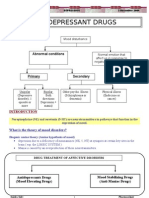
Anti Depressant
Anti Depressant
Download as docx, pdf, or txt
You might also like
- Antidepressant Comparison ChartDocument3 pagesAntidepressant Comparison Chartiggyputtty100% (31)
- Cognition PsychosisDocument100 pagesCognition PsychosisNadia LoveNo ratings yet
- Medical ToxicologyDocument283 pagesMedical ToxicologyMunera SultanNo ratings yet
- Antidepressant DrugsDocument47 pagesAntidepressant DrugsOjambo Flavia80% (5)
- Black Book of NursesDocument46 pagesBlack Book of Nursesmichaeluriel100% (10)
- CNS Drugs-2Document34 pagesCNS Drugs-2semessor021245No ratings yet
- Anti Depressant DrugsDocument31 pagesAnti Depressant DrugsR A H U LNo ratings yet
- Antidepressant AgentsDocument3 pagesAntidepressant AgentsBern NerquitNo ratings yet
- Antidepressant Juli 2016Document18 pagesAntidepressant Juli 2016NadiarosmaliaNo ratings yet
- Psychopharma 1Document7 pagesPsychopharma 1Mitchee Zialcita100% (1)
- Anti Dep.Document6 pagesAnti Dep.Amir AlhaidaryNo ratings yet
- Anti Dep Press AntsDocument19 pagesAnti Dep Press Antsgollaveeresh457No ratings yet
- Antidepressants UOLDocument85 pagesAntidepressants UOLYahya AhmedNo ratings yet
- Psychotropic DrugsDocument11 pagesPsychotropic DrugscchatrumaNo ratings yet
- Anti Depresan1Document39 pagesAnti Depresan1Akmal SafwanNo ratings yet
- PCOL 1 PREFINALS PART 3 eDocument5 pagesPCOL 1 PREFINALS PART 3 eJillian Mae DacerNo ratings yet
- AntidepressantsDocument5 pagesAntidepressantsUm HamoOd100% (2)
- Anti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCDocument17 pagesAnti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCÑiťhišh Śhankąŕ LóganáthánNo ratings yet
- Margo-7 New - VersionDocument27 pagesMargo-7 New - VersionKhushman KaurNo ratings yet
- Lecture 5Document7 pagesLecture 5danaelawadyNo ratings yet
- Pharmacology (All Lectures)Document283 pagesPharmacology (All Lectures)Youssef ElzataryNo ratings yet
- Anti Depressant DrugsDocument14 pagesAnti Depressant Drugs9127084416rcnNo ratings yet
- Antidepressants EDocument58 pagesAntidepressants EBasit IqbalNo ratings yet
- Systemic Effects of Histamine and SerotoninDocument5 pagesSystemic Effects of Histamine and SerotoninibrahimNo ratings yet
- Drugs For Psyciatric DisordersDocument19 pagesDrugs For Psyciatric Disordersapi-36993610% (1)
- Not Associated With Significant Weight GainDocument9 pagesNot Associated With Significant Weight GainDima MasadehNo ratings yet
- AntiConvulsants Drugs in Brief PDFDocument28 pagesAntiConvulsants Drugs in Brief PDFSunilNo ratings yet
- Kappa Uptake of Choline: Pharmacology1-FinalsDocument8 pagesKappa Uptake of Choline: Pharmacology1-FinalsJered OlarveNo ratings yet
- Antidepressants Final PDFDocument7 pagesAntidepressants Final PDFareebaNo ratings yet
- Adrenoceptor - Activating Other Sympathomimetic Drugs PDFDocument43 pagesAdrenoceptor - Activating Other Sympathomimetic Drugs PDFRupal RaghuwanshiNo ratings yet
- Pharmacology CNS DrugsDocument7 pagesPharmacology CNS DrugsDavid Hosam100% (1)
- 23) Mood Altering Drugs: ClassificationDocument2 pages23) Mood Altering Drugs: ClassificationTherealmodeyNo ratings yet
- 44 Adverse Drug Reactions v3Document32 pages44 Adverse Drug Reactions v3a7medtygaNo ratings yet
- Antiseizure DrugsDocument10 pagesAntiseizure DrugsJoyce SumagaysayNo ratings yet
- Therapeutic Drug MonitoringDocument4 pagesTherapeutic Drug MonitoringJhannette RosendoNo ratings yet
- Pharmacology Lec 4 - Converted-1Document14 pagesPharmacology Lec 4 - Converted-171122090No ratings yet
- Antidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyDocument38 pagesAntidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyVinod GuruNo ratings yet
- Drug Cheat SheetDocument6 pagesDrug Cheat SheetSheldon LordNo ratings yet
- Anti-Depressants: Soumya Mary 1 Year MSC (N)Document22 pagesAnti-Depressants: Soumya Mary 1 Year MSC (N)Salman HabeebNo ratings yet
- Drugs Acting On Cns - Dd22Document29 pagesDrugs Acting On Cns - Dd22vabinh.dd2022No ratings yet
- Drugs HandoutDocument9 pagesDrugs Handoutekwamboka956No ratings yet
- Barbiturates: of Action of GABA. Independent of GABADocument10 pagesBarbiturates: of Action of GABA. Independent of GABAAvi WerdesheimNo ratings yet
- Pharmacholgy Antidepressants...Document19 pagesPharmacholgy Antidepressants...Adan IsrarNo ratings yet
- Antidepressents XyzDocument82 pagesAntidepressents XyzAnuranjan VishwakarmaNo ratings yet
- Sedative Hypnotic DrugsDocument80 pagesSedative Hypnotic DrugsNaomi YsabelleNo ratings yet
- Anti Epileptic DrugsDocument89 pagesAnti Epileptic DrugsInderjeet SohalNo ratings yet
- AutocoidsDocument5 pagesAutocoidsMitvinder SinghNo ratings yet
- Therapeutic Drug MonitoringDocument5 pagesTherapeutic Drug MonitoringJanielle Medina FajardoNo ratings yet
- 5th Antidepressant DrugDocument12 pages5th Antidepressant DrugZahraa Mahdi JumaNo ratings yet
- Drug Table 2Document10 pagesDrug Table 2jvanessam703No ratings yet
- Antidepressants: HistoryDocument8 pagesAntidepressants: HistoryTejus Murthy A GNo ratings yet
- AntidepressantDocument29 pagesAntidepressantGrace Natasha SibaraniNo ratings yet
- NeuropharmacologyDocument30 pagesNeuropharmacologytracy_lau_8No ratings yet
- Antidepressants DESKTOP MHAO1SHDocument19 pagesAntidepressants DESKTOP MHAO1SHjanemwanza003No ratings yet
- Cholinergic AntagonistsDocument3 pagesCholinergic Antagonistszkhan260No ratings yet
- 3, Antiepileptic DrugsDocument39 pages3, Antiepileptic DrugsAbebe TilahunNo ratings yet
- Antiemetic DrugsDocument16 pagesAntiemetic DrugswekesacarrenNo ratings yet
- Toxicology: by Group 4 2018/2019 Tan Geok Eng Reena DewiDocument59 pagesToxicology: by Group 4 2018/2019 Tan Geok Eng Reena DewiTan Geok EngNo ratings yet
- Top DrugsDocument7 pagesTop DrugsGracian Vel AsocsomNo ratings yet
- Antidepressants AntidepressantsDocument38 pagesAntidepressants AntidepressantsjaneNo ratings yet
- CNS Depressants: - Sedatives and Hypnotics - General Anesthetics - Narcotic AnalgesicsDocument118 pagesCNS Depressants: - Sedatives and Hypnotics - General Anesthetics - Narcotic Analgesicsbiruk getahunNo ratings yet
- AntidepressantsDocument20 pagesAntidepressantsvimalaNo ratings yet
- Top 100 Drugs Pocket Reference Guide (2023 Edition)From EverandTop 100 Drugs Pocket Reference Guide (2023 Edition)No ratings yet
- Quiz PsychopharmacologyDocument1 pageQuiz PsychopharmacologySolsona Natl HS Maananteng100% (1)
- Peripheral NeuropathyDocument36 pagesPeripheral NeuropathySantiago HerreraNo ratings yet
- Chapter 11, 16 and 17 - Depressive Disorder, Suicide and Bipolar Disorders - Summer 2020Document109 pagesChapter 11, 16 and 17 - Depressive Disorder, Suicide and Bipolar Disorders - Summer 2020Haley Vest MustaficNo ratings yet
- Monoamine Oxidase InhibitorsDocument14 pagesMonoamine Oxidase InhibitorsMary Ann DimayugaNo ratings yet
- Pharmacology QuizesDocument30 pagesPharmacology QuizesRM DemetilloNo ratings yet
- Clin Tox Lab 1Document4 pagesClin Tox Lab 1Czariana Cassidy MagbanuaNo ratings yet
- Notes FileDocument78 pagesNotes FileSEIYADU IBRAHIM K100% (1)
- Antidepressants - AMBOSSDocument7 pagesAntidepressants - AMBOSSOpio IsaacNo ratings yet
- An Overview of Behavioral Disorders and Its Therapeutic Management in Dogs and CatsDocument12 pagesAn Overview of Behavioral Disorders and Its Therapeutic Management in Dogs and CatsDr N B ShridharNo ratings yet
- 52 Q. Medicine 2nd Half PDFDocument15 pages52 Q. Medicine 2nd Half PDFFahad2036No ratings yet
- 1 PBDocument3 pages1 PBJovie MasongsongNo ratings yet
- Clomipramine PDFDocument18 pagesClomipramine PDFddandan_2No ratings yet
- Dina-Farouk Q - A NotesDocument120 pagesDina-Farouk Q - A Notesraju niraulaNo ratings yet
- Chapter 5 - Depression - 2018 - Integrative MedicineDocument13 pagesChapter 5 - Depression - 2018 - Integrative MedicineandreNo ratings yet
- Treatment of Diabetic Neuropathy - UpToDateDocument20 pagesTreatment of Diabetic Neuropathy - UpToDateKarina MilaréNo ratings yet
- Neurobiology and Neuroprotective Benefits of Sleep.4 PDFDocument23 pagesNeurobiology and Neuroprotective Benefits of Sleep.4 PDFchanguito17No ratings yet
- Management of Poisoning and OverdoseDocument36 pagesManagement of Poisoning and OverdoseAtiqa AslamNo ratings yet
- MEDSCAPE ACCOUNT QT - Association of Antipsychotic and Antidepressant Drugs With Q-T Interval ProlongationDocument11 pagesMEDSCAPE ACCOUNT QT - Association of Antipsychotic and Antidepressant Drugs With Q-T Interval ProlongationHesbon MomanyiNo ratings yet
- Pharmacology MnemonicsDocument17 pagesPharmacology MnemonicsJuvenis SampangNo ratings yet
- Antidepressants (Igor Iezhitsa) Students Copy (ME219)Document40 pagesAntidepressants (Igor Iezhitsa) Students Copy (ME219)Zobayer AhmedNo ratings yet
- Care of Clients With Maladaptive Patterns of Behavior1Document188 pagesCare of Clients With Maladaptive Patterns of Behavior1Kissy Besario100% (1)
- Anti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCDocument17 pagesAnti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCÑiťhišh Śhankąŕ LóganáthánNo ratings yet
- PAIN PresentationDocument24 pagesPAIN PresentationLarasati RamadianiNo ratings yet
- Effexor/Effexor XR (Venlafaxine) : General InformationDocument5 pagesEffexor/Effexor XR (Venlafaxine) : General InformationAchmad HariyantoNo ratings yet
- 4 Lowry JA Pediatric Pharmaceutical Ingestions Pediatr Ann 2017 Dec 1Document8 pages4 Lowry JA Pediatric Pharmaceutical Ingestions Pediatr Ann 2017 Dec 1Daniela JaramilloNo ratings yet