Basic Pharmacology
Basic Pharmacology
Download as pdf or txt
You might also like
- Brenner and Steven's Pharmacology 5th EditionDocument4 pagesBrenner and Steven's Pharmacology 5th Editionarief satya0% (4)
- Rau's Chapter 2 WBDocument4 pagesRau's Chapter 2 WBMichael DunlapNo ratings yet
- BPS2110 Midterm 1 AnswersDocument5 pagesBPS2110 Midterm 1 AnswersMaya AkkawiNo ratings yet
- Pharmacology UNIT 1 - Lesson 1Document29 pagesPharmacology UNIT 1 - Lesson 1Bea Bianca Cruz100% (1)
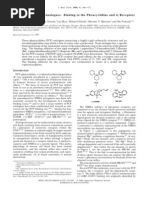
- J. Med. Chem. 1998, 41, 468-477Document10 pagesJ. Med. Chem. 1998, 41, 468-477SlapdragonxNo ratings yet
- HyndaviDocument42 pagesHyndaviHyndavi ManyamNo ratings yet
- Pharma LectureDocument68 pagesPharma LectureMax LocoNo ratings yet
- Pharmaceutics pt2Document22 pagesPharmaceutics pt2bismaqayyum69No ratings yet
- Pharmaceutics 2Document16 pagesPharmaceutics 2bismaqayyum69No ratings yet
- Report On Coursera 1-LalithaVedulaDocument12 pagesReport On Coursera 1-LalithaVedulaLalitha SahithiNo ratings yet
- PHC 501 Drug Design, Discovery and DevelopmentDocument16 pagesPHC 501 Drug Design, Discovery and DevelopmentSasaniNo ratings yet
- Basic Principles of PharmacologyDocument75 pagesBasic Principles of PharmacologyJessica Febrina Wuisan100% (2)
- Nurs 316 Notes Nurs 316 2Document241 pagesNurs 316 Notes Nurs 316 2sukhman1996No ratings yet
- Introduction To PharmacologyDocument6 pagesIntroduction To PharmacologyMark Russel Sean LealNo ratings yet
- PHARMACOLOGY Handout 8 18 21Document3 pagesPHARMACOLOGY Handout 8 18 21Sheila May Teope SantosNo ratings yet
- Pharma NotesDocument4 pagesPharma Notesmoncalshareen3No ratings yet
- Lec 2Document25 pagesLec 2rafid mNo ratings yet
- Notes FormatDocument4 pagesNotes FormatSamuel IdoNo ratings yet
- Unit 1 NotesDocument21 pagesUnit 1 Notesbdelvalle3No ratings yet
- Introduction To Pharmacology DefinitionDocument4 pagesIntroduction To Pharmacology DefinitionMaicha PestañoNo ratings yet
- Nwe Drug Development and FDADocument125 pagesNwe Drug Development and FDAUjwala Chowdary50% (2)
- Pharmacology: Introduction To Nursing PharmacologyDocument10 pagesPharmacology: Introduction To Nursing PharmacologyMarianne Joyce ManzoNo ratings yet
- Introduction Into Pharmacology 2029Document8 pagesIntroduction Into Pharmacology 2029mohammaddammagNo ratings yet
- Practicals (Pharmaceutical Technology)Document24 pagesPracticals (Pharmaceutical Technology)Kustian Kohat100% (1)
- Drug Development & RegulationDocument63 pagesDrug Development & Regulationlucymueni700No ratings yet
- Introduction To PharmacologyDocument52 pagesIntroduction To PharmacologyNicole SorongonNo ratings yet
- Basic Principles of Pharmacology: Prof. Suheil Zmeili Faculty of Medicine Department of Pharmacology University of JordanDocument79 pagesBasic Principles of Pharmacology: Prof. Suheil Zmeili Faculty of Medicine Department of Pharmacology University of JordanChengDNo ratings yet
- Non Clinical StudiesDocument7 pagesNon Clinical Studiesvipinkv99No ratings yet
- 2) Chapter 1 clinical trail Module 1aDocument4 pages2) Chapter 1 clinical trail Module 1ayebadaaNo ratings yet
- Chapter 1: Introduction To Nursing PharmacologyDocument9 pagesChapter 1: Introduction To Nursing PharmacologyAlyssaGrandeMontimorNo ratings yet
- AghhjnvfhjDocument15 pagesAghhjnvfhjAllyssa Mae CambaNo ratings yet
- Pharmacology: Bachelor of Science in Nursing Level 2 Second SemesterDocument41 pagesPharmacology: Bachelor of Science in Nursing Level 2 Second SemesterAmiel Francisco ReyesNo ratings yet
- IND Ashwani GoyalDocument16 pagesIND Ashwani Goyalashpharma007No ratings yet
- Drug Ders 1Document45 pagesDrug Ders 1nadyamelekavciNo ratings yet
- Pharm NCLEXDocument76 pagesPharm NCLEXSara PirmanNo ratings yet
- General Introduction of Pharmacology and Experimental PharmacologyDocument2 pagesGeneral Introduction of Pharmacology and Experimental PharmacologyswetaNo ratings yet
- Approval & Development: DrugsDocument11 pagesApproval & Development: DrugsOmar SalehNo ratings yet
- Banned Drug 1Document6 pagesBanned Drug 1Nasrin Akther ShopnaNo ratings yet
- Medication AdministrationDocument298 pagesMedication AdministrationOfficially Random100% (1)
- Viewer in PharmaDocument8 pagesViewer in Pharmacloeyeol1485No ratings yet
- Comprehensive Pharmacy Review 7Document61 pagesComprehensive Pharmacy Review 7Imee TingzonNo ratings yet
- General PharmacologyDocument8 pagesGeneral PharmacologysekarenthangavelNo ratings yet
- Notes in PharmacologyDocument95 pagesNotes in PharmacologyMylz MendozaNo ratings yet
- Experimental PharmacologyDocument14 pagesExperimental PharmacologyAdarsh Mauli PawarNo ratings yet
- Biotechnology and New Drug Development: Duhok Polytechnic University Duhok Technical Institute Pharmacy DepartmentDocument19 pagesBiotechnology and New Drug Development: Duhok Polytechnic University Duhok Technical Institute Pharmacy DepartmentTurkiya Shammo AliNo ratings yet
- Questions On Drug Discovery and DevelopmentDocument6 pagesQuestions On Drug Discovery and Developmentvalerybikobo588100% (1)
- 2011 02 28 Development Classification of MedicineDocument71 pages2011 02 28 Development Classification of MedicineDiana D'souzaNo ratings yet
- Drug Development CPRDocument8 pagesDrug Development CPRmuhammadyawarsaeed4No ratings yet
- Drug DevelopmentDocument96 pagesDrug DevelopmentSheena GagarinNo ratings yet
- Individual Assignment 1Document6 pagesIndividual Assignment 1Che InopiaNo ratings yet
- Regulatory Bodies in USA, Europe, India, China and AustraliaDocument9 pagesRegulatory Bodies in USA, Europe, India, China and AustraliapriyadarshNo ratings yet
- 02 - The Drug Development Process - Step 1 - Discovery and DevelopmentDocument2 pages02 - The Drug Development Process - Step 1 - Discovery and DevelopmentArunendu MajiNo ratings yet
- 1.0 Pharmaceutical Chemistry - 091533Document13 pages1.0 Pharmaceutical Chemistry - 091533owegibrian479No ratings yet
- Drug Testing, Manufacture and ProvisionDocument11 pagesDrug Testing, Manufacture and Provisionniyathi tips2007No ratings yet
- Module 1 Introduction to DrugsDocument5 pagesModule 1 Introduction to DrugsNicole Cassey GutierrezNo ratings yet
- Safety Testing of PharmaceuticalsDocument39 pagesSafety Testing of PharmaceuticalsSaikumar RoithNo ratings yet
- Notes in PharmacologyDocument96 pagesNotes in Pharmacologydmd_2dd50% (2)
- Final Project LevofloxacinDocument102 pagesFinal Project LevofloxacinJalwaz TihamiNo ratings yet
- Drugs and Pharmaceutical Technology Question BankDocument7 pagesDrugs and Pharmaceutical Technology Question BankVanitha ENo ratings yet
- Safety Data GenerationDocument17 pagesSafety Data GenerationAbhinav BhathejaNo ratings yet
- 3 - 5 The Drug Development ProcessDocument10 pages3 - 5 The Drug Development Processaghanafissa5No ratings yet
- ANS Adrenergic System (Medlive by DR Priyanka)Document464 pagesANS Adrenergic System (Medlive by DR Priyanka)bushrawrites10101No ratings yet
- Analgesic and Acetylcholinesterase Inhibition Potential of PolyphenolsDocument10 pagesAnalgesic and Acetylcholinesterase Inhibition Potential of Polyphenolsvlad_văluNo ratings yet
- 715 PrometricDocument61 pages715 PrometricNosheen HaqNo ratings yet
- Mechanisms of Drug Interactions: Pharmacodynamics and PharmacokineticsDocument4 pagesMechanisms of Drug Interactions: Pharmacodynamics and Pharmacokineticsgowepa9266No ratings yet
- Chapter 22 Sedative HypnoticsDocument7 pagesChapter 22 Sedative HypnoticsChristine Annmarie TapawanNo ratings yet
- Pharmacology QuestionsDocument6 pagesPharmacology Questionsliaqat ahmed100% (1)
- Pharmacology Notes CH 1 IntroductionDocument4 pagesPharmacology Notes CH 1 Introductionridley45No ratings yet
- Addendum StemBook2018 202003Document5 pagesAddendum StemBook2018 202003Yachao LiuNo ratings yet
- 41-46 TEXTBOOK The Asam Essentials of Addiction MedicineDocument7 pages41-46 TEXTBOOK The Asam Essentials of Addiction MedicineErlanNo ratings yet
- Drug-Receptor Interactions and PharmacodynamicsDocument4 pagesDrug-Receptor Interactions and Pharmacodynamicshussam mazinNo ratings yet
- Autacoid - SerotoninDocument4 pagesAutacoid - SerotoninJohn Ellard M. SaturnoNo ratings yet
- Pharmacology 1 - Case Study 1Document2 pagesPharmacology 1 - Case Study 1BaldogNo ratings yet
- Adrenergic Antagonist (2013)Document23 pagesAdrenergic Antagonist (2013)Akmal SafwanNo ratings yet
- Betahistine Dihydrochloride in The Treatment of Peripheral Vestibular VertigoDocument6 pagesBetahistine Dihydrochloride in The Treatment of Peripheral Vestibular VertigoRidho HidayatullohNo ratings yet
- PainDocument124 pagesPainWinno Pradana UtomoNo ratings yet
- Revised Pharmacophore Model For 5 HT2A Receptor Antagonists Derived From The Atypical Antipsychotic Agent RisperidoneDocument14 pagesRevised Pharmacophore Model For 5 HT2A Receptor Antagonists Derived From The Atypical Antipsychotic Agent RisperidoneLUCAS OYANEDERNo ratings yet
- 2.BMD Study Guide Final 6.4.2023Document42 pages2.BMD Study Guide Final 6.4.2023Phyo Wai KyawNo ratings yet
- Prefix Suffix MnemonicsDocument4 pagesPrefix Suffix MnemonicsAubrey BellezaNo ratings yet
- Module 1 Active Learning GuideDocument4 pagesModule 1 Active Learning GuideKamil MominNo ratings yet
- Prefix Suffix MnemonicsDocument5 pagesPrefix Suffix MnemonicsPj MontecilloNo ratings yet
- Pharmacology Review - A Comprehensive Reference Guide For Medical, Nursing, and Paramedic StudentsDocument276 pagesPharmacology Review - A Comprehensive Reference Guide For Medical, Nursing, and Paramedic Studentsfjletona100% (2)
- General Pharmacology) 343 (Document28 pagesGeneral Pharmacology) 343 (ALNAKI100% (1)
- Pharmacology MCQ-1Document102 pagesPharmacology MCQ-1asadullah.amanNo ratings yet
- Adrenergic and Antiadrenergic DrugsDocument31 pagesAdrenergic and Antiadrenergic DrugsMaaz AliNo ratings yet
- Precise PharmacologyDocument323 pagesPrecise Pharmacologykiggundu alvinNo ratings yet
- Pharmacology AtfDocument77 pagesPharmacology AtfGheorghe AdrianNo ratings yet