3. Desjeux P. Leishmaniasis: public health aspects and control. Clin Der- and educational intervention.7 Although no pharma-
matol 1996;14:417-23.
4. Seaman J, Mercer AJ, Sondorp HE, Herwaldt BL. Epidemic visceral cologic agent has proved curative, the treatment of
leishmaniasis in southern Sudan: treatment of severely debilitated patients specific symptoms — for example, with neuroleptic
under wartime conditions and with limited resources. Ann Intern Med
1996;124:664-72.
drugs — can greatly aid the child’s ability to be helped
5. Report on the consultative meeting on Leishmania/HIV co-infection, by such programs.8 Despite better detection and im-
Rome, 6–7 September, 1994. Geneva: World Health Organization, 1995. proved services, autism is a major burden for chil-
(WHO/LEISH/95.35.)
6. Kuhlencord A, Maniera T, Eibl H, Unger C. Hexadecylphosphocholine: dren and their families. It affects 1 in approximately
oral treatment of visceral leishmaniasis in mice. Antimicrob Agents Chemo- 2000 children2 and is associated with some degree of
ther 1992;36:1630-4. mental retardation in about 75 percent of cases. In
7. Croft SL, Snowdon D, Yardley V. The activities of four anticancer alkyl-
lysophospholipids against Leishmania donovani, Trypanosoma cruzi and slightly less than half of cases, affected persons never
Trypanosoma brucei. J Antimicrob Chemother 1996;38:1041-7. develop communicative speech.2 Understandably, par-
8. Sundar S, Rosenkaimer F, Makharia MK, et al. Trial of oral miltefosine
for visceral leishmaniasis. Lancet 1998;352:1821-3.
ents often feel overwhelmed and devastated by this
9. Sundar S, Gupta LB, Makharia MK, et al. Oral treatment of visceral diagnosis.
leishmaniasis with miltefosine. Ann Trop Med Parasitol 1999;93:589-97. As noted by Sandler et al.,1 given the absence of a
10. Murray HW, Delph-Etienne S. Visceral leishmanicidal activity of hexa-
decylphosphocholine (miltefosine) in mice deficient in T cells and activated “cure,” it is not surprising that a great number of
macrophage microbicidal mechanisms. J Infect Dis (in press). treatments have been proposed; new treatments, of-
ten accompanied by extravagant claims that they are
©1999, Massachusetts Medical Society. responsible for marked improvement or cure, are re-
ported regularly, although usually with minimal or
inadequate data. In the case of secretin, the impetus
for interest in this drug was the reports in the broad-
cast and print media about a young child with au-
tism who improved dramatically after receiving this
gastrointestinal peptide during a study of pancreatic
function and the report of a small, uncontrolled case
series.9 The widespread media attention and reports
1842 · Dec em b er 9 , 19 9 9
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
ED ITORIA LS
of dramatic improvement and cure led many parents parents to pursue unproven or emerging treatments is
to seek secretin treatment for their children, and the understandable. Treatments that have been consid-
ensuing frenzy led to a black market for the drug. ered over the years include lysergic acid diethylamide,
The interest in secretin was remarkable, because it oc- high-dose glucocorticoids, psychosurgery, and injec-
curred in the absence of substantive data on its po- tions of sheep-brain extract. Clearly, it is important
tential benefit or safety; secretin had been approved by that parents know that some interventions have been
the Food and Drug Administration only for single- proved to be effective and helpful; such treatments
dose use in the diagnosis of certain gastrointestinal should not be lightly abandoned. Examples include
disorders. The safety of repeated administration of se- intensive special education and attention to the child’s
cretin, which in its original form was derived from behavior to improve communication, speech, and oth-
pigs, was unclear, and the potential for sensitization er skills. The attempt to educate professionals by de-
after an initial infusion was a concern. veloping guidelines for the diagnosis and treatment of
Sandler et al. found no significant improvement in autism is welcome in this regard.8,13 Unfortunately,
various outcome measures after a single infusion of claims may be made on the basis of uncontrolled, sin-
secretin, as compared with placebo. In addition, they gle-case reports with all the attendant problems (e.g.,
note that in both the secretin group and the placebo ambiguities regarding diagnosis and the nature of the
group there was a significant decrease in the severity treatment and the fact that some children improve
of symptoms over time (i.e., as a result of the non- without intervention). Pursuing unproven treatments
specific but important effects of being involved in re- risks depleting the financial and psychosocial resourc-
search).10 None of the children treated with secretin es of families.14,15 It is important that physicians help
had treatment-limiting adverse effects in this study, families make informed decisions about treatment for
nor did there seem to be a delayed beneficial effect autism.
of the secretin infusion. The authors also note the The nonspecific gains in behavioral and develop-
interest of many parents in continuing the use of the mental functioning that can be realized as a result
drug in their children, even after the families obtained of being involved in research deserve particular men-
the results of this study. The authors rightly note the tion. These gains highlight the importance of con-
limitations of their study. It will, of course, need rep- trolled research, as well as the potential of system-
lication and extension, although the emerging results atic attention in improving the lives of people with
from other trials of secretin for the treatment of au- autism.10
tism appear to be similar.11
Lessons to be learned from the secretin phenom- FRED R. VOLKMAR, M.D.
enon relate to the relation between medicine and the Yale University School of Medicine
news media, as well as to the nature and treatment New Haven, CT 06520
of autism. The extensive media attention when sub-
stantive supporting data were absent was clearly pre- REFERENCES
mature and unfortunate. Parents scrambled to obtain 1. Sandler AD, Sutton KA, DeWeese J, Girardi MA, Sheppard V, Bodfish
this “cure” for their children in the absence of data on JW. Lack of benefit of a single dose of synthetic human secretin in the
treatment of autism and pervasive developmental disorder. N Engl J Med
safety and efficacy — aided, in some cases, by well- 1999;341:1801-6.
meaning, if not well-informed, health care profession- 2. American Psychiatric Association. Diagnostic and statistical manual. 4th
als. What makes an interesting television program ed. Washington, D.C.: APA Press, 1994.
3. Kanner L. Autistic disturbances of affective contact. Nerv Child 1943;
may not, of course, be the same as what makes good 2:217-50.
science. 4. Rapin I. Autism. N Engl J Med 1997;337:97-104.
Although important findings do sometimes emerge 5. Volkmar FR, Klin A, Cohen DJ. Diagnosis and classification of autism
and related conditions: consensus and issues. In: Cohen DJ, Volkmar FR,
unexpectedly and dramatically, most of the time sci- eds. Handbook of autism and pervasive developmental disorders. New
entific progress is made slowly and incrementally, as York: Wiley, 1997:5-40.
6. Rutter M, Bailey A, Simonoff E, Pickles A. Genetic influences and au-
investigators replicate and extend results of previous tism. In: Cohen DJ, Volkmar FR, eds. Handbook of autism and pervasive
work. In autism, the progress in clarifying the role of developmental disorders. New York: Wiley, 1997:370-87.
genetic factors is one such example.12 Methodical and 7. Harris SL, Handleman JS. Helping children with autism enter the main-
stream. In: Cohen DJ, Volkmar FR, eds. Handbook of autism and perva-
painstaking work, however, may not be particularly sive developmental disorders. New York: Wiley, 1997:665-75.
newsworthy. Will the media devote as much attention 8. Volkmar FR, Cook E, Pomeroy J, Realmuto G, Tanguay P. Practice pa-
and energy to publicizing the negative results report- rameters for the assessment and treatment of children and adolescents with
autism and pervasive developmental disorders. J Am Acad Child Adolesc
ed by Sandler and colleagues as to the apparent initial Psychiatry 1999;38:Suppl:32-54.
success of secretin? From a policy perspective, im- 9. Horvath K, Stefanatos G, Sokolski KN, Wachtel R, Nabors L, Tildon
JT. Improved social and language skills after secretin administration in
proved communication between journalists and inves- patients with autism spectrum disorders. J Assoc Acad Minor Phys 1998;
tigators in the attempt to provide accurate and hon- 9:9-15.
est information to parents is an important but as yet 10. Shapiro AK, Shapiro E. The powerful placebo: from ancient priest to
modern physician. Baltimore: Johns Hopkins University Press, 1997.
often unachieved goal. 11. Owley T, Steele E, Corsello C, et al. A double-blind, placebo-controlled
Given the seriousness of autism, the willingness of trial of secretin for the treatment of autistic disorder. Medscape General
Vol ume 341 Numb e r 2 4 · 1843
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
Medicine 1999 (http://www.medscape.com/medscape/GeneralMedicine/ 14. Sparrow S, Zigler E. Evaluation of a patterning treatment for retarded
journal/1999/v01.n10/mgm1006.owle/mgm1006.owle-01.html). children. Pediatrics 1978;62:137-50.
12. Rutter M. Autism: two-way interplay between research and clinical 15. Mesibov GB. Facilitated communication: a warning for pediatric psy-
work. J Child Psychol Psychiatry 1999;40:169-88. chologists. J Pediatr Psychol 1995;20:127-30.
13. Filipek PA, Accardo PJ, Baranek G, et al. The screening and diagno-
sis of autistic spectrum disorders. J Autism Dev Disord 1999;29:437-
82. ©1999, Massachusetts Medical Society.
1844 · Dec em b er 9 , 19 9 9
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
OC C A S IONA L NOTES
Occasional Notes
D EATH OF A P RESIDENT
I T was the best of times. The last war had ended a
generation earlier, and a European war had just
been avoided. Prosperity was visible. There were new
medicines for frightening diseases. As snow blanket-
ed the Virginia countryside, the young nation’s future
seemed bright. It was the last month of the century:
December 1799.
But on a frigid afternoon, three physicians, gath-
ered around a dying man, were not so optimistic. The
man’s wife looked on as he gasped for air, constantly
shifting position. His aide lay on the bed beside him,
repositioning him, propping up his exhausted frame.
Christopher Sheels, a slave valet, stood beside the dy-
ing man. A porcelain bleeding bowl rested nearby.
After lighting a fire to warm him, slave housemaid
Caroline Branham joined slave seamstress Charlotte
and slave housemaid Molly (surnames unknown) just
inside the doorway. The patient’s eyes were alert and
comprehending. George Washington, who had recent-
ly retired as president of the United States, was pre-
paring to die.1,2
Each physician knew him well. The 69-year-old,
Edinburgh-trained James Craik had frequently visited
the president’s Mount Vernon estate. He and Wash-
Figure 1. The Death of Washington, an 1896 Sketch in Oil by
ington had fought together in the French and Indi-
Howard Pyle (1853–1911).
an Wars. Gustavus Richard Brown, also trained in
The men in the room are Tobias Lear (kneeling), James Craik
Edinburgh, was a wealthy, 52-year-old physician from (standing), and Gustavus Richard Brown (seated). Martha Wash-
Port Tobacco, Maryland, who had just cofounded ington sits at the foot of the bed. This little-known sketch was
the Medical and Chirurgical Faculty of Maryland. published in an 1897 book on George Washington by future
Elisha Cullen Dick, a 37-year-old physician trained in president Woodrow Wilson.3 President Warren Harding’s son also
researched the medical aspects of Washington’s death.4 Cour-
Pennsylvania, was a former quarantine superinten- tesy of the Boston Public Library Print Department.
dent and board-of-health physician in Alexandria,
Virginia. He knew the latest medical literature and
was clinically aggressive. He had been appointed
coroner the previous year. tea with vinegar. Tilting his head back to drip the
Craik, the first physician to arrive, at 9 a.m., ob- mixture down his throat, he nearly suffocated, unable
tained the medical history.1,2 On Friday, December 13, to cough the fluid up. Still alert, he rose and walked
Washington had “taken a cold,” with mild hoarseness. about the bedroom, then sat upright in a chair for
At 2 the next morning, he awoke and had difficulty two hours. Returning to bed, he squirmed to find a
breathing. By 6 a.m., he was febrile, with throat pain comfortable position.
and respiratory distress. Unable to swallow, he spoke Arriving at 3 p.m., Dick argued that further bleed-
with difficulty. His aide, Colonel Tobias Lear, sent for ing might weaken Washington. Craik nevertheless or-
Craik and bloodletter George Rawlins. At about 7:30 dered a fourth bleeding, with the removal of 32 oz
a.m., Rawlins removed 12 to 14 oz (355 to 414 ml) (946 ml) of blood. Brown arrived at 4 p.m., at which
of blood, with Washington requesting additional time calomel (mercurous chloride) and tartar emetic
bloodletting. The mixture of molasses, vinegar, and (antimony potassium tartrate) were administered.
butter Lear gave him brought on nearly fatal choking. Awaiting a therapeutic effect (Fig. 1), the physi-
Craik applied a blister of cantharides to Washing- cians might well have thought about Benjamin Rush,
ton’s throat and removed approximately 18 oz (532 a medical colleague and friend of Washington whose
ml) of blood at 9:30 a.m., with a similar amount re- professional fate was being decided that day. Craik had
moved at 11 a.m. Washington repeatedly gargled sage served with Rush in the Revolutionary War, Brown
Vol ume 341 Numb e r 2 4 · 1845
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
had been his classmate in Edinburgh (class of 1768), set and course of the illness and describing their treat-
and Dick had been his student in Pennsylvania. Amer- ment. Apparently the first justification of a medical
ica’s most famous physician and a signer of the Dec- practice to the American public, the explanation back-
laration of Independence, Rush was fighting allega- fired. That Washington had died at the hands of his
tions of medical malpractice. physicians was immediately suggested by his friends,9
The legal case concerned bloodletting, which Rush as well as by American and British medical scholars10,11
championed. Journalist William Cobbett had charged and the press.12,13 Some 20th-century authors have
Rush with killing patients. Rush had sued. In their charged that he was murdered.14-16
opening statements, the lawyers for the two men trad- Why was 80 oz (2365 ml) of blood removed in
ed blood-tinged metaphors. Rush’s lawyer argued, 12 hours, and was such treatment helpful or harmful?
“[A physician’s] reputation is a fabric delicate as air, The physicians, who did not provide a rationale for
the slightest gust of popular prejudice or caprice dis- this treatment, were nevertheless using accepted “he-
sipates it. . . . Virtue, bleeding at every pore, calls roic” therapy. They understood that Washington’s
for justice on her despoiler.”5 Cobbett’s lawyer quot- condition was inflammatory (subsuming what we now
ed his client, “The times are ominous indeed, when know as infection) and that inflammation was asso-
quack to quack cries purge and bleed.”5 The verdict ciated with tissue swelling, which in turn was related
was scheduled for December 14, as Washington lay to transudation. But they lacked modern antiinflam-
dying. matory therapy. According to some 19th-century his-
After the fourth bloodletting, Washington’s con- torians, Washington’s physicians might have reasoned
dition improved, and he was able to swallow. He that because bloodletting caused visible dermal vaso-
examined his will. Realizing that Sheels had been constriction, it would also constrict the vessels as-
standing for hours, Washington motioned him to sit sociated with swelling in the windpipe17,18 and that
down. Around 5 p.m., Washington again sat up in a the dehydrating effects of “purging” (with the use of
chair but soon returned to bed and was helped into calomel), diaphoresis (with sage tea and subemetic
an upright position. He continued to struggle for air, doses of antimony), and blistering (with cantharides)
and his condition began to deteriorate. At 8 p.m., would potentiate the effect. This speculation may re-
the physicians applied blisters of cantharides to his flect the historians’ a posteriori reasoning.19,20
feet, arms, and legs and then applied wheat-bran cat- In any case, Washington’s blood eventually became
aplasms (poultices) to his throat. His condition de- viscous and flowed slowly,1 presumably reflecting de-
teriorated further. At around 10 p.m., Washington hydration and hypovolemia. Modern physicians would
whispered burial instructions to Lear. doubt the beneficial effects of such therapy on local
At 10:20 p.m., George Washington died. Sheels, inflammatory swelling and would worry that aggres-
Branham, Charlotte, and Molly looked on. Craik sive bleeding might cause weakness and worsen the
closed his friend’s eyelids, while Dick stopped the bed- hypoxia associated with partial airway obstruction;
room clock. The body was carried downstairs and laid they would also worry that iatrogenic dehydration
on a table in the unheated dining room. might lead to electrolyte imbalance. Lacking such
News of Washington’s death spread quickly. Sym- modern concepts, Washington’s physicians may have
bolic funeral services held in hundreds of cities fea- reasoned that with death approaching, “heroic de-
tured elaborate cortèges with empty coffins, riderless pletion” was their only option.
horses, and tolling bells.6 Newspapers published he- What disorder led to Washington’s death? Dick re-
roic poems by grieving women. People made pilgrim- jected Craik’s diagnosis of “inflammatory quinsy” and
ages to Mount Vernon. In France, Napoleon ordered proposed three alternatives: “stridula suffocatis,” “la-
the hanging of black crêpe from flags and standards, ryngea,” or “cynanche tracheitis [sic]”21; the third,
and the marquis de Fontanes delivered a stirring éloge as corrected, eventually prevailed.
(official eulogy) at the temple de Mars (Hôtel des Cynanche trachealis (literally, “dog strangulation”)
Invalides).7 In the American capital, Reverend Rich- was a relatively new diagnostic entity at the time.
ard Allen, minister of the African Methodist Epis- Beginning in the late 1770s, Brown’s teacher, the
copal Church, announced that Washington’s slaves great Edinburgh nosologist William Cullen, defined
would eventually be free. Americans dressed in black it as “inflammation of the glottis, larynx, or upper part
or wore mourning badges for months. of the trachea . . . a rare occurrence . . . [produc-
But amid the sorrow there was controversy over ing] such an obstruction of the passage of the air, as
Washington’s medical care. Rush’s victory in the suffocates, and thereby proves suddenly fatal.”22
bloodletting suit, on the day of Washington’s death, Cynanche could not have been unknown to Wash-
could not eliminate popular suspicion that overuse ington’s physicians. Dick and Craik had been discuss-
of bloodletting was harmful. ing diagnostic possibilities during a “croup” epidemic
Craik and Dick chose a preemptive strike. In an that winter.21 Moreover, one of the earliest and most
open letter to the nation,8 they attributed Washing- authoritative descriptions of cynanche was reported
ton’s death to “cynanche trachealis,” reviewing the on- in 1770 by Brown’s own nephew, also named Gusta-
1846 · Dec em b er 9 , 19 9 9
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
OC C A S IONA L NOTES
vus Brown,23 with subsequent reports by Dick’s teach- the previous evening, as Washington’s illness became
er, Benjamin Rush.24,25 Brown, Craik, and Dick, who critical. Thornton had rushed to Mount Vernon with
probably knew as much about cynanche as any three the same idea as Dick: to perform an emergency tra-
physicians in the United States, even summoned cheotomy.
Brown’s nephew to Washington’s bedside.26 He lived Too late, Thornton still hoped that Washington
in St. Mary’s County, Maryland, however, and failed might be in a suspended state from which he could be
to arrive in time. aroused. After conducting a careful examination of the
Although historians do not agree on the cause corpse, Thornton proposed that the body be thawed
of Washington’s death, the signs and symptoms1,18,19 gradually, first in cool water and then with warm
point to acute bacterial epiglottitis. This diagnosis, blankets and rubbing of the skin, with the subsequent
proposed first in 183827 and several times since,28,29 is performance of a tracheotomy, artificial respiration
consistent with current clinical and epidemiologic in- at the tracheotomy site, and transfusion of lamb’s
formation.30-32 Medical reports during the period from blood.43 Although Martha Washington must have
1776 to 1826 suggest that cynanche trachealis cor- known that her husband had once revived a frozen
responded to the modern diagnosis of bacterial epi- slave thought to be dead, she refused this proposal.
glottitis, but the term was probably also used to refer Thornton and Craik persuaded the family to en-
to some cases of laryngeal diphtheria and viral croup. case the coffin in lead because of the risk of commu-
Other suggested diagnoses seem less likely. Quin- nicable disease.9,44 At the funeral, one of Washing-
sy33 causes unilateral neck swelling, which Washing- ton’s closest friends, Bryan, Lord Fairfax, “caught”
ton did not have, and is seen almost exclusively in a cynanche-like disease. He attributed his survival to
children. Washington had probably been exposed to copious bloodletting.45
streptococci as a child34 and had also apparently had
diphtheria.35 Laryngeal diphtheria was a slowly pro- EPILOGUE
gressive disease largely confined to childhood, as it James Craik apparently never again spoke about
is now, and diphtheria was not prevalent in Virginia the events of December 14. But he did have second
in 1799.28,35 Pneumonia, Ludwig’s angina, Vincent’s thoughts about declining payment, submitting to the
angina, and other proposed diagnoses have largely estate on December 24 a bill for the same fee Brown
been ruled out.28,36-38 and Dick had received at his suggestion. He was also
Could Washington have survived epiglottitis? Dick, bequeathed Washington’s valuable tambour secre-
overruled in his opposition to bloodletting, next ar- tary and circular chair. Craik, who had named one
gued for tracheotomy.21,39 In 1799, even elective tra- of his sons George Washington, attended the death
cheotomy, let alone tracheotomy performed on an of Martha Washington two years later. He died in
emergency basis, was rarely undertaken. It is improb- 1814. One of his grandsons, William Craik, became
able that, at the time of Washington’s illness, trache- a U.S. congressman.
otomy had not been performed in the United States, Meeting over the holidays, Gustavus Richard Brown
as has been claimed,40 although a workable procedure praised Elisha Cullen Dick and said that he wished
had been described in surgical detail only the year they had heeded his advice about bloodletting.26,46
before.41 Undoubtedly, the specter of failure with a Dick, who initially talked of “putting [away] his lan-
grisly, painful (in the absence of anesthesia), and un- cet forever” to become a nurse,26 was less charitable
tried surgical experiment on the former president to his colleagues, later criticizing Brown explicitly and
weighed heavily in Craik’s decision to veto this rad- Craik implicitly.21,39 Brown made no further com-
ical suggestion. ments about Washington’s treatment. Gustavus Brown
One historian has defended Craik by arguing that died in 1801, and Gustavus Richard Brown in 1804.
tracheotomy with the patient in the supine position Dick seems never to have given up revisiting the
would have led to positional ball-and-valve airway clo- events of December 14. Despite his strenuous argu-
sure and rapid death.42 But Dick’s later comments on ments against bloodletting and in favor of tracheot-
tracheotomy specified the upright position.39 Trache- omy, he later reversed himself, arguing that in patients
otomy may have been the only lifesaving option left, with cynanche, bloodletting ad deliquium (to the
but it was not attempted. point of syncope) was so effective it removed the need
After Washington’s death, his physicians spent the for tracheotomy.39 Later still, his preferred treatment
night at Mount Vernon. In the morning, Dick mea- regressed to a “strong toddy” with red pepper. Dick
sured the frozen corpse; it was 1.9 m (6 ft, 31/2 in.) and Rush became national experts on bloodletting as
long. Craik declined payment but recommended that a treatment for cynanche and other diseases, ignor-
Lear pay each of the other two physicians $40 (about ing evidence against its use.47 Dick, who became may-
$375 in 1999 dollars), after which they left. Several or of Alexandria, Virginia, in 1804, remained devoted
hours later, the last physician who had been sum- to Washington’s memory, spearheading both a move-
moned arrived. William Thornton, a physician trained ment to make his birthday a national holiday and the
in Edinburgh and a family friend, had been called erection of a national monument. He died in 1825.
Vol ume 341 Numb e r 2 4 · 1847
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
His grandson, James Alfred Pearce, became a U.S. The last 16 hours of Washington’s life must have
senator. been agonizing as he fought for air, unable to find a
Benjamin Rush’s legal victory invited further attack. comfortable position. His chief concern was appar-
His tormentor, Cobbett, subsequently accused Rush’s ently that his physicians “enable him to die easy.”50
pupil, Dick, of causing Washington’s death. Chased by Though not a Christian, he must have been impatient
Rush’s son, Cobbett escaped a duel and fled to Eng- to reach a “hereafter” with as little trouble as possi-
land, where he became a member of Parliament. Rush, ble. According to Lear’s notes, at the very end, Wash-
who gave the proceeds from his $5,000 judgment ington settled back in bed and appeared calm. His
($47,000 in 1999 dollars) to charity, died in 1813. last act in life was a medical one: he felt his own pulse,
He is remembered today as one of America’s greatest a practice that he had probably picked up in minis-
physicians, a father of psychiatry, and a founder of the tering to his slaves and family. Not even his physi-
liberal humanist tradition in American medicine. cians learned the result as his fingers slipped from his
William Thornton pursued a career as an inventor wrist and his breathing stopped.
and architect, designing the nation’s first Capitol and
developing the city of Washington. He also directed DAVID M. MORENS, M.D.
the patent office, wrote a seminal work on teaching University of Hawaii
deaf–mute persons, codeveloped the first steam- Honolulu, HI 96822
boat, and was involved in many social causes. He
died in 1828. A bibliography (244 entries) on the death of George Washington and
Washington’s will specified that on his wife’s death, related subjects addressed in this report is available from the author on re-
quest. (Please provide a complete address, including e-mail address.)
the slaves he owned at Mount Vernon (about half the
total number) were to be freed. Persuaded by family I am indebted to Mary V. Thompson and Barbara McMillan of
members that this provision of the will might pro- the Mount Vernon Ladies’ Association of the Union; Stephen J. Green-
voke a slave to murder her, Martha Washington freed berg, Elizabeth Tunis, and the staff of the History of Medicine Divi-
sion, National Library of Medicine; George K. Combs of the Lloyd
them all. Sadly, Sheels, Branham, Charlotte, and Mol- House, Alexandria Library; Virginia M. Tanji of the University of
ly had been owned by Mrs. Washington, who was Hawaii; Erlinda Tacadena of Tripler Army Medical Center; Ratna
prevented by inheritance laws from freeing them. Soetjahja Morens; and numerous staff members at the Library of
On her death in 1802, they and the remaining slave Congress for research assistance; to Robert J. Littman for translating
families were dispersed according to those laws. important passages from the Latin; and to Philip K. Wilson and
Peter R. Henriques for valuable suggestions on the manuscript.
Around 1830, as historian Jared Sparks prepared
to write his biography of Washington,48 he tracked REFERENCES
down Caroline Branham, who was at that time owned
1. Lear T. Tobias Lear’s narrative accounts of the death of George Wash-
by Washington’s grandson. The elderly woman gave ington. In: Twohig D, Chase PD, Runge BH, et al., eds. The papers of
Sparks the last eyewitness account of George Wash- George Washington. Retirement series 4: April–December 1799. Char-
ington’s death in exchange for the freedom of her en- lottesville: University Press of Virginia, 1999:542-55.
2. A comparative critique of Washington’s last illness. In: Carroll JA, Ash-
slaved grandson.49 As a free man, the grandson, Rob- worth MW. George Washington. Vol. 7. First in peace. New York: Charles
ert Robinson, left a menial job in a cracker bakery, Scribner’s Sons, 1957:637-53. (Appendix VII-2.)
3. Wilson W. George Washington. New York: Harper & Brothers, 1897:
educated himself, and moved to Alexandria, near (plate illustration follows page 304).
Mount Vernon, where his grandmother had lived as 4. Harding WG II. Oral surgery and the presidents — a century of con-
Washington’s slave. Appointed minister of the Meth- trast. J Oral Surg 1974;32:490-3.
5. (Taken in shorthand by T. Carpenter.) A report of an action for a libel,
odist Church on South Washington Street, he be- brought by Dr. Benjamin Rush, against William Cobbett, in the Supreme
came an influential African-American leader. Court of Pennsylvania, December term, 1799, for certain defamatory pub-
In considering the final illness of George Wash- lications in a news-paper, entitled Porcupine’s Gazette, of which the said
William Cobbett was editor. Philadelphia: W.W. Woodward, 1800.
ington, it is worth remembering that he received 6. George Washington’s invisible corpse and the beaver hat. In: Laderman
prompt and expert medical care that reflected then- G. The sacred remains: American attitudes toward death, 1799–1883. New
Haven, Conn.: Yale University Press, 1996:15-21, 180.
current concepts. In questioning his physicians’ treat- 7. Fontanes L-J-P. Éloge funèbre de Washington, prononcé dans le temple
ment decisions, we should also reflect on the balance de Mars, le 20 pluviôse, an 8. Paris: H. Agasse, 1800.
between art and science in medicine, especially in the 8. Craik J, Dick EC. From “The Times [and District of Columbia Adver-
tiser],” a newspaper printed in Alexandria (Virginia), dated in December,
context of modern therapy for diseases whose patho- 1799. Med Repos 1800;3:311-2.
genesis and natural history are poorly understood 9. Boyd TM. Death of a hero, death of a friend: George Washington’s last
(e.g., atherosclerosis and diabetes mellitus). In 1999, hours. Virginia Cavalcade 1984;33:136-43.
10. Brickell J. Observations on the medical treatment of General Washing-
the treatment of many medical conditions still lacks ton, in his last illness, addressed to his physicians Messrs. Craik and Dick.
a sound scientific or empirical basis. Advances in sci- In: Porcupine P. The Rush-Light. No. II. New York: William Cobbett,
February 28, 1800:81-5.
ence permit us to uncover pitfalls in prior medical 11. Reid J. Observations on the medical treatment of General Washing-
practice but do not by themselves advance the art. ton’s last illness. Med Phys J 1800;3(January–June):473-5.
Thus, physicians must not only continue to develop 12. A note to Dr. Dick. In: Porcupine P. The Rush-Light. No. II. New
York: William Cobbett, February 28, 1800:85-6.
the science of medicine but also maintain and strength- 13. Porcupine P. The American Rush-Light; by the help of which, way-
en its problem-solving aspects and practice as an art. ward and disaffected Britons may see a complete specimen of the baseness,
1848 · Dec em b er 9 , 19 9 9
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
OC C A S IONA L NOTES
dishonesty, ingratitude, and perfidy of Republicans, and of the profligacy, 34. Katz AR, Morens DM. Severe streptococcal infections in historical
injustice, and tyranny of Republican governments. London: J. Wright, perspective. Clin Infect Dis 1992;14:298-307.
1800. 35. Willius FA, Keys TE. The medical history of George Washington
14. Lloyd JU. Who killed George Washington? Eclectic Med J 1923;83: (1732-1799). II. Proceedings of Staff Meetings of the Mayo Clinic 1942;
353-6, 403-8, 453-6. 17:107-12.
15. Marx R. A medical profile of George Washington. American Heritage 36. Brown MW. The famous controversy about Washington’s last illness.
1955;6:43-7, 106-7. Med J Rec 1932;135:39-41.
16. Pirrucello F. How the doctors killed George Washington. Chicago Trib- 37. Barker C. A case report. Yale J Biol Med 1936/1937;9:185-7.
une Magazine. February 20, 1977. 38. George Washington: 1732-1799. In: Wold KC. Mr. President — how
17. Jackson J. Memoir on the last sickness of General Washington and its is your health? St. Paul, Minn.: Bruce Publishing, 1948:1-17.
treatment by the attendant physicians. (Privately printed), 1860. 39. Dick EC. Facts and observations relative to the disease of cynanche
18. Solis-Cohen S. Washington’s death and the doctors. Lippincott’s trachealis, or croup. Philadelphia Med Physical J 1809(May, Suppl 3):242-55.
Monthly Magazine 1899;64:945-52. 40. Reece RL. George Washington: his death and his doctors. Minnesota
19. Reflections on blood-letting. In: King LS. Medical thinking: a histor- Med 1966;49:1185-90.
ical preface. Princeton, N.J.: Princeton University Press, 1982:227-44, 327. 41. Desault PJ. Mémoire sur la bronchotomie & sur les moyens d’y sup-
20. Therapeutic change. In: Warner JH. The therapeutic perspective: pléer en certains cas. In: Bichat M-F-X, ed. Oeuvres chirurgicales de P.J.
medical practice, knowledge, and identity in America, 1820–1885. Cam- Desault, chirurgien en chef du grand Hospice d’Humanité, ci-devant Hôtel-
bridge, Mass: Harvard University Press, 1986:83-161. Dieu de Paris; ou tableau de sa doctrine & de sa pratique dans le traitement
21. Nydegger JA. The last illness of George Washington. Med Rec 1917; des maladies externes. Seconde Partie. Maladies des parties molles. Paris:
92:1128. C.Ve. Desault, 1798:212-53.
22. Of the quinsy, or cynanche. In: Cullen W. First lines of the practice of 42. Scheidemandel HH. Did George Washington die of quinsy? Arch Oto-
physic. Vol. 1. Chapter 5. Edinburgh, Scotland: C. Elliott, 1784:278-306. laryngol 1976;102:519-21.
23. Brown G. Disputatio medica inauguralis de cynanche phlogistica. Ed- 43. Thornton W. (Untitled manuscript catalogued as “Miscellaneous writ-
inburgi, Scotland: Balfour, Auld, et Smellie, 1770. ing on sleep.”) Library of Congress, The Papers of William Thornton, doc-
24. Rush B. (Unfound newspaper article on cynanche trachialis [sic]). In: ument page 3057.
Corner GW, ed. The autobiography of Benjamin Rush: his “Travels through 44. Idem. (Untitled letter to John Marshall, dated from the City of Wash-
Life” together with his Commonplace Book for 1789-1813. Westport, ington, January 2, 1800.) Library of Congress, The Papers of William
Conn.: Greenwood Press, 1948:82. Thornton, document pages 378-9.
25. Observations on the cynanche trachealis. In: Rush B. Medical inquiries 45. Fairfax B. (Untitled letter, probably to the Earl of Buchan, dated from
and observations. Vol. 2. 3rd ed. Philadelphia: Thomas and William Bradford Mount Eagle, near Alexandria, Virginia, 18 January 1800.) Original in the
et al., 1809:373-81. Bodleian Library, Oxford, England. Accession no. RM-100. Catalog no.
26. Washington’s physicians, diseases and death. In: Blanton WB. Medicine PS-2261. (Photostat copy at the Mount Vernon Ladies’ Association of the
in Virginia in the 18th century. Richmond, Va.: Garrett & Massie, 1931: Union, Mount Vernon, Va.)
297-312. 46. Brown GR. (Letter designated “Dr. Brown to Dr. Craik,” January 2,
27. Marsh H. Cases of acute inflammation confined to the epiglottis. Dub- 1800.) In: Ford WC, ed. Last illness and death: the writings of George
lin J Med Sci 1838;13:1-23. Washington. Vol. 14. New York: G.P. Putnam’s Sons, 1893:243-67[257f ].
28. Wells WA. Last illness and death of Washington. Virginia Medical 47. Smith TW. Observations on the medical treatment of the croup. Phil-
Monthly 1927;53:629-42. adelphia Medical Museum 1808;4:31-5.
29. Estes JW. George Washington and the doctors: treating America’s first 48. Sparks J. The life of George Washington. Boston: Ferdinand Andrews,
superhero. Med Heritage 1985;1:44-57. 1839.
30. Frantz TD, Rasgon BM, Quesenberry CP Jr. Acute epiglottitis in 49. The Custis family. In: Powell MG. The history of old Alexandria, Vir-
adults: analysis of 129 cases. JAMA 1994;272:1358-60. ginia, from July 13, 1749 to May 24, 1861. Book II. Richmond, Va.: Wil-
31. Berg S, Trollfors B, Nylén O, Hugosson S, Prellner K, Carenfelt C. liam Byrd Press, 1928:241-9.
Incidence, aetiology, and prognosis of acute epiglottitis in children and 50. Corner GW, ed. The autobiography of Benjamin Rush: his “Travels
adults in Sweden. Scand J Infect Dis 1996;28:261-4. through Life” together with his Commonplace Book for 1789-1813. West-
32. Trollfors B, Nylén O, Carenfelt C, et al. Aetiology of acute epiglottitis port, Conn.: Greenwood Press, 1948:245-9.
in adults. Scand J Infect Dis 1998;30:49-51.
33. Of the death, funeral, and family. In: Prussing EE. The estate of
George Washington, deceased. Boston: Little, Brown, 1927:17-23. ©1999, Massachusetts Medical Society.
Vol ume 341 Numb e r 2 4 · 1849
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
tive (not declarative). Also include a running head of fewer than 40
letter spaces; the name(s) of the author(s), including the first name(s)
and no more than two graduate degrees; the name of the department
and institution in which the work was done; the institutional affilia-
tion of each author; and the name and address of the author to whom
INFORMATION FOR AUTHORS reprint requests should be addressed. Any grant support that requires
acknowledgment should be mentioned on this page.
ABSTRACTS Provide on a separate page an abstract of not more
These guidelines are in accordance with the “Uniform Requirements for than 250 words. This abstract should consist of four paragraphs, la-
Manuscripts Submitted to Biomedical Journals.” (The complete document
beled Background, Methods, Results, and Conclusions. They should
appears in N Engl J Med 1997;336:309-15.)
briefly describe, respectively, the problem being addressed in the
study, how the study was performed, the salient results, and what the
MANUSCRIPTS Manuscripts containing original material are ac- authors conclude from the results.
cepted for consideration if neither the article nor any part of its essen- KEY WORDS Three to 10 key words or short phrases should be
tial substance, tables, or figures has been or will be published or sub- added to the bottom of the abstract page; these will help us index the
mitted elsewhere before appearing in the Journal. This restriction article and may be published with the Abstract. Use terms from the
does not apply to abstracts or press reports published in connection Medical Subject Headings from Index Medicus.
with scientific meetings. Authors should submit to the Editor copies REFERENCES References must be triple-spaced and numbered con-
of any published papers or other manuscripts in preparation or sub- secutively as they are cited. References first cited in tables or figure leg-
mitted elsewhere that are related to the manuscript to be considered ends must be numbered so that they will be in sequence with references
by the Journal. The Journal discourages the submission of more than cited in the text. The style of references is that of Index Medicus. List
one article dealing with related aspects of the same study. all authors when there are six or fewer; when there are seven or more,
Submit an original manuscript with one set of original figures list the first three, then “et al.” The following is a sample reference:
and two copies of the complete manuscript. Manuscripts must be
1. Lahita R, Kluger J, Drayer DE, Koffler D, Reidenberg MM. Antibodies
no longer than 3000 words. Please supply a word count (not includ- to nuclear antigens in patients treated with procainamide or acetylprocain-
ing abstract or references). Use standard-sized paper, and triple-space amide. N Engl J Med 1979;301:1382-5.
throughout. Address all submissions to the Editor, New England Jour-
nal of Medicine, 10 Shattuck St., Boston, MA 02115-6094. A covering Numbered references to personal communications, unpublished
letter signed by all authors should identify the person (with the address data, and manuscripts either “in preparation” or “submitted for pub-
and telephone number) responsible for negotiations concerning the lication” are unacceptable (see “Permissions”). If essential, such ma-
manuscript; the letter should make it clear that the final manuscript terial may be incorporated in the appropriate place in the text.
has been seen and approved by all authors and that they have taken TABLES Double-space tables and provide a title for each. If an ar-
due care to ensure the integrity of the work. At least one person’s name ticle is accepted, the Journal will arrange to deposit extensive tables
must accompany a group name — e.g., Thelma J. Smith, for the Bos- of important data with the National Auxiliary Publications Service
ton Porphyria Group. As stated in the Uniform Requirements (see (NAPS); we will pay for the deposit and add an appropriate footnote
above), credit for authorship requires substantial contributions to: (a) to the text. This service makes available microfiche or photocopies of
conception and design, or analysis and interpretation of data; and (b) tables at moderate charges to those who request them.
the drafting of the article or critical revision for important intellectual ILLUSTRATIONS Figures should be professionally designed. Sym-
content. If more than 12 authors are listed for a multicenter trial, or bols, lettering, and numbering should be clear and large enough to
more than 8 for a study from a single institution, each author must remain legible after the figure has been reduced to fit the width of a
sign a statement attesting that he or she fulfills the authorship criteria single column.
of the Uniform Requirements. No more than 12 names will be listed The back of each figure should include the sequence number, the
under the title; other names will appear in a footnote. Acknowledg- name of the author, and the proper orientation (e.g., “top”). Do not
ments will be limited to a column of Journal space, and those acknowl- mount the figure on cardboard. Photomicrographs should be cropped
edged will be listed only once. (See editorial, Nov. 21, 1991, issue.) to a width of 8 cm, and electron photomicrographs should have in-
LETTERS TO THE EDITOR See the Journal correspondence section. ternal scale markers.
CONFLICT OF INTEREST Authors of research articles should dis- If photographs of patients are used, either the subjects should not
close at the time of submission any financial arrangement they may have be identifiable or their pictures must be accompanied by written per-
with a company whose product figures prominently in the submitted mission to use the figure. Permission forms are available from the
manuscript or with a company making a competing product. Such in- Editor.
formation will be held in confidence while the paper is under review Legends for illustrations should be triple-spaced on a separate sheet
and will not influence the editorial decision, but if the article is accepted and should not appear on the illustrations.
for publication, the editors will usually discuss with the authors the Color illustrations are encouraged. Send both transparencies and
manner in which such information is to be communicated to the reader. prints for this purpose.
Because the essence of reviews and editorials is selection and inter- ABBREVIATIONS Except for units of measurement, abbreviations
pretation of the literature, the Journal expects that authors of such are discouraged. Consult Scientific Style and Format: The CBE Manual
articles will not have any financial interest in a company (or its com- for Authors, Editors, and Publishers (Sixth edition. New York: Cam-
petitor) that makes a product discussed in the article. bridge University Press, 1994) for lists of standard abbreviations. The
COPYRIGHT Authors agree to execute copyright transfer forms as first time an abbreviation appears it should be preceded by the words
requested. Copyright in any contribution is owned by the Massachu- for which it stands.
setts Medical Society. The Society and its licensees have the right to DRUG NAMES Generic names should generally be used. When
use, reproduce, transmit, derivate, publish, and distribute the contri- proprietary brands are used in research, include the brand name in pa-
bution, in the Journal or otherwise, in any form or medium. Authors rentheses in the Methods section.
will not use or authorize the use of the contribution without the So- PERMISSIONS Materials taken from other sources must be accom-
ciety’s written consent, except as may be allowed by U.S. fair use law. panied by a written statement from both author and publisher giving
UNITS OF MEASUREMENT Authors should express all measure- permission to the Journal for reproduction.
ments in conventional units, with Système International (SI) units Obtain permission in writing from at least one author of papers still
given in parentheses throughout the text. Figures and tables should in press, unpublished data, and personal communications.
use conventional units, with conversion factors given in legends or REVIEW AND ACTION Manuscripts are examined by the editorial
footnotes. In accordance with the Uniform Requirements, however, staff and are usually sent to outside reviewers. We encourage authors
manuscripts containing only SI units will not be returned for that to suggest the names of possible reviewers, but we reserve the right of
reason. final selection. Only one copy of rejected manuscripts will be re-
TITLES AND AUTHORS’ NAMES With the manuscript, provide a turned, usually within six weeks. Decisions about potentially accept-
page giving the title of the paper; titles should be concise and descrip- able manuscripts may take longer.
1850 · Dec em b er 9 , 19 9 9
The New England Journal of Medicine
Downloaded from nejm.org at NYU WASHINGTON SQUARE CAMPUS on July 18, 2015. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.
You might also like
- NEJM - 15 year outcomes after monitoring, surgery and rt for prostate cancerNo ratings yetNEJM - 15 year outcomes after monitoring, surgery and rt for prostate cancer12 pages
- Dose Escalation For Oligometastatic Disease Is MoNo ratings yetDose Escalation For Oligometastatic Disease Is Mo2 pages
- Issues and Unmet Needs in Advanced Prostate CancerNo ratings yetIssues and Unmet Needs in Advanced Prostate Cancer9 pages
- Antitumor Effects of Octreotide LAR, A Somatostatin AnalogNo ratings yetAntitumor Effects of Octreotide LAR, A Somatostatin Analog2 pages
- Androgen Receptor Blockade As Treatment of Triple Negative Metastatic Breast CancerNo ratings yetAndrogen Receptor Blockade As Treatment of Triple Negative Metastatic Breast Cancer4 pages
- Medullary Thyroid Cancer in The Era of Tyrosine Kinase Inhibitors: To Treat or Not To Treat-And With Which Drug-Those Are The QuestionsNo ratings yetMedullary Thyroid Cancer in The Era of Tyrosine Kinase Inhibitors: To Treat or Not To Treat-And With Which Drug-Those Are The Questions7 pages
- Psa Persistentemente Elevado Post P RadicalNo ratings yetPsa Persistentemente Elevado Post P Radical20 pages
- Giant Prolactinomas: Multi-Modal Approach To Achieve Tumor ControlNo ratings yetGiant Prolactinomas: Multi-Modal Approach To Achieve Tumor Control2 pages
- Rana R Mckay Outcomes of Post Neoadjuvant IntenseNo ratings yetRana R Mckay Outcomes of Post Neoadjuvant Intense9 pages
- The Role of Free PSA in The Detection of Prostate Cancer: Your Lab FocusNo ratings yetThe Role of Free PSA in The Detection of Prostate Cancer: Your Lab Focus5 pages
- Phase II Study of Pomegranate Juice For Men With Rising Prostate-Specific Antigen Following Surgery or Radiation For Prostate CancerNo ratings yetPhase II Study of Pomegranate Juice For Men With Rising Prostate-Specific Antigen Following Surgery or Radiation For Prostate Cancer9 pages
- Actividad Física Como Prevención de Enfermedades A Largo Plazo.No ratings yetActividad Física Como Prevención de Enfermedades A Largo Plazo.11 pages
- Perspectives On The Treatment Of: Acute Myeloid LeukemiaNo ratings yetPerspectives On The Treatment Of: Acute Myeloid Leukemia7 pages
- Myasthenia Gravis Related To Thymic Carcinoma: A Case Study: Address For CorrespondenceNo ratings yetMyasthenia Gravis Related To Thymic Carcinoma: A Case Study: Address For Correspondence4 pages
- Short-Term Metronidazole Not Linked To CancerNo ratings yetShort-Term Metronidazole Not Linked To Cancer1 page
- Beta-Blocker Drug Use and Survival Among Patients With Pancreatic AdenocarcinomaNo ratings yetBeta-Blocker Drug Use and Survival Among Patients With Pancreatic Adenocarcinoma9 pages
- Article. Neoadjuvant Treatment Response As An Early Response Indicator For Patients With Rectal CancerNo ratings yetArticle. Neoadjuvant Treatment Response As An Early Response Indicator For Patients With Rectal Cancer7 pages
- evaluation-of-tumor-growth-in-treatment-of-murine-melanoma-bytransdermal-infusion-of-etoposide-by-radiofrequency-2155-9554-1000325No ratings yetevaluation-of-tumor-growth-in-treatment-of-murine-melanoma-bytransdermal-infusion-of-etoposide-by-radiofrequency-2155-9554-10003251 page
- Nanomedicine and Cancer Research And Textbook 5From EverandNanomedicine and Cancer Research And Textbook 5No ratings yet
- Functional Gene Correction For Cystic Fibrosis inNo ratings yetFunctional Gene Correction For Cystic Fibrosis in7 pages
- A Comparative Study of Five Technologically Diverse Testing PlatformsNo ratings yetA Comparative Study of Five Technologically Diverse Testing Platforms7 pages
- (Reference Series in Phytochemistry) Sumita Jha (Eds.) - Transgenesis and Secondary Metabolism-Springer International Publishing (2017)No ratings yet(Reference Series in Phytochemistry) Sumita Jha (Eds.) - Transgenesis and Secondary Metabolism-Springer International Publishing (2017)652 pages
- Leishmaniasis: Dr. Kazi Shihab Uddin Mbbs MRCP (Uk) Associate Professor & HOD Department of Internal MedicineNo ratings yetLeishmaniasis: Dr. Kazi Shihab Uddin Mbbs MRCP (Uk) Associate Professor & HOD Department of Internal Medicine20 pages
- Study Guide of Medical Parasitology, Part 1. ProtozoologyNo ratings yetStudy Guide of Medical Parasitology, Part 1. Protozoology50 pages
- Current Affairs - October 2024_1st_chapterNo ratings yetCurrent Affairs - October 2024_1st_chapter33 pages
- Chapter 36 - Visceral Leishmaniasis and TrypanosomiasisNo ratings yetChapter 36 - Visceral Leishmaniasis and Trypanosomiasis99 pages
- Conn With Chomicz Et Al 2016 BioMed Research International Special Issue Newly Emerging Parasitic ThreatsNo ratings yetConn With Chomicz Et Al 2016 BioMed Research International Special Issue Newly Emerging Parasitic Threats74 pages
- The Leishmaniases-Old-Neglected-Tropical-Diseases-2018 PDFNo ratings yetThe Leishmaniases-Old-Neglected-Tropical-Diseases-2018 PDF249 pages
- National Vector Borne Disease Control Programme (NRHM - Common Review Mission)No ratings yetNational Vector Borne Disease Control Programme (NRHM - Common Review Mission)36 pages
- Bihar Current Affairs - May 2024 To August-MergedNo ratings yetBihar Current Affairs - May 2024 To August-Merged52 pages



















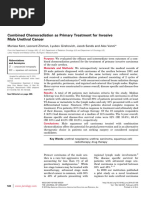

















































































- NEJM - 15 year outcomes after monitoring, surgery and rt for prostate cancerNEJM - 15 year outcomes after monitoring, surgery and rt for prostate cancer
- Issues and Unmet Needs in Advanced Prostate CancerIssues and Unmet Needs in Advanced Prostate Cancer
- Antitumor Effects of Octreotide LAR, A Somatostatin AnalogAntitumor Effects of Octreotide LAR, A Somatostatin Analog
- Androgen Receptor Blockade As Treatment of Triple Negative Metastatic Breast CancerAndrogen Receptor Blockade As Treatment of Triple Negative Metastatic Breast Cancer
- Medullary Thyroid Cancer in The Era of Tyrosine Kinase Inhibitors: To Treat or Not To Treat-And With Which Drug-Those Are The QuestionsMedullary Thyroid Cancer in The Era of Tyrosine Kinase Inhibitors: To Treat or Not To Treat-And With Which Drug-Those Are The Questions
- Giant Prolactinomas: Multi-Modal Approach To Achieve Tumor ControlGiant Prolactinomas: Multi-Modal Approach To Achieve Tumor Control
- The Role of Free PSA in The Detection of Prostate Cancer: Your Lab FocusThe Role of Free PSA in The Detection of Prostate Cancer: Your Lab Focus
- Phase II Study of Pomegranate Juice For Men With Rising Prostate-Specific Antigen Following Surgery or Radiation For Prostate CancerPhase II Study of Pomegranate Juice For Men With Rising Prostate-Specific Antigen Following Surgery or Radiation For Prostate Cancer
- Actividad Física Como Prevención de Enfermedades A Largo Plazo.Actividad Física Como Prevención de Enfermedades A Largo Plazo.
- Perspectives On The Treatment Of: Acute Myeloid LeukemiaPerspectives On The Treatment Of: Acute Myeloid Leukemia
- Myasthenia Gravis Related To Thymic Carcinoma: A Case Study: Address For CorrespondenceMyasthenia Gravis Related To Thymic Carcinoma: A Case Study: Address For Correspondence
- Beta-Blocker Drug Use and Survival Among Patients With Pancreatic AdenocarcinomaBeta-Blocker Drug Use and Survival Among Patients With Pancreatic Adenocarcinoma
- Article. Neoadjuvant Treatment Response As An Early Response Indicator For Patients With Rectal CancerArticle. Neoadjuvant Treatment Response As An Early Response Indicator For Patients With Rectal Cancer
- evaluation-of-tumor-growth-in-treatment-of-murine-melanoma-bytransdermal-infusion-of-etoposide-by-radiofrequency-2155-9554-1000325evaluation-of-tumor-growth-in-treatment-of-murine-melanoma-bytransdermal-infusion-of-etoposide-by-radiofrequency-2155-9554-1000325
- Fast Facts: Prostate Cancer: If, when and how to interveneFrom EverandFast Facts: Prostate Cancer: If, when and how to intervene
- Fast Facts: Molecular Profiling in Solid TumorsFrom EverandFast Facts: Molecular Profiling in Solid Tumors
- Nanomedicine and Cancer Research And Textbook 5From EverandNanomedicine and Cancer Research And Textbook 5
- A Comparative Study of Five Technologically Diverse Testing PlatformsA Comparative Study of Five Technologically Diverse Testing Platforms
- (Reference Series in Phytochemistry) Sumita Jha (Eds.) - Transgenesis and Secondary Metabolism-Springer International Publishing (2017)(Reference Series in Phytochemistry) Sumita Jha (Eds.) - Transgenesis and Secondary Metabolism-Springer International Publishing (2017)
- Leishmaniasis: Dr. Kazi Shihab Uddin Mbbs MRCP (Uk) Associate Professor & HOD Department of Internal MedicineLeishmaniasis: Dr. Kazi Shihab Uddin Mbbs MRCP (Uk) Associate Professor & HOD Department of Internal Medicine
- Study Guide of Medical Parasitology, Part 1. ProtozoologyStudy Guide of Medical Parasitology, Part 1. Protozoology
- Chapter 36 - Visceral Leishmaniasis and TrypanosomiasisChapter 36 - Visceral Leishmaniasis and Trypanosomiasis
- Conn With Chomicz Et Al 2016 BioMed Research International Special Issue Newly Emerging Parasitic ThreatsConn With Chomicz Et Al 2016 BioMed Research International Special Issue Newly Emerging Parasitic Threats
- The Leishmaniases-Old-Neglected-Tropical-Diseases-2018 PDFThe Leishmaniases-Old-Neglected-Tropical-Diseases-2018 PDF
- National Vector Borne Disease Control Programme (NRHM - Common Review Mission)National Vector Borne Disease Control Programme (NRHM - Common Review Mission)