Piab 003
Piab 003
Uploaded by
yuwengunawan7Copyright:
Available Formats
Piab 003
Piab 003
Uploaded by
yuwengunawan7Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
Piab 003
Piab 003
Uploaded by
yuwengunawan7Copyright:
Available Formats
Journal of the Pediatric Infectious Diseases Society
ORIGINAL ARTICLE
Management and Outcomes in Children with Third-
Generation Cephalosporin-Resistant Urinary Tract
Infections
Marie E. Wang,1 Tara L. Greenhow,2 Vivian Lee,3 Jimmy Beck,4 Michael Bendel-Stenzel,5 Nicole Hames,6 Corrie E. McDaniel,4 Erin E. King,5
Whitney Sherry,6 Deepika Parmar,7,a Sara T. Patrizi,7,b Nivedita Srinivas,1,8 and Alan R. Schroeder,1,9
1
Division of Pediatric Hospital Medicine, Stanford University School of Medicine and Lucile Packard Children’s Hospital Stanford, Stanford, California, USA, 2Division of Infectious
Diseases, Kaiser Northern California, San Francisco, California, USA, 3Division of Hospital Medicine, Children’s Hospital Los Angeles and Department of Pediatrics, University
of Southern California Keck School of Medicine, Los Angeles, California, USA, 4Department of Pediatrics, University of Washington School of Medicine and Seattle Children’s
Downloaded from https://academic.oup.com/jpids/article/10/5/650/6140794 by guest on 12 February 2024
Hospital, Seattle, Washington, USA, 5Division of Hospital Medicine, Children’s Minnesota, Minneapolis, Minnesota, USA, 6Division of Pediatric Hospital Medicine, Emory
University School of Medicine and Children’s Healthcare of Atlanta, Atlanta, Georgia, USA, 7Department of Pediatrics, Kaiser Northern California, Oakland, California, USA,
8
Division of Pediatric Infectious Diseases, Stanford University School of Medicine, Stanford, California, USA, and 9Division of Pediatric Critical Care Medicine, Stanford University
School of Medicine, Stanford, California, USA
Background. Third-generation cephalosporin-resistant urinary tract infections (UTIs) often have limited oral antibiotic op-
tions with some children receiving prolonged parenteral courses. Our objectives were to determine predictors of long parenteral
therapy and the association between parenteral therapy duration and UTI relapse in children with third-generation cephalosporin-
resistant UTIs.
Methods. We conducted a multisite retrospective cohort study of children <18 years presenting to acute care at 5 children’s
hospitals and a large managed care organization from 2012 to 2017 with a third-generation cephalosporin-resistant UTI from
Escherichia coli or Klebsiella spp. Long parenteral therapy was ≥3 days and short/no parenteral therapy was 0–2 days of concordant
parenteral antibiotics. Discordant therapy was antibiotics to which the pathogen was non-susceptible. Relapse was a UTI from the
same organism within 30 days.
Results. Of the 482 children included, 81% were female and the median age was 3.3 years (interquartile range: 0.8-8). Fifty-
four children (11.2%) received long parenteral therapy (median duration: 7 days). Predictors of long parenteral therapy included
age <2 months (adjusted odds ratio [aOR] 67.3; 95% confidence interval [CI]: 16.4-275.7), limited oral antibiotic options (aOR 5.9;
95% CI: 2.8-12.3), and genitourinary abnormalities (aOR 5.4; 95% CI: 1.8-15.9). UTI relapse occurred in 1 of the 54 (1.9%) children
treated with long parenteral therapy and in 6 of the 428 (1.5%) children treated with short/no parenteral therapy (P = .57). Of the 105
children treated exclusively with discordant antibiotics, 3 (2.9%, 95% CI: 0.6%-8.1%) experienced UTI relapse.
Conclusions. Long parenteral therapy was associated with age <2 months, limited oral antibiotic options, and genitourinary ab-
normalities. UTI relapse was rare and not associated with duration of parenteral therapy. For UTIs with limited oral options, further
research is needed on the effectiveness of continued discordant therapy.
Key words. children; treatment; urinary tract infection.
Urinary tract infections (UTIs), one of the most common are caused by extended-spectrum beta-lactamase (ESBL)-
bacterial infections in children [1], have shown increasing producing organisms [3]. Children hospitalized with ESBL
antimicrobial resistance over the last 2 decades [2, 3]. An esti- UTIs have significantly longer lengths of stay than children
mated 5% of pediatric community-acquired UTIs worldwide with non-ESBL UTIs, resulting in patient/family stress, in-
creased costs, and potential for iatrogenic harm [3–5]. The
increased length of stay has been attributed to the transition
that occurs from empiric discordant therapy (in vitro non-
Received 9 May 2020; editorial decision 28 December 2020; accepted 6 January 2021;
Published online February 17, 2021. susceptibility of the pathogen to the antibiotic) to definitive
a
Present Affiliation: UCSF Benioff Children’s Hospital, San Francisco, CA, USA. concordant therapy and prolonged parenteral courses due to
b
Present Affiliation: Stanford University School of Medicine and Lucile Packard Children’s
Hospital Stanford, Stanford, CA, USA.
limited oral antibiotic options [3, 4].
Corresponding Author: Marie E. Wang, MD, MPH, Division of Pediatric Hospital Medicine, The American Academy of Pediatrics (AAP) UTI guide-
Stanford University School of Medicine, 300 Pasteur Drive MC 5776, Stanford, CA, USA. E-mail:
lines state that most children can be treated orally but do not
marie.wang@stanford.edu.
Journal of the Pediatric Infectious Diseases Society 2021;10(5):650–8
offer specific recommendations for resistant organisms [6].
© The Author(s) 2021. Published by Oxford University Press on behalf of The Journal of the Given that these infections have fewer oral antibiotic options,
Pediatric Infectious Diseases Society. All rights reserved. For permissions, please e-mail:
journals.permissions@oup.com.
more data are needed regarding their optimal management.
DOI: 10.1093/jpids/piab003 Resistance to third-generation cephalosporins is often used as
650 • jpids 2021:10 (May) • Wang et al
a surrogate marker for ESBL UTIs due to lack of ESBL testing at prior 6 months or had underlying malignancy or immunode-
some laboratories [2]. ficiency), had a complex chronic condition (except for renal
We recently reported results from a multisite study abnormalities) [10], did not have a patient encounter docu-
demonstrating that most children with third-generation mented or a urinalysis associated with the urine culture, were
cephalosporin-resistant UTIs started empirically on discordant transferred to/from an outside facility, had a concurrent bacte-
antibiotics improved by the time urine cultures resulted (typi- rial infection requiring prolonged antibiotics (eg, meningitis),
cally after 2-3 days) [7]. In this investigation, we describe the or had a UTI in the prior 30 days, to ensure that captured cases
definitive management and outcomes of these children with were index cases and not relapses. Only one case per patient
third-generation cephalosporin-resistant UTIs after urine cul- was included. Patients were identified through microbiology or
ture results are finalized. Our objectives were to determine pre- medical record query and site investigators reviewed charts to
dictors of long (≥3 days) concordant parenteral therapy and to confirm eligibility and extract demographic, clinical, and lab-
evaluate the association between duration of parenteral therapy oratory data. For the 5 children’s hospitals, all eligible cases
and UTI relapse. were included. For the large managed care organization, due
Downloaded from https://academic.oup.com/jpids/article/10/5/650/6140794 by guest on 12 February 2024
to limited resources for chart review at that site, we decided a
METHODS
priori to use simple random sampling to select approximately
70% of cases meeting the inclusion criteria for review to meet
Study Location and Design the target sample size. Data were entered into a secure Research
We conducted a multisite retrospective cohort study at 5 Electronic Data Capture tool hosted at Stanford University [11].
children’s hospitals and 1 large managed care organization
from January 1, 2012, to June 30, 2017. Sites were located in Definitions
California (3), Georgia (1), Minnesota (1), and Washington (1) Definitive therapy was defined as the antibiotics received to treat
as detailed in Supplementary Table 1. The study was approved the UTI once the organism and susceptibilities were known.
by the institutional review board at each participating site. This therapy was classified as concordant (isolate susceptible)
or discordant (isolate non-susceptible, ie, intermediate or re-
Study Population sistant), consistent with prior studies [12–15]. The “limited oral
We included children ≤18 years old presenting to an acute antibiotic options” variable was defined as non-susceptibility to
care setting (emergency department, inpatient setting, or all of the following oral antibiotics to which susceptibility was
general pediatrics/urgent care clinic) with a third-generation tested: amoxicillin-clavulanate, ciprofloxacin, trimethoprim-
cephalosporin-resistant UTI. UTI was defined per AAP sulfamethoxazole, and nitrofurantoin. These antibiotics were
Guidelines as having both: (1) pyuria, defined as >5 white chosen because they are the most common oral options for third-
blood cells per high power field or any leukocyte esterase and generation cephalosporin-resistant isolates. If all options were not
(2) urine culture with ≥50 000 colony-forming units per mil- tested, the isolate was considered to have “limited oral antibiotic
liliter of growth [6]. Third-generation cephalosporin-resistant options” if it was non-susceptible to all the tested options. Because
UTI was defined as a UTI from Enterobacterales, specifically nitrofurantoin is not recommended for pyelonephritis [16], it was
Escherichia coli or Klebsiella spp., non-susceptible (ie, inter- only considered an oral option for patients ≥2 years without symp-
mediate or resistant) to ceftriaxone/cefotaxime. We studied toms concerning for pyelonephritis (defined as fever, abdominal/
third-generation cephalosporin-resistant isolates, similar to flank pain, poor oral intake, or nausea/vomiting). Genitourinary
other investigations [2, 8], because some institutions’ labora- abnormalities were defined as renal abnormalities or vesicoureteral
tories within our study did not specifically test for ESBL resist- reflux. Clinical response at the time that urine culture suscepti-
ance. Site laboratories completed urinalyses, urine dipsticks, bilities were available was assessed by physician chart review for
and urine cultures according to standard procedures, and an- patients started on discordant therapy for whom this information
tibiotic susceptibilities were determined according to Clinical was available in follow-up documentation [7]. Clinical response
and Laboratory Standards Institute (CLSI) guidelines [9]. Given was classified as “improved” (complete or partial resolution of pre-
that practitioners are more likely to react to the laboratory des- senting signs or symptoms) or “not improved” (persistence of pre-
ignation of susceptibility rather than the minimum inhibitory senting signs or symptoms).
concentration (MIC) levels for ceftriaxone/cefotaxime, we did
not collect MIC data. Urine cultures were obtained via straight Outcomes
catheterization or clean catch. If the collection method was The outcome of concordant parenteral therapy duration was cat-
not documented, subjects without documentation of a urinary egorized as: (1) long parenteral therapy, defined as ≥3 days of
catheter were included. Children were excluded if they had a concordant parenteral therapy or (2) short/no parenteral therapy,
history of urologic surgery other than circumcision, were im- defined as 0–2 days of concordant parenteral therapy and also
munocompromised (received immunosuppressants in the included treatment with only oral antibiotics or no definitive
Management and Outcomes of Resistant UTIs • jpids 2021:10 (May) • 651
treatment. For example, if a patient received 2 days of ceftriaxone age, limited oral antibiotic options, and genitourinary abnormal-
while awaiting urine culture results, followed by 2 days of ities. We conducted a sensitivity analysis including the variable
meropenem, the patient would be categorized as “short/no par- of clinical response, which was available for 48% of the cohort.
enteral therapy” because they received 2 days of concordant par- Coefficients were “marginalized” so that estimates represented
enteral therapy. A duration of ≥3 days was chosen based on prior the average effect across hospitals [21]. We compared the propor-
literature [17] and author consensus. UTI relapse was defined as tion of patients with UTI relapse using unadjusted analysis with
a third-generation cephalosporin-resistant UTI with the same or- Fisher’s exact test due to the low number of events. Data were
ganism species within 30 days of the initial UTI and urine culture analyzed using Stata version 15 (StataCorp, College Station, TX).
[17–20] and was determined by physician chart review. Half of the
study population came from institutions that had access to records RESULTS
from outside institutions. We also noted if there was a documenta-
Study Population
tion of a health care visit in their electronic medical record within
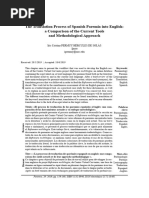
Overall, 1259 children ≤18 years of age met inclusion criteria
6 months of the initial UTI.
(Figure 1). We excluded 777 children, most commonly due to his-
Downloaded from https://academic.oup.com/jpids/article/10/5/650/6140794 by guest on 12 February 2024
tory of urologic surgery, complex chronic condition, or immuno-
Sample Size and Statistical Methods compromised status. A total of 482 children with third-generation
Based on preliminary data from the central study institution, we cephalosporin-resistant UTIs were included. Table 1 describes
estimated that 50% of the patients would be treated with long patient characteristics. The majority (80.9%) were female and the
parenteral therapy, and based on prior literature, we estimated median age was 3.3 years (interquartile range [IQR]: 0.8–8). The
that the UTI relapse rate would be 1.5% [19]. In order to have median age of males (0.3 years, IQR 0.2–1.1) was lower than that
80% power to detect an absolute risk difference of 5%, our target of females (4.4 years, IQR 1.6–8.3), P < .001. Most of the isolates
sample size was 480. We conducted multivariable mixed-effects (453/482, 94.0%) were resistant to ceftriaxone/cefotaxime, and 29
logistic regression to determine predictors of long parenteral (6.0%) had intermediate susceptibility. Antibiotic susceptibilities are
therapy with hospital site as a random effect. Covariates were presented in Supplementary Table 2. Median total duration of anti-
determined a priori based on prior literature and included sex, biotic therapy was 10 days (IQR: 9-12).
Figure 1. Study profile.
652 • jpids 2021:10 (May) • Wang et al
Table 1. Demographic, Clinical, and Laboratory Characteristics of discordant parenteral therapy (mean duration: 2 days) prior to con-
Children With Third-Generation Cephalosporin-Resistant UTIs
cordant therapy. Twenty-three (43%) were only hospitalized once
n = 482 N, %a urine cultures finalized. The long parenteral therapy group had a
Sex (n, %) higher proportion who were male, <2 months of age, had genitou-
Male 92 (19.1) rinary abnormalities, and had limited oral antibiotic options com-
Female 390 (80.9)
pared with the short/no parenteral therapy group (Table 2). Most
Age (median, IQR) 3.3 (0.8-8)
children in this group were treated with a carbapenem (Table 3).
Age category (n, %)
Less than 2 mo 28 (5.8)
Short/No Parenteral Therapy
2-23 mo 158 (32.8)
2-4 y 101 (21.0)
Overall, 428 (88.8%) children received short/no parenteral
5-17 y 195 (40.5) therapy; 6 (1.4%) received 1–2 days of concordant parenteral
Genitourinary abnormalities (n, %) 25b (5.2) therapy, 407 (95.1%) were treated with only oral antibiotics, and
Prior UTI (n, %) 106 (22.0) 15 (3.5%) did not receive definitive treatment (Table 3).
Prior third-generation cephalosporin-resistant UTI (n, %) 8 (1.7)
Downloaded from https://academic.oup.com/jpids/article/10/5/650/6140794 by guest on 12 February 2024
When urine cultures finalized, most of the children (302/428,
Setting of initial evaluation (n, %)
70.6%) received concordant antibiotics, 105 (24.5%) received
Emergency Department 268 (55.6)
General pediatrics/urgent care clinic 211 (43.8)
discordant antibiotics, and 6 (1.4%) had documentation of an
Inpatient 3 (0.6) antibiotic change with no mention of the new antibiotic name.
Ill appearance (n, %) 8 (1.7) Of those treated with discordant antibiotics, 88 were continued
Presenting symptoms on empiric discordant antibiotics (44 with clear documenta-
Abdominal and/or back pain 88 (18.3)
tion of continuation of discordant antibiotics and 44 with no
Abnormal urine odor 83 (17.2)
documentation of antibiotic change) and 17 were switched to
Dysuria 203 (42.1)
Fever 275 (57.1)
different discordant antibiotics following the return of cul-
Fussiness and/or irritability 49 (10.2) ture results. Selected comments from chart review describing
Nausea and/or vomiting 100 (20.7) reasons for continued discordant antibiotics are presented in
Poor oral intake 76 (15.8) Supplementary Table 3 and include clinical improvement, pa-
Otherc 115 (23.9)
tient/family preference, and consultant recommendations.
≥1 symptom 475 (98.5)
Sixty-nine children (16.1%) in the short/no parenteral
Urine culture collection method
Straight catheterization 171 (35.5) therapy group had limited oral antibiotic options. In this group,
Clean catch 288 (59.8) the most common definitive antibiotics were nitrofurantoin
Method not recorded 23 (4.8) (31) and cephalosporins (18); 30 of the 31 (97%) children who
Urine culture colony count (n, %) received nitrofurantoin reported symptoms concerning for py-
50 000-100 000 CFU/mL 74 (15.4)
elonephritis (eg, fever) and 12 of the 31 children (39%) were
Greater than 100 000 CFU/mL 408 (84.6)
Urine culture organism (n, %)
<2 years.
Escherichia coli 476 (98.8) Seven patients without symptoms recorded were treated
Klebsiella spp. 6 (1.2) with: long parenteral therapy (1) and short/no parenteral
Bacteremia 3d (0.6) therapy (6: concordant antibiotics [3], discordant antibiotics
Limited oral antibiotic options 100 (20.7) [1], unknown antibiotics [1], and no treatment [1]).
Abbreviations: IQR, interquartile range; UTI, urinary tract infection, CFU/mL, colony-forming units per milliliter.
a
Percentages may not add up to 100 due to rounding.
b
11/25 patients with genitourinary abnormalities had vesicoureteral reflux (6 had grade 1–3, 2 had grade 4–5,
and 3 did not have grade documented); 21/25 had renal abnormalities (eg, duplicated or dilated collecting Predictors of Long Parenteral Therapy
system, hydronephrosis, renal cysts, and pelviectasis).
In multivariable regression, predictors of long parenteral
c
The most common symptoms in the “Other” category included other genitourinary symptoms (eg, frequency/
urgency), constitutional symptoms, and GI symptoms not included in the above categories. A total of 466/482 therapy included: age <2 months (adjusted odds ratio [aOR]
(96.7%) patients had at least 1 symptom from the above categories without including the “Other” category.
d
Two patients had bacteremia with the same third-generation cephalosporin-resistant organism from their 67.3; 95% confidence interval [CI]: 16.4-275.7 compared
urine culture. One patient had 2 E. coli organisms in urine culture, 1 ceftriaxone-resistant strain, and 1 with age 5-17 years), limited oral antibiotic options (aOR 5.9;
ceftriaxone-susceptible strain and also had bacteremia with the ceftriaxone-susceptible strain.
95% CI: 2.8-12.3), and genitourinary abnormalities (aOR 5.4;
95% CI: 1.8-15.9) (Table 2). Male sex was borderline signif-
Definitive Treatment icant (aOR 2.1; 95% CI: 1.0-4.7). In a sensitivity analysis in-
Long Parenteral Therapy cluding clinical response information for 230 patients started
Fifty-four children (11.2%) received long parenteral therapy with on discordant therapy, the association between lack of im-
a median duration of 7 days (IQR: 7-10, range 3-21); 43 of the 54 provement in clinical response and long parenteral therapy
(80%) children received parenteral therapy exclusively. Thirty-one was not significant (aOR 1.7, 95% CI: 0.5-5.2; Supplementary
(57%) were hospitalized at presentation, 27 of whom received Table 4).
Management and Outcomes of Resistant UTIs • jpids 2021:10 (May) • 653
Table 2. Predictors of Long Parenteral Therapy in Children With Third-Generation Cephalosporin-Resistant UTIs
Short/no Parenteral Therapy (n = 428) Long Parenteral Therapy (n = 54)
n, (%) n, (%) Unadjusted Odds Ratios (95% CI) Adjusted Odds Ratiosa (95% CI)
Sex
Male 63 (14.7) 29 (53.7) 6.7 (3.7-12.2) 2.1 (1.0-4.7)
Female 365 (85.3) 25 (46.3) Ref. Ref.
Age category
<2 mo 7 (1.6) 21 (38.9) 114.0 (33.2-391.2) 67.3 (16.4-275.7)
2–23 mo 136 (31.8) 22 (40.7) 6.1 (2.3-16.6) 2.6 (0.9-7.5)
2–4 y 95 (22.2) 6 (11.1) 2.4 (0.7-8.1) 2.0 (0.6-6.6)
5–17 y 190 (44.4) 5 (9.3) Ref. Ref.
Limited oral antibiotic options
Yes 69 (16.1) 31 (57.4) 4.3 (2.4-7.7) 5.9 (2.8-12.3)
No 359 (83.9) 23 (42.6) Ref. Ref.
Genitourinary abnormalities
Downloaded from https://academic.oup.com/jpids/article/10/5/650/6140794 by guest on 12 February 2024
Yes 16 (3.7) 9 (16.7) 5.2 (2.2-12.3) 5.4 (1.8-15.9)
No 412 (96.3) 45 (83.3) Ref. Ref.
Abbreviation: CI, confidence interval.
a
Our single mixed-effects model included these 4 factors as fixed effects and hospital site as a random effect to adjust for clustering. Estimated coefficients from the mixed-effects models were marginalized to reflect the average
effect across hospitals. Intra-class correlation coefficient was 17% (95% CI 4%-49%), P = .002.
UTI Relapse Within the short/no parenteral therapy group, UTI relapse oc-
UTI relapse occurred in 7 of the 482 children (1.5%, 95% CI: curred in 3 of the 302 children (1.0%, 95% CI: 0.2%-2.9%) treated
0.6%-3.0%). In the long parenteral therapy group, UTI relapse with concordant therapy and 3 of the 105 children (2.9%, 95% CI:
occurred in 1 of the 54 (1.9%, 95% CI: 0.1%-9.9%) children com- 0.6%–8.1%) treated with discordant therapy. The absolute risk dif-
pared with 6 of the 428 (1.4%, 95% CI: 0.5%-3.0%) children in the ference between the discordant and concordant therapy groups
short/no parenteral therapy group, for an absolute risk difference was 1.8% (95% CI: −1.5% to 5.1%). Subgroup analyses by suscep-
of −0.4% (95% CI: −4.2% to 3.3%; Table 4). tibility to ceftriaxone are presented in Supplementary Table 5.
Table 3. Definitive Antibiotic Treatment, by Age Group, in Children With Third-Generation Cephalosporin-Resistant UTIs
All Children (n = 482) N, %a Less Than 2 months (n = 28) N, % 2-23 Months (n = 158) N, % 2-4 Years (n = 101) N, % 5-17 Years (n = 195) N, %
Long parenteral therapy (n, %) 54 (11.2)a 21 (75.0) 22 (13.9) 6 (5.9) 5 (2.6)
Beta-lactam/beta-lactamase inhibitorb 7 (1.5) 5 (17.9) 1 (0.6) 0 (0) 1 (0.5)
Carbapenemc 39 (8.1) 10 (35.7) 19 (12.0) 6 (5.9) 4 (2.1)
Cephalosporind 4 (0.8) 2 (7.1) 2 (1.3) 0 (0) 0 (0)
Gentamicine 4 (0.8) 4 (14.3) 0 (0) 0 (0) 0 (0)
Short/no parenteral therapy (n, %) 428 (88.8) 7 (25.0) 136 (86.1) 95 (94.1) 190 (97.4)
Amoxicillin-clavulanate 60 (12.4) 5 (17.9) 28 (17.7) 12 (11.9) 15 (7.7)
Cephalosporinf 85 (17.6) 0 (0) 30 (19.0) 21 (20.8) 34 (17.4)
Ciprofloxacin 30 (6.2) 0 (0) 7 (4.4) 4 (4.0) 19 (9.7)
Nitrofurantoin 89 (18.5) 2 (7.1) 20 (12.7) 23 (22.8) 44 (22.6)
Trimethoprim-sulfamethoxazole 136 (28.2) 0 (0) 40 (25.3) 30 (29.7) 66 (33.8)
Otherg 7 (1.5) 0 (0) 2 (1.3) 2 (2.0) 3 (1.5)
Unknownh 6 (1.2) 0 (0) 3 (1.9) 0 (0) 3 (1.5)
Nonei 15 (3.1) 0 (0) 6 (3.8) 3 (3.0) 6 (3.1)
Percentages may not add up to 100 due to rounding.
a
11 patients were transitioned to definitive oral therapy. Age/therapy breakdown was: age <2 months (3 children: amoxicillin-clavulanate [1] and trimethoprim-sulfamethoxazole [2]), age 2-23 months (4 children: amoxicillin-
clavulanate [2] and trimethoprim-sulfamethoxazole [2]), age 2-4 years (3 children: amoxicillin-clavulanate [2] and trimethoprim-sulfamethoxazole [1]), and age 5-17 years (1 child: trimethoprim-sulfamethoxazole).
b
Beta-lactam/beta-lactamase inhibitors included ampicillin-sulbactam (1) and piperacillin-tazobactam (6).
c
Carbapenems included ertapenem (8) and meropenem (31).
d
Parenteral cephalosporins included cefepime (2), cefoxitin (1), and ceftazidime (1).
e
One patient was treated concurrently with cefotaxime.
f
Oral cephalosporins included cephalexin (64), cefprozil (3), cefdinir (14), and cefixime (4). One patient in this group grew 2 strains of E. coli in the urine, 1 ceftriaxone-resistant strain, and 1 ceftriaxone-susceptible strain. The
patient received 3 days of ceftriaxone followed by cefixime due to bacteremia from a ceftriaxone-susceptible strain.
g
Other included: amoxicillin (2), minocycline (2), doxycycline (1), cefdinir and amoxicillin-clavulanate concurrently (1), and 1 patient who was treated with 3 days of nitrofurantoin followed by 2 days of ertapenem after which anti-
biotics were stopped.
h
These 6 patients had documentation of switching antibiotics after culture results returned with no mention of antibiotic name.
i
Five patients were started on empiric antibiotics (4 on discordant antibiotics) during the initial evaluation, which were stopped when the culture results returned since they had improved and the urine cultures were considered
either contaminant or asymptomatic bacteriuria. The remaining 10 patients were not started on antibiotics.
654 • jpids 2021:10 (May) • Wang et al
Table 4. UTI Relapse in Children With Third-Generation Cephalosporin-Resistant UTIs
(a). Percentage With UTI Relapse
# UTI Relapses/Total % With UTI Relapse (95% CI) P-value Risk Difference, % (95% CI)
All patients 7/482 1.5 (0.6-3.0)
Long parenteral therapy 1/54 1.9 (0.1-9.9) .57 −0.4 (−4.2 to 3.3)
Short/no parenteral therapy 6/428 1.5 (0.5-3.0)
(b) UTI Relapse Case Details
Case Age/Sex Definitive Therapy Genitourinary Abnormalities
1 2 mo M Meropenem Grade 1 hydronephrosis and grade 1-III VUR
2 1yF Cephalexin None
3 4yF Cephalexin None
4 5yF Cefdinir None
5 5yF Nitrofurantoin None
Downloaded from https://academic.oup.com/jpids/article/10/5/650/6140794 by guest on 12 February 2024
6 8yF Trimethoprim-sulfamethoxazole None
7 16 y F Nitrofurantoin None
The first line was made bold since it represented the numbers for the entire study population.
Abbreviations: CI, confidence interval. UTI, urinary tract infection; VUR, vesicoureteral reflux.
About three-quarters of patients (357/482, 74%) were seen Most of the studies on pediatric third-generation
at institutions with access to records from outside institutions cephalosporin-resistant UTIs describe hospitalized children
or had documentation of a healthcare visit in their EMR within with ESBL UTIs and have documented favorable outcomes on
6 months of the initial UTI. non-carbapenem parenteral therapy [22–24]. However, few
have reported outcomes for those treated with oral therapy.
Peripherally Inserted Central Catheter Complications Our study used a multisite cohort with tertiary and community
Two of the 16 patients (13% or 4% of the entire long paren- sites and found that 422 of the 482 (87.6%) patients received
teral therapy group) who underwent peripherally inserted only oral therapy. This is a higher percentage than reported by 2
central catheter (PICC) placement experienced PICC com- US-based studies, which demonstrated that 62% of 76 children
plications. One had a PICC line thrombosis and received 4 with ESBL infections (85% from urine) from a single center and
weeks of anticoagulation. One had a PICC line breakage and 57% of 210 children with ESBL infections (89% from urine)
replacement. from 4 children’s hospitals were treated as outpatients [25, 26].
This difference is likely explained by cohort selection, since our
study only included UTIs and excluded children with complex
DISCUSSION
chronic conditions. We also found that UTI relapse occurred in
In this multisite retrospective cohort study of 482 children with only 1.5% of children and the risk of UTI relapse did not differ
third-generation cephalosporin-resistant UTIs, long parenteral by parenteral therapy duration. These results suggest that the
therapy was more common in children <2 months old, those AAP UTI guidelines recommending oral antibiotics can also be
with genitourinary abnormalities, and those whose culture sus- applied to third-generation cephalosporin-resistant UTIs.
ceptibilities conferred limited oral antibiotic options. Among We found that age <2 months was the most significant
children ≥2 months old, only 8% received long parenteral factor associated with long parenteral therapy. This is similar
therapy. UTI relapse was rare and not associated with parenteral to previous studies of pediatric UTI management showing that
therapy duration. These findings suggest that when oral anti- parenteral courses ≥4 days were more common in younger in-
biotic options are available, third-generation cephalosporin- fants, though the percentage of infants <2 months old receiving
resistant UTIs can be treated effectively with oral therapy and ≥4 days of parenteral therapy has decreased from 50% in 2005
should be considered first-line definitive treatment unless to 19% in 2015 [17, 19]. The higher percentage (75%) of infants
children cannot tolerate oral medications. Unexpectedly, a <2 months receiving long parenteral therapy in our study may
substantial proportion (>20%) of our study cohort was treated be explained by limited oral antibiotic options, concerns about
definitively with discordant antibiotics, and few patients ex- side effects of certain oral antibiotics (eg, sulfonamides and
perienced UTI relapse. Therefore, this study also provides in- quinolones), and the overall vulnerability of young infants [27].
formation on current practice patterns, especially when there The association of limited oral antibiotic options with long par-
are limited oral antibiotic options, and provides groundwork enteral therapy is consistent with prior studies demonstrating
for future studies investigating the outcomes of patients treated longer lengths of stay for children with ESBL UTIs when com-
with discordant therapy. pared with children with non-ESBL UTIs [3–5].
Management and Outcomes of Resistant UTIs • jpids 2021:10 (May) • 655
Management of third-generation cephalosporin-resistant Eligibility was confirmed through chart review and we applied
UTIs can be challenging when there are limited oral options. the AAP UTI definition to decrease the risk of misclassification.
Providers should weigh potential harms of prolonged paren- There are also several limitations. First, our regression model
teral therapy and hospitalization against the risk of UTI relapse. may not have included all relevant characteristics that influenced
Unfortunately, many of these potential harms and risks have not the decision regarding the route of therapy. Clinical response in-
been well characterized in the literature, making it challenging formation was only available for about half of the cohort; however,
for providers to engage in adequate shared decision-making the results were similar in a sensitivity analysis that included this
with patients and families. In our study, nearly 30% of patients information. Second, cases of UTI relapse and changes to therapy
treated with long parenteral therapy had a PICC placed and may have been missed if a patient re-presented to a different insti-
13% experienced complications, which is within the 8%–30% tution whose medical records were not accessible. However, inves-
complication rate from larger studies [28–31]. tigators either had access to outside records or there was evidence
There were a few unexpected findings in our study that of follow-up in the same institution for 74% of patients. This sug-
may be considered when treating a resistant UTI with lim- gests that the assessment of this outcome may be more reliable
Downloaded from https://academic.oup.com/jpids/article/10/5/650/6140794 by guest on 12 February 2024
ited oral antibiotic options. First, 69 of the 100 children than studies using administrative databases with follow-up data
whose isolates conferred limited oral antibiotic options available only from the initial institution [17, 19]. Of the patients
were nonetheless treated with either discordant antibiotics classified as receiving definitive discordant therapy, about 60%
or nitrofurantoin, which is recommended only in cystitis had clear documentation of an antibiotic switch or continuation
[16] and not in children ≤24 months, but given to some pa- of discordant therapy. Third, the study may not be adequately
tients with symptoms concerning for pyelonephritis and/ powered to detect small differences in the percentage of patients
or ≤24 months of age. In these cases, providers may have with UTI relapse. Our target sample size was based on an esti-
felt that the specific presentation was not consistent with mate that 50% would receive long parenteral therapy when only
pyelonephritis or may have felt that the potential harms 11% of our sample did. However, the upper 95% CI of the risk dif-
associated with prolonged parenteral therapy outweighed ference between the long and short/no parenteral therapy groups
those of treating with an agent that was discordant or not was only 3.3%, meaning that even in a “worst-case scenario,” the
recommended. Second, regardless of the availability of oral number-needed-to-treat (approximately 30) with long parenteral
antibiotic options, 105 of the 482 (21.8%) children were antibiotics to prevent one relapse would be fairly high, especially
treated definitively with discordant antibiotics with a low when juxtaposing this number with the number-needed-to-harm
UTI relapse rate. It is possible that if a patient’s symptoms (approximately 8) for complications from a PICC line. We were
improved while on discordant therapy, providers may have also not able to account for the severity of disease or response to
continued that treatment instead of changing antibiotics (if therapy in assessing risk for relapse and were not able to conduct
a concordant oral option was available) or recommending an adjusted analysis due to the rarity of the outcome. Nevertheless,
hospitalization and prolonged parenteral therapy (if there we believe that the rarity of the outcome regardless of parenteral
were limited oral options). Comments from chart review therapy duration is in and of itself one of the main takeaways of
showed that parental preference and specialist recom- the study. Fourth, although we incorporated pyuria into our def-
mendations may have also influenced this decision. Several inition of UTI, some patients may have had asymptomatic bac-
studies of children with ESBL UTIs have demonstrated in- teriuria. However, only a small number of patients did not have
itial clinical and microbiologic improvement while on dis- symptoms documented and most of them were treated, sug-
cordant therapy [22, 23, 32–34], and we previously reported gesting clinical suspicion for UTI. It is possible that symptoms
that the majority of patients in this study started on dis- were present but not recorded or abstracted from the chart. Fifth,
cordant antibiotics had improved by the time urine cultures since this was a retrospective study, we were unable to determine if
finalized [7]. One possible explanation for this favorable re- documented relapses were caused by a genetically identical strain
sponse is that in vitro susceptibility may not always reflect as the index infection. Finally, the results cannot be generalized to
in vivo response, since some antibiotics may achieve high patients not included in the study population, most notably those
urinary concentrations [35]. Further studies are needed to with urologic surgery, immunocompromised status, and complex
evaluate the effectiveness of continued discordant therapy chronic conditions.
in children with resistant UTIs who are improving and have
limited oral antibiotic treatment options.
CONCLUSIONS
This study has several strengths. To our knowledge, this is the
first multisite US-based study with data from tertiary children’s In a large US-based cohort of children with third-generation
hospitals and community settings to examine the outcomes of cephalosporin-resistant UTIs, we found that long parenteral
children with third-generation cephalosporin-resistant UTIs. therapy was more likely in infants <2 months of age, those with
656 • jpids 2021:10 (May) • Wang et al
genitourinary abnormalities and limited oral antibiotic op- Form for Disclosure of Potential Conflicts of Interest. Conflicts that the edi-
tors consider relevant to the content of the manuscript have been disclosed.
tions, and uncommon in children ≥2 months old. UTI relapse
was rare and not associated with parenteral therapy duration.
References
These results suggest that third-generation cephalosporin-
1. Montini G, Tullus K, Hewitt I. Febrile urinary tract infections in children. N Engl
resistant UTIs can be treated effectively with oral antibiotics J Med 2011; 365:239–50.
when oral options are available. Furthermore, UTI relapse 2. Logan LK, Braykov NP, Weinstein RA, Laxminarayan R. Extended-spectrum
beta-lactamase-producing and third-generation cephalosporin-resistant
was also uncommon among children treated definitively with Enterobacteriaceae in children: trends in the United States, 1999–2011. Pediatr
discordant antibiotics. When there are limited oral antibiotic Infect Dis J. 2014; 3(4): 320–8.
3. Flokas ME, Detsis M, Alevizakos M, Mylonakis E. Prevalence of ESBL-producing
options for third-generation cephalosporin-resistant UTIs, Enterobacteriaceae in paediatric urinary tract infections: a systematic review and
providers should weigh the potential harms of hospitalization meta-analysis. J Infect 2016; 73:547–57.
4. Dayan N, Dabbah H, Weissman I, et al. Urinary tract infections caused
and prolonged parenteral therapy against the risk of treatment by community-acquired extended-spectrum β-lactamase-producing and
failure when recommending a definitive course of therapy. nonproducing bacteria: a comparative study. J Pediatr 2013; 163:1417–21.
5. Amin O, Prestel C, Gonzalez MD, et al. Urinary tract infections with extended-
While treating definitively with discordant therapy may be
spectrum-β-lactamase-producing bacteria: case-control study. Pediatr Infect Dis
Downloaded from https://academic.oup.com/jpids/article/10/5/650/6140794 by guest on 12 February 2024
an option, further investigations evaluating this approach are J 2020; 39:211–6.
needed. 6. Roberts KB. Urinary tract infection: clinical practice guideline for the diagnosis
and management of the initial UTI in febrile infants and children 2 to 24 months.
Pediatrics 2011; 128(3): 595–610.
Supplementary Data 7. Wang ME, Lee V, Greenhow TL, et al. Clinical response to discordant
therapy in third-generation cephalosporin-resistant UTIs. Pediatrics 2020;
Supplementary materials are available at Journal of the Pediatric Infectious 145(2):e20191608.
Diseases Society online (http://jpids.oxfordjournals.org). 8. Bidell MR, Palchak M, Mohr J, Lodise TP. Fluoroquinolone and third-generation-
cephalosporin resistance among hospitalized patients with urinary tract in-
Notes fections due to Escherichia coli: do rates vary by hospital characteristics and
geographic region? Antimicrob Agents Chemother 2016; 60:3170–3.
In Memoriam. The authors wish to dedicate this paper to the memory 9. CLSI. Performance Standards for Antimicrobial Susceptibility Testing. 27th ed. CLSI
of Dr Michael Bendel-Stenzel, a coauthor who died tragically in an au- Supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute; 2017.
tomobile accident on September 25, 2020. He was 55 years old. Michael 10. Feudtner C, Feinstein JA, Zhong W, et al. Pediatric complex chronic conditions
was remarkable and yet unassuming in many ways. He was a graduate of classification system version 2: updated for ICD-10 and complex medical tech-
Gustavus Adolphus College, studying athletic training and music, followed nology dependence and transplantation. BMC Pediatr 2014; 14:199.
by medical school at the University of Minnesota where he was inducted 11. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)–a
into the prestigious Alpha Omega Alpha honor society. He completed metadata-driven methodology and workflow process for providing translational
research informatics support. J Biomed Inform 2009; 42:377–81.
residency and fellowship at the University of Minnesota, specializing in
12. Jerardi KE, Auger KA, Shah SS, et al. Discordant antibiotic therapy and length
Pediatric Nephrology. He joined Children’s Minnesota in 2008 as one of the of stay in children hospitalized for urinary tract infection. J Hosp Med 2012;
first pediatric hospitalists and has since shared his love of bow ties, extensive 7:622–7.
knowledge, and kindness with all those around him. He served as the Lead 13. Hyle EP, Lipworth AD, Zaoutis TE, et al. Impact of inadequate initial antimicro-
for Clinical Outcomes and has completed numerous quality improvement bial therapy on mortality in infections due to extended-spectrum beta-lactamase-
projects locally and nationally with the American Academy of Pediatrics. producing Enterobacteriaceae: variability by site of infection. Arch Intern Med
He was inordinately generous with his time, often helping anyone around 2005; 165:1375–80.
him with tasks large and small. Michael’s greatest passions were his love for 14. Greenhouse I, Babushkin F, Finn T, et al. Long-term outcomes of inappro-
his family, devotion to patients, music, Cheerios, golf, and travel. He and his priate antibiotic therapy for upper urinary tract infections caused by extended-
spectrum beta-lactamase-producing Enterobacteriaceae: a retrospective cohort
wife Ellen were devoted philanthropists supporting many local charitable
study. Diagn Microbiol Infect Dis 2017; 89:222–9.
and arts institutions. He has made innumerable contributions to the health 15. Lee SS, Kim Y, Chung DR. Impact of discordant empirical therapy on outcome of
of children through his research, knowledge-sharing, and joyful care of hos- community-acquired bacteremic acute pyelonephritis. J Infect 2011; 62:159–64.
pitalized children. He will be missed dearly, but his tremendous legacy and 16. Huttner A, Verhaegh EM, Harbarth S, et al. Nitrofurantoin revisited: a system-
impact will endure. atic review and meta-analysis of controlled trials. J Antimicrob Chemother 2015;
Acknowledgments. The authors would like to thank Gomathi Krishnan, 70:2456–64.
PhD, for her valuable assistance with data extraction. 17. Brady PW, Conway PH, Goudie A. Length of intravenous antibiotic therapy
Authors’ Contributions. M. E. W. designed the study, collected local and treatment failure in infants with urinary tract infections. Pediatrics 2010;
data, performed the data analyses, interpreted the data, drafted the ini- 126:196–203.
18. Desai S, Aronson PL, Shabanova V, et al. Parenteral antibiotic therapy dur-
tial manuscript, and reviewed and revised the manuscript critically for
ation in young infants with bacteremic urinary tract infections. Pediatrics 2019;
important intellectual content. T. L. G., V. L., J. B., M. B.-S., N. H., C. E.
144:e20183844.
M., E. E. K., W. S., D. P., and S. T. P. collected local data, interpreted the 19. Lewis-de Los Angeles WW, Thurm C, Hersh AL, et al. Trends in intravenous
data, and reviewed and revised the manuscript critically for important antibiotic duration for urinary tract infections in young infants. Pediatrics 2017;
intellectual content. N. S. contributed to the design of the study, collected 140:e20171021.
local data, interpreted the data, and reviewed and revised the manuscript 20. Schroeder AR, Shen MW, Biondi EA, et al. Bacteraemic urinary tract infection:
critically for important intellectual content. A. R. S. designed the study, management and outcomes in young infants. Arch Dis Child 2016; 101:125–30.
collected local data, interpreted the data, and reviewed and revised the 21. Hedeker D, du Toit SHC, Demirtas H, Gibbons RD. A note on marginalization of
manuscript critically for important intellectual content. All authors ap- regression parameters from mixed models of binary outcomes. Biometrics 2018;
74:354–61.
proved the final manuscript as submitted and agree to be accountable for
22. Madhi F, Jung C, Timsit S, et al.; Urinary-tract Infection due to Extended-
all aspects of the work.
Spectrum Beta-lactamase-producing Enterobacteriaceae in Children Group.
Financial support. No external funding for this manuscript. Febrile urinary-tract infection due to extended-spectrum beta-lactamase-
Potential conflicts of interest. The authors have no conflicts of interest producing Enterobacteriaceae in children: a French prospective multicenter
relevant to this article to disclose. The author has submitted the ICMJE study. PLoS One 2018; 13:e0190910.
Management and Outcomes of Resistant UTIs • jpids 2021:10 (May) • 657
23. Katsuta T, Shoji K, Watanabe Y, Saitoh A. Treatment of pyelonephritis caused 29. Jumani K, Advani S, Reich NG, et al. Risk factors for peripherally inserted central
by extended-spectrum β-lactamase-producing Enterobacteriaceae in children. venous catheter complications in children. JAMA Pediatr 2013; 167:429–35.
Pediatr Infect Dis J 2013; 32:417–9. 30. Keren R, Shah SS, Srivastava R, et al.; Pediatric Research in Inpatient Settings Network.
24. Abe Y, Inan-Erdogan I, Fukuchi K, et al. Efficacy of non-carbapenem antibiotics for Comparative effectiveness of intravenous vs oral antibiotics for postdischarge treat-
pediatric patients with first febrile urinary tract infection due to extended-spectrum ment of acute osteomyelitis in children. JAMA Pediatr 2015; 169:120–8.
beta-lactamase-producing Escherichia coli. J Infect Chemother 2017; 23:517–22. 31. Barrier A, Williams DJ, Connelly M, Creech CB. Frequency of peripherally in-
25. Strysko JP, Mony V, Cleveland J, et al. International travel is a risk factor for serted central catheter complications in children. Pediatr Infect Dis J 2012;
extended-spectrum β-lactamase-producing Enterobacteriaceae acquisition in 31:519–21.
children: a case-case-control study in an urban U.S. hospital. Travel Med Infect 32. Tratselas A, Iosifidis E, Ioannidou M, et al. Outcome of urinary tract infections
Dis 2016; 14:568–71. caused by extended spectrum β-lactamase-producing Enterobacteriaceae in chil-
26. Zerr DM, Miles-Jay A, Kronman MP, et al. Previous antibiotic exposure increases dren. Pediatr Infect Dis J 2011; 30:707–10.
risk of infection with extended-spectrum-β-Lactamase- and AmpC-producing 33. Uyar Aksu N, Ekinci Z, Dundar D, Baydemir C. Childhood urinary tract infec-
Escherichia coli and Klebsiella pneumoniae in pediatric patients. Antimicrob tion caused by extended-spectrum beta-lactamase-producing bacteria: risk fac-
Agents Chemother 2016; 60:4237–43. tors and empiric therapy. Pediatr. Int. 2017; 59(2): 176–80.
27. Kaguelidou F, Turner MA, Choonara I, Jacqz-Aigrain E. Ciprofloxacin use in neo- 34. Hyun HS, Kim JH, Cho MH, et al. Low relapse rate of urinary tract infections
nates: a systematic review of the literature. Pediatr Infect Dis J 2011; 30:e29–37. from extended-spectrum beta-lactamase-producing bacteria in young children.
28. Kovacich A, Tamma PD, Advani S, et al. Peripherally inserted central venous Pediatr Nephrol 2019; 34:2399–407.
catheter complications in children receiving outpatient parenteral antibiotic 35. Turnidge J, Paterson DL. Setting and revising antibacterial susceptibility break-
therapy (OPAT). Infect Control Hosp Epidemiol 2016; 37:420–4. points. Clin Microbiol Rev 2007; 20:391–408, table of contents.
Downloaded from https://academic.oup.com/jpids/article/10/5/650/6140794 by guest on 12 February 2024
658 • jpids 2021:10 (May) • Wang et al
You might also like
- Choros No 1 by Heitor Villa-Lobos PDFDocument6 pagesChoros No 1 by Heitor Villa-Lobos PDFJuan Manuel Navarro Ameller100% (1)
- Organic Chemistry ProjectDocument11 pagesOrganic Chemistry Projectapi-463768793No ratings yet
- Piaa 055Document7 pagesPiaa 055m6ztfk4nsvNo ratings yet
- Jurnal 1Document7 pagesJurnal 1Deski MadeNo ratings yet
- ciad385Document8 pagesciad385Bella saphiraNo ratings yet
- Mi Tiku 2018Document10 pagesMi Tiku 2018irania lubisNo ratings yet
- Impact of Antibiotic Treatment Duration On Community-Acquired Pneumonia in Children - A Systematic ReviewDocument9 pagesImpact of Antibiotic Treatment Duration On Community-Acquired Pneumonia in Children - A Systematic ReviewWelisson BarbosaNo ratings yet
- Antibiotic Choice and Clinical Outcomes in Ambulatory Children With Community-Acquired PneumoniaDocument19 pagesAntibiotic Choice and Clinical Outcomes in Ambulatory Children With Community-Acquired PneumoniaRisa LestariNo ratings yet
- Pneumonia Comparative Effectiveness of Empiric Antibiotics For Community-AcquiredDocument9 pagesPneumonia Comparative Effectiveness of Empiric Antibiotics For Community-AcquiredSulis Na EndutzNo ratings yet
- Pediatrics 2014 Queen E23 9Document10 pagesPediatrics 2014 Queen E23 9Desrainy InhardiniNo ratings yet
- Jiad 252Document11 pagesJiad 252Dyah Wahyu Oktania SariNo ratings yet
- Pneumonia in Infants and ChildrenDocument52 pagesPneumonia in Infants and ChildrenMikeyNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofStella NoviaNo ratings yet
- Vol. 3 No. 02 (2024) 102-117Document16 pagesVol. 3 No. 02 (2024) 102-117muradchy321No ratings yet
- Cir 531Document52 pagesCir 531Mario CornejoNo ratings yet
- Antibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenDocument5 pagesAntibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenLavfy NjlaaNo ratings yet
- Cir 531Document52 pagesCir 531Nubia PuNo ratings yet
- Nac Idsa PDFDocument52 pagesNac Idsa PDFYULIETH ANDREA SAAVEDRA COGOLLONo ratings yet
- Recomendation Treatment PneumoniaDocument52 pagesRecomendation Treatment PneumoniaJanuwar LukitaNo ratings yet
- Endocarditis: Un Estudio de Cohorte Multicéntrico, RetrospectivoDocument8 pagesEndocarditis: Un Estudio de Cohorte Multicéntrico, RetrospectivoMelendi NavarroNo ratings yet
- Burden of Severe Rotavirus Diarrhea in Indonesia: SupplementarticleDocument7 pagesBurden of Severe Rotavirus Diarrhea in Indonesia: SupplementarticleDyah Ayu KusumawarddhaniNo ratings yet
- Efficacy and Safety of Fluconazole Prophylaxis in Extremely Low Birth Weight Infants: Multicenter Pre-Post Cohort StudyDocument10 pagesEfficacy and Safety of Fluconazole Prophylaxis in Extremely Low Birth Weight Infants: Multicenter Pre-Post Cohort StudyAnry UmarNo ratings yet
- Lactobacillus Rhamnosus GG Versus Placebo For Acute Gastroenteritis in ChildrenDocument21 pagesLactobacillus Rhamnosus GG Versus Placebo For Acute Gastroenteritis in ChildrenMarsella Epifania SuwignyoNo ratings yet
- 0mpZwP-12887 2024 Article 4639Document8 pages0mpZwP-12887 2024 Article 4639MMNo ratings yet
- Diarrea en QuimioterapiaDocument6 pagesDiarrea en QuimioterapiaPaola DiazNo ratings yet
- A Study of Prescription Pattern of Antibiotics in Pediatric In-Patients of Mc-Gann Teaching Hospital Shivamogga Institute of Medical Sciences (SIMS), Shivamogga, Karnataka.Document5 pagesA Study of Prescription Pattern of Antibiotics in Pediatric In-Patients of Mc-Gann Teaching Hospital Shivamogga Institute of Medical Sciences (SIMS), Shivamogga, Karnataka.International Organization of Scientific Research (IOSR)No ratings yet
- CAP in Children - IDSADocument52 pagesCAP in Children - IDSAlala liliNo ratings yet
- Peds Pneumnoaie GuidlinesDocument56 pagesPeds Pneumnoaie GuidlinesDorji InternationalNo ratings yet
- 2011 Ispad NeumoníaDocument14 pages2011 Ispad NeumoníaAaron Nureña JaraNo ratings yet
- National Ambulatory Antibiotic Prescribing Patterns For Pediatric Urinary Tract Infection, 1998 - 2007Document9 pagesNational Ambulatory Antibiotic Prescribing Patterns For Pediatric Urinary Tract Infection, 1998 - 2007Rodolfo Rodriguez CamposNo ratings yet
- Nur Aisiyah Widjaja_Folia 2023Document8 pagesNur Aisiyah Widjaja_Folia 2023Baarizah FebrianaNo ratings yet
- Risk Factors For and Outcomes of Multidrug-Resistant Escherichia Coli Infections in ChildrenDocument17 pagesRisk Factors For and Outcomes of Multidrug-Resistant Escherichia Coli Infections in ChildrenLihaniUltifaNo ratings yet
- Vital Sign Predictors of Severe InfluenzaDocument11 pagesVital Sign Predictors of Severe InfluenzaDesiska PriciliaNo ratings yet
- 10 11648 J Ajim 20150303 13Document8 pages10 11648 J Ajim 20150303 13Fate ChanNo ratings yet
- journal.pone.0274423Document13 pagesjournal.pone.0274423seilla manja rahmadinaNo ratings yet
- 1 SM PDFDocument7 pages1 SM PDFCintia FloresNo ratings yet
- Resistensi AntibiotikDocument21 pagesResistensi AntibiotikMaruliTuaNo ratings yet
- With Pneumonia Narrow Vs Broad-Spectrum Antimicrobial Therapy For Children HospitalizedDocument10 pagesWith Pneumonia Narrow Vs Broad-Spectrum Antimicrobial Therapy For Children HospitalizedanettepardedeNo ratings yet
- 40121_2017_Article_152Document13 pages40121_2017_Article_152Fragen IntermedicaNo ratings yet
- E20161692 FullDocument11 pagesE20161692 FullWiti Triple'sNo ratings yet
- medip,+IJCP-1957+O+DDocument6 pagesmedip,+IJCP-1957+O+Djobekara9No ratings yet
- Ciac 948Document9 pagesCiac 948Mestika KuineNo ratings yet
- Cost HMPVDocument9 pagesCost HMPVjan yerenaNo ratings yet
- Probiotics and The Immunological Response To Infant Vaccinations - A Prospective, Placebo Controlled Pilot StufyDocument6 pagesProbiotics and The Immunological Response To Infant Vaccinations - A Prospective, Placebo Controlled Pilot StufyDhayu Mart Hindrasyah PandiaNo ratings yet
- Moderately Affected Children Tonsillectomy and Adenotonsillectomy For Recurrent Throat Infection inDocument11 pagesModerately Affected Children Tonsillectomy and Adenotonsillectomy For Recurrent Throat Infection inReza Rizky Al RasyidNo ratings yet
- With Intravenous Antibiotics Urinary Tract Infections in 1-To 3-Month-Old Infants: Ambulatory TreatmentDocument9 pagesWith Intravenous Antibiotics Urinary Tract Infections in 1-To 3-Month-Old Infants: Ambulatory Treatmentsri_jva8No ratings yet
- Effect of Amoxicillin Dose and Treatment Duration On The Need For Antibiotic Re-Treatment in Children With Community-Acquired PneumoniaDocument140 pagesEffect of Amoxicillin Dose and Treatment Duration On The Need For Antibiotic Re-Treatment in Children With Community-Acquired Pneumoniajennylau0809No ratings yet
- Moderate-to-Severe Diarrhea and Stunting Among ChildrenDocument8 pagesModerate-to-Severe Diarrhea and Stunting Among ChildrenFebry AnaNo ratings yet
- Esbl Sepsis India2011Document8 pagesEsbl Sepsis India2011Jonathan WelchNo ratings yet
- Article 1Document6 pagesArticle 1AMILA SYAZLINANo ratings yet
- Diagnosis and Management of Acute Sinusitis by PediatriciansDocument8 pagesDiagnosis and Management of Acute Sinusitis by Pediatriciansminerva_stanciuNo ratings yet
- Bloodstream Infections in Hospitalized Children: Epidemiology and Antimicrobial SusceptibilitiesDocument4 pagesBloodstream Infections in Hospitalized Children: Epidemiology and Antimicrobial SusceptibilitiesrasioputraNo ratings yet
- (R) Varicella 2Document4 pages(R) Varicella 2IdzhamReezaNo ratings yet
- UntitledDocument10 pagesUntitledWahidNo ratings yet
- Time To ATBsDocument8 pagesTime To ATBsXIMENAGILDANo ratings yet
- Prevalence and Risk Factors of Helicobacter Pylori Infection in Asymptomatic Chinese Children: A Prospective, Cross-Sectional, Population-Based StudyDocument8 pagesPrevalence and Risk Factors of Helicobacter Pylori Infection in Asymptomatic Chinese Children: A Prospective, Cross-Sectional, Population-Based StudyyundaNo ratings yet
- 10 16899-jcm 1475605-3893872Document8 pages10 16899-jcm 1475605-3893872cemresukizilcinarNo ratings yet
- 2277-Article Text-7155-4-10-20200122Document15 pages2277-Article Text-7155-4-10-20200122fadil ahmadiNo ratings yet
- Moderately Affected Children Tonsillectomy and Adenotonsillectomy For Recurrent Throat Infection inDocument11 pagesModerately Affected Children Tonsillectomy and Adenotonsillectomy For Recurrent Throat Infection inKarlina MiaowNo ratings yet
- Ajp - 180544 EosDocument9 pagesAjp - 180544 EosJeeNo ratings yet
- Ciz 1197Document8 pagesCiz 1197Lindia PrabhaswariNo ratings yet
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- The Translation Process of Spanish Paremia Into EnglishDocument10 pagesThe Translation Process of Spanish Paremia Into EnglishAnka GłowiakNo ratings yet
- Play and Learn Character Awards 2024Document4 pagesPlay and Learn Character Awards 2024Anj TaalaNo ratings yet
- The Economics of Social Problems - (Pages 1 To 25)Document25 pagesThe Economics of Social Problems - (Pages 1 To 25)21100724dNo ratings yet
- Tamako Sia by Blacklily PDFDocument286 pagesTamako Sia by Blacklily PDFMaria Shin Yen MendozaNo ratings yet
- 5 One Dimensional Flow of Water Through SoilsDocument28 pages5 One Dimensional Flow of Water Through SoilsJenina LogmaoNo ratings yet
- Case Analysis MetrobankDocument4 pagesCase Analysis MetrobankMei Misaki20% (5)
- Documentation Guidelines in Software EngineeringDocument10 pagesDocumentation Guidelines in Software EngineeringvenumulkallapalliNo ratings yet
- The Impact of Cell Phone, Laptop Computer, and Microwave Oven Usage On Male FertilityDocument17 pagesThe Impact of Cell Phone, Laptop Computer, and Microwave Oven Usage On Male FertilitymaxsmaxNo ratings yet
- Lavanya ResumeDocument2 pagesLavanya ResumestoberryNo ratings yet
- Davidson SongofSongs AUSSDocument19 pagesDavidson SongofSongs AUSSBart Foster100% (2)
- Test 1 - AnswersDocument0 pagesTest 1 - AnswersOnlyMyWayNo ratings yet
- Jets80 Stainless-Steel-Self-Priming-Jet-Pump - 48342Document3 pagesJets80 Stainless-Steel-Self-Priming-Jet-Pump - 48342chaghoufNo ratings yet
- Heat TransferDocument42 pagesHeat TransferKundan KumarNo ratings yet
- Pollution Water AgricultureDocument20 pagesPollution Water AgricultureSikder Mohammod Ekteder NabilNo ratings yet
- Environmental Engineering (BFC 32403) Individual Assignment (5%)Document6 pagesEnvironmental Engineering (BFC 32403) Individual Assignment (5%)Muhammad HasanuddinNo ratings yet
- CHP Eight StatisticDocument17 pagesCHP Eight StatisticFaris SyahmiNo ratings yet
- CTD and eCTDDocument5 pagesCTD and eCTDSri harsha reddyNo ratings yet
- Everret SteamshipDocument42 pagesEverret SteamshipJoshua OuanoNo ratings yet
- Check List - How Assignment A Will Be AssessedDocument3 pagesCheck List - How Assignment A Will Be AssessedKatrina WongNo ratings yet
- Business Budget: FundingDocument4 pagesBusiness Budget: FundingMae Anne Yabut Roque-CunananNo ratings yet
- Embrace The Danish Way of LivingDocument4 pagesEmbrace The Danish Way of Livingmaximiliano lencinaNo ratings yet
- LS Central/LS Nav Cumulative Updates 2007 - 2023, Overview: Industry Feature (With Link To LS Retail Help)Document1,440 pagesLS Central/LS Nav Cumulative Updates 2007 - 2023, Overview: Industry Feature (With Link To LS Retail Help)Sandeep ShettyNo ratings yet
- Junglee Child - Visual Pitch DeckDocument15 pagesJunglee Child - Visual Pitch Decksarah stuntNo ratings yet
- Module I - Lessons 1 and 2Document4 pagesModule I - Lessons 1 and 2potsuNo ratings yet
- Gov. Larry Hogan's 'Stay at Home' Order 3.30.20Document8 pagesGov. Larry Hogan's 'Stay at Home' Order 3.30.20WJZ89% (9)
- Antonio Lauro - Yacambu (Guitar Pro)Document4 pagesAntonio Lauro - Yacambu (Guitar Pro)Jefte Israel MontillaNo ratings yet
- Running Bill Formate For DevkamiyatiDocument15 pagesRunning Bill Formate For DevkamiyatiOm Chauhan100% (1)
- Commercial Paper: (Industrial Paper, Finance Paper, Corporate Paper)Document27 pagesCommercial Paper: (Industrial Paper, Finance Paper, Corporate Paper)shivakumar N100% (1)