1) Many obstetricians believe that pushing during labor increases the risk of retinal detachment (RD), but evidence shows this belief is not supported.
2) Two surveys of obstetricians found that the majority recommended assisted delivery for patients with RD risk factors based on personal opinion rather than evidence.
3) Pushing during labor does not pose a risk of rhegmatogenous RD, the most common type, as it is caused by breaks or tears in the retina unrelated to labor pressures. Exudative RD seen in preeclampsia also has a different cause.
4) In conclusion, labor does not increase the risk of RD, so obstetric decisions need not consider this and o
1) Many obstetricians believe that pushing during labor increases the risk of retinal detachment (RD), but evidence shows this belief is not supported.
2) Two surveys of obstetricians found that the majority recommended assisted delivery for patients with RD risk factors based on personal opinion rather than evidence.
3) Pushing during labor does not pose a risk of rhegmatogenous RD, the most common type, as it is caused by breaks or tears in the retina unrelated to labor pressures. Exudative RD seen in preeclampsia also has a different cause.
4) In conclusion, labor does not increase the risk of RD, so obstetric decisions need not consider this and o
1) Many obstetricians believe that pushing during labor increases the risk of retinal detachment (RD), but evidence shows this belief is not supported.
2) Two surveys of obstetricians found that the majority recommended assisted delivery for patients with RD risk factors based on personal opinion rather than evidence.
3) Pushing during labor does not pose a risk of rhegmatogenous RD, the most common type, as it is caused by breaks or tears in the retina unrelated to labor pressures. Exudative RD seen in preeclampsia also has a different cause.
4) In conclusion, labor does not increase the risk of RD, so obstetric decisions need not consider this and o
1) Many obstetricians believe that pushing during labor increases the risk of retinal detachment (RD), but evidence shows this belief is not supported.
2) Two surveys of obstetricians found that the majority recommended assisted delivery for patients with RD risk factors based on personal opinion rather than evidence.
3) Pushing during labor does not pose a risk of rhegmatogenous RD, the most common type, as it is caused by breaks or tears in the retina unrelated to labor pressures. Exudative RD seen in preeclampsia also has a different cause.
4) In conclusion, labor does not increase the risk of RD, so obstetric decisions need not consider this and o
12643 2020;22:103–5 The Obstetrician & Gynaecologist Commentary http://onlinetog.org
Risk of retinal detachment during labour: beliefs versus
evidence Abdallah A Ellabban FRCS Msc PhD,*a,b Ajay D Patil FRCOphth,c David Yorston FRCOphth,d Tom H Williamson FRCOphth, David A Laidlaw FRCOphth,e Colin J Vize FRCOphth,a Edward P Morris e MRCOG f
a Consultant Ophthalmologist, Department of Ophthalmology, Hull University Teaching Hospitals NHS Trust, Anlaby Rd, Hull HU3 2JZ, UK b Lecturer of Ophthalmology, Suez Canal University, 6 Ring Rd, Ismailia 41111, Egypt c Specialty Trainee Year 6, Department of Ophthalmology, Leeds Teaching Hospitals NHS Trust, Great George St, Leeds LS1 3EX, UK d Consultant Ophthalmologist, Gartnavel General Hospital, 1053 Great Western Rd, Glasgow G12 0YN, UK e Consultant Ophthalmologist, Guy’s and St Thomas’ NHS Foundation Trust, 20 St Thomas St, London SE1 9RS, UK f Department of Obstetrics and Gynaecology, Norfolk and Norwich University Hospital, Colney Ln, Norwich NR4 7UY, UK *Correspondence: Abdallah A Ellabban. Email: ellabbanabdallah@gmail.com
Accepted on 9 May 2019. Published online 17 January 2020.
Obstetricians’ opinions of the risk of retinal
Introduction detachment caused by labour Some obstetricians believe that forcible pushing during A questionnaire-based study of obstetricians from different labour increases the risk of retinal detachment (RD). This countries asked for their opinion regarding the is of particular concern to clinicians if the woman has a recommended method of delivery in women with history of RD or is known to be at risk for RD due to high previous RD. The survey showed that the majority of myopia, peripheral retinal degeneration or previous respondents (76%) recommended assisted delivery – either treatment for a retinal tear. This has led some obstetricians caesarean section or instrumental delivery.1 The decision to advocate for assisted delivery or for referring the patient to was mainly influenced by personal opinion rather than ophthalmology for advice regarding mode of delivery.1–5 evidence. The decision to proceed with assisted delivery This brief Commentary will address common beliefs was often taken without consulting an ophthalmologist.1 among obstetricians regarding the risk of RD during labour In another survey, Inglesby et al. sent a questionnaire to compared with evidence from the literature. randomly selected UK obstetricians and almost three-quarters
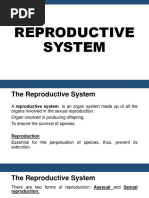
Figure 1. Pathogenesis of rhegmatogenous retinal detachment (RD). (A) Wide-field fundus picture of the right eye showing a superotemporal RD. There is a horseshoe retinal tear (white arrow) and localised areas of RD (white arrowheads). (B) Schematic diagram depicting the pathogenesis of rhegmatogenous RD. Initially, the vitreous gel liquefies and detaches from the back of the eye. This process is called posterior vitreous detachment (PVD) or separation. With eye movements, the detached vitreous gel moves within the vitreous cavity, causing traction on the peripheral retina (yellow arrow) and creating a retinal tear. The liquefied vitreous fluid escapes through the tear into the subretinal space (black curved arrow) and dissects the neurosensory retina, leading to progression of the detachment. This is by far the most common pathogenesis of rhegmatogenous RD. Occasionally, rhegmatogenous RD may occur secondary to a retinal hole without PVD, particularly in young myopes. The liquified vitreous escapes through the hole dissecting the neurosensory retina, leading to the progression of the retinal detachment.
ª 2020 Royal College of Obstetricians and Gynaecologists 103
Risk of retinal detachment during labour
considered a history of RD surgery to be an indication for Serous or exudative RD is caused by exudation of fluid into assisted delivery.2 In a retrospective study conducted in Poland the subretinal space in the absence of retinal breaks or traction. by Socha et al., 100 (2.04%) of 4895 caesarean sections were This can occur in a variety of vascular, inflammatory or performed for ocular reasons, including high myopia, risk of neoplastic diseases of the retina or choroid. In these disorders, RD, history of RD, glaucoma and retinopathy.4 fluid leaks from abnormal retinal or choroidal vessels and The obstetricians’ main concern was that pushing during accumulates under the retina. Exudative RD is well known to the second stage of labour might lead to elevated intraocular obstetricians as it may occur in about 10% of women with pressure (IOP), and that this would increase the risk of RD. eclampsia, and rarely in women with pre-eclampsia.9 It is often associated with signs of hypertensive retinopathy and other systemic comorbidities. This type of RD does not require Pathogenesis and risk of retinal surgery and usually resolves within a few weeks of delivery, with detachment during labour a good visual prognosis.9 Affected women should only undergo RD refers to the separation of the inner neurosensory retina caesarean delivery for obstetric reasons. from the underlying retinal pigment epithelium (RPE), and encompasses two types: rhegmatogenous (rhegma, meaning a Conclusion ‘rent/break’ in Greek), and non-rhegmatogenous RD. There may be some confusion about the terms used to Rhegmatogenous retinal detachment describe different types of RD, particularly rhegmatogenous In clinical ophthalmology or obstetric practice, RD RD, which is not related to pregnancy or labour, and commonly refers to rhegmatogenous RD. In this type, there exudative RD, which occasionally is seen in cases of pre- is a full-thickness defect in the neurosensory retina (tear or eclampsia or eclampsia. These two types of RD have hole) that allows fluid in the vitreous cavity to enter the completely different pathogeneses. subretinal space, leading to detachment of the retina The action of ‘bearing down’ during labour can occa- (Figure 1). This is by far the most common presentation of sionally cause innocuous subconjunctival haemorrhage, and RD. The risk factors for rhegmatogenous RD include high very rarely retinal bleeding as Valsalva retinopathy, but does myopia, peripheral retinal degeneration, vitreoretinopathy not pose any risk for rhegmatogenous RD.10 or previous cataract surgery. Elevated IOP does not increase There is no clinical or theoretical evidence that vaginal the risk of rhegmatogenous RD. Rhegmatogenous RD delivery increases the risk of rhegmatogenous RD. Therefore, usually requires surgery to close the retinal break and there is no reason to alter the management plan for women reattach the retina.6 with a history of rhegmatogenous RD or those considered at In the past, three studies have investigated the risk of risk of RD. Similarly, there is no indication for additional rhegmatogenous RD in women identified as being at risk, routine eye examinations in women considered to be at and they did not find any correlation between labour and the increased risk of this type of RD. Ophthalmology referrals are risk of rhegmatogenous RD.5,7,8 As stated previously, only required if patients develop visual symptoms. rhegmatogenous RD is due to a break in the retina Obstetricians, and the women they care for, may be allowing fluid in the vitreous cavity to enter the subretinal confident that their decisions regarding management of space; there is no reason why this should be affected by labour will have little or no impact on the woman’s pushing during labour. risk of RD.
Non-rhegmatogenous retinal detachment Disclosure of interests
Non-rhegmatogenous RD can either be tractional or There are no conflicts of interest. serous (exudative). In both conditions, the neurosensory retina detaches from the underlying RPE, but there is no Contribution to authorship retinal break. Tractional RD occurs when the retina is AAE wrote and edited the article. ADP, DY, THW, DAL, CJV pulled off the RPE by tractional bands or membranes in and EPM reviewed and critically revised the article. All the absence of retinal tears. This type of retinal detachment authors approved the final version. occurs in retinovascular disorders such as proliferative diabetic retinopathy, retinopathy of prematurity, or sickle References cell disease. Tractional RD may require surgery if the central vision is threatened. The pathogenesis of tractional 1 Papamichael E, Aylward GW, Regan L. Obstetric opinions regarding the RD is unrelated to pregnancy or labour. Women with method of delivery in women that have had surgery for retinal detachment. JRSM Short Rep 2011;2:24. tractional RD are suitable for normal labour and 2 Inglesby DV, Little BC, Chignell AH. Surgery for detachment of the retina vaginal delivery. should not affect a normal delivery. BMJ 1990;300:980.
104 ª 2020 Royal College of Obstetricians and Gynaecologists
Risk of retinal detachment during labour
3 Chiu H, Steele D, McAlister C, Lam W-C. Delivery recommendations for 7 Neri A, Grausbord R, Kremer I, Ovadia J, Treister G. The management of pregnant females with risk factors for rhegmatogenous retinal detachment. labor in high myopic patients. Eur J Obstet Gynecol Reprod Biol Can J Ophthalmol 2015;50:11–8. 1985;19:277–9. 4 Socha MW, Piotrowiak I, Jagielska I, Kazdepka-Zieminska A, Szymanski M, 8 Landau D, Seelenfreund MH, Tadmor O, Silverstone BZ, Diamant Y. The Zalewska M, et al. [Retrospective analysis of ocular disorders and frequency effect of normal childbirth on eyes with abnormalities predisposing to of cesarean sections for ocular indications in 2000–2008 – our own rhegmatogenous retinal detachment. Graefes Arch Clin Exp Ophthalmol experience]. Ginekol Pol 2010;81:188–91. 1995;233:598–600. 5 Elsherbiny SM, Benson MT. Retinal detachment and the second stage of 9 Dornan KJ, Mallek DR, Wittmann BK. The sequelae of serous retinal labour: a survey of regional practice and literature review. J Obstet Gynaecol detachment in preeclampsia. Obstet Gynecol 1982;60:657–63. 2003;23:114–7. 10 Eneh A, Almeida D. Valsalva hemorrhagic retinopathy during labour: 6 Ghazi NG, Green WR. Pathology and pathogenesis of retinal detachment. a case report and literature review. Can J Ophthalmol 2013;48: Eye (Lond) 2002;16:411–21. e145–7.
ª 2020 Royal College of Obstetricians and Gynaecologists 105