Incisional Hernia Repair: Laparoscopy Versus Open Surgery - A Prospective Study
Incisional Hernia Repair: Laparoscopy Versus Open Surgery - A Prospective Study
Research Article ISSN 2689-1093
Research Article Surgical Research
Incisional Hernia Repair: Laparoscopy versus Open Surgery - A
Prospective Study
LAMARA Abdelhak1*, BENYARABAH Saliha1, GUADDA Mounir1, BELHATEM Mohamed Salah1, NINI
Badereddine1, BOUKHENE Mohamed1, MEDJAHDI Sid Ahmed1, NIBOUCHA Mohamed Lamine2
and Dr. Meriem Rayen LAMARA3
*
Correspondence:
General Surgery, Regional Military Hospital of Constantine /5RM Algeria.
1
Professor Abdelhak LAMARA, Head of General Surgery,
2
Department of Medical Activity, Regional Military Hospital of Constantine Regional Military Hospital, Abdelaali BENBAATOUCHE -
/5RM Algeria. Constantine / 5 RM, BP: 61 C, 25001 - Constantine – Algeria,
Tel: (213) 697289929.
Peterborough, UK.
3
Received: 28 Jul 2023; Accepted: 30 Aug 2023; Published: 05 Sep 2023
Citation: LAMARA A, BENYARBAH S, GUADDA M, et al. Incisional Hernia Repair: Laparoscopy versus Open Surgery - A Prospective
Study. Surg Res. 2023; 5(2): 1-6.
ABSTRACT
Objective: To assess the feasibility of laparoscopic incisional hernia repairs and to examine possible differences in
operative time, morbidity, recurrence rates and length of hospital stay compared to repairs performed by open surgery.
Patients: Between January 2016 and June 2019, sixty patients who underwent parietal repair were enrolled in this
study. Patients were divided into two non-randomised groups. Data were collected prospectively and recorded in a
database. The statistical analysis was performed using SPSS24 biomedical statistics software and Microsoft Excel.
The statistical analysis was performed using the chi-two test, with calculation of the P value (Pearson test).
Results: Thirty patients who underwent parietal repair by laparoscopic preperitoneal prosthesis placement (first
group), and 30 patients who underwent open repair (2nd group). The two groups were comparable in terms of
gender distribution and body mass index. No significant differences were observed in age and comorbidities between
the two groups.
In the first group, implantation of an intraperitoneal bifacial prosthesis was possible in 93.3% of patients. In the
second group, the prosthesis was placed retromuscularly in 56.6% of patients and perifascial in 41% of patients.
The conversion rate to open surgery was 6.6%. The average operating time was (81mn vs 92min). The complication
rate was (26.6% vs 43.3%). The average length of hospital stay was 2 days 5.6 days. The recurrence rate at 3 years
is (3.3% 6.6%; P< 0.05).
Conclusion: The results of this study suggest that parietal repair by laparoscopic intraperitoneal prosthesis
placement has some advantages over open surgery.
Keywords incisional hernias, thanks to the use of adapted prosthetic material
Incisional hernia, Laparoscopic repair, Open surgeon repair, that allows the implantation sites on the abdominal wall to be
Morbidity, Hospital stay, Recurrence. enlarged according to their physicochemical characteristics [1-
3]. Over time, several surgical techniques have been validated
Introduction depending on the nature and type of prosthesis used.
Significant progress has been made in the treatment of ventral
Surg Res, 2023 Volume 5 | Issue 2 | 1 of 6
Tension-free parietoplasty with prosthetic reinforcement is An abdominal ultrasound was performed in all patients, mainly
considered the technique of choice for the repair of incisional and to look for associated intraperitoneal pathology. In addition,
primary ventral hernias by open surgery. In contrast, the repair of a CT scan of the abdominal wall was performed to clarify the
ventral incisional hernias by laparoscopy consists of parietoplasty exact dimensions of the hernia, the nature of the hernial contents,
by intraperitoneal composite prosthesis, aimed at filling the parietal measure the diastasis of the rectus muscles of the abdomen and
defect by overlapping the edges of the defect by 3-5 cm, without assess the thickness of the adipose tissue.
deterioration of the wall. This technique is currently considered
a quality reference because of its feasibility, cost-effectiveness, Risk factors and comorbidities were considered and assessed.
reduced morbidity and improved quality of life [1,2].
Patients who are candidates for laparoscopic surgery were
informed during the preoperative consultation about the
The main challenge in repairing ventral hernias is to reduce the
rate of recurrence, and the effectiveness of each technique is advantages and disadvantages of this technique, as well as the
evaluated according to the incidence of recurrence. Based on possibility of conversion to open surgery if necessary. Patients'
recent data from the literature and in order to contribute to the consent was obtained regarding the surgical technique chosen and the
development of new minimally invasive techniques in our possibility of discharge from hospital on the first post-operative day in
hospital, we chose the technique of parietal repair of incisional the absence of complications. The intraperitoneal site has been used in
hernias by laparoscopy using the intraperitoneal site. To reinforce laparoscopic repairs, while the retromuscular site has been preferred
the value of this prospective study, we compared this technique to in the majority of cases during open surgery repairs.
other open surgery parietal repair procedures performed during the
same study period. Results
In this study, a total of sixty patients were operated on for a ventral
The main objective of this prospective comparative study is to incisional hernia, divided into two groups of thirty patients each.
evaluate the feasibility of this technique on a scarred abdomen The first group was operated on by laparoscopic surgery and the
in patients who have undergone several surgical procedures, second group by open surgery. The mean age of patients was 52.53
except for patients with a recurrent hernia already treated with a
years, with an age range of 27 to 82 years. Women accounted for
prosthesis. In addition, we sought to analyze the rate and causes of
78% of cases, a sex ratio of 3.61. The majority of females were
conversion, the rate of recurrence, and to evaluate the advantages
housewives (68.3%) of cases. Not all patients included in the study
of this technique compared to other procedures.
were morbidly obese, but all had at least one predisposing factor for
The use of minimally invasive incisional hernia repair using the hernia. In the majority of cases, eventration was secondary to anterior
intraperitoneal site with adapted prostheses aims to reduce the rate laparotomy (83.3%), followed by hernia on a trocar orifice (10%).
of recurrence on the one hand and to improve quality of life and The most common type of hernia was type M2, accounting for 60% of
reduce economic costs on the other hand. Since our department is cases and evenly distributed between the two groups (Table1).
a training center, we tried, during the study period, to allow other
surgeons and residents to learn this technique. Table 1: Features of patients and hernia.
Features of patients and Laparoscopy Open Surgery
P
It should be noted that other surgical techniques are still used. hernia N (%) N (%)
Overall, the aim of this prospective study is to evaluate the M 07 (23) 06 (20) 0.07
Gender
feasibility of repairing ventral eventrations using intraperitoneal F 23 (76.6) 24 (80)
prostheses by laparoscopy, and to compare the results obtained with 27-42 11 (36.6) 03 (10)
those of repairs performed by open surgery. Endpoints assessed in Age (Years) 43-65 12 (40) 13 (43.3) 0.1
this study include duration of surgery, rate of conversion to open 66-82 07 (23.3) 14 (46.6)
surgery, incidence of complications, length of hospital stay, and ≤ 25 9 (30) 8 (26,6)
recurrence rate. kg/m2 ≥ 25 ≤ 30 14 (46,6) 17 (56,6)
≥30 ≤35 7 (23,3) 5 (16,6)
Patients and Method Respiratory disorder 21 (70) 14 (46)
This is a prospective, non-randomized controlled study of sixty M1 - - 06 20 P 0.3
patients who underwent surgery for ventral incisional hernia. M2 18 60 18 60
Thirty patients underwent laparoscopic surgery and thirty patients M3 03 5 03 10
underwent open surgery from January 2016 to June 2019. Topography
M4 - - 02 6.6
Inclusion criteria in this study included all ventral incisional L1 01 3.3 01 3.3
hernias of the anterolateral wall, recurrent abdominal eventrations L3 02 6.6 -
not treated with prosthesis, incisional hernias on trocar orifice, and OR 06 20 -
eventrations with a diameter greater than 6 cm. IBM SPSS24 and < à 05 cm 14 (46.6) 09 (30) NS
Microsoft Excel biomedical software were used, as well as the 05 à 10 cm 13 (43.3) 19 (63.3) p : 0,03
Defect size
chi-two test with p-value calculation (Pearson test), to analyze the Double orifice 01 (3.3) 01 (3.3) NS
study results. Multiorifice 02 (6.6) NS
Surg Res, 2023 Volume 5 | Issue 2 | 2 of 6
The size of the hernial collar ranged from 5 to 10 cm, with 23 level analgesics. Only two patients in the first group developed
patients having a collar less than 5 cm, and 32 patients having wall sepsis, while six patients in the second group developed
a collar between 10 and 15 cm. Two patients had double-orifice wall sepsis. The average length of hospital stay was 2 days for
hernias and two other patients had multi-orificial hernias (Table1). laparoscopic surgery and 5 to 6 days for open surgery. The overall
recurrence rate was 5%, with one recurrence in the first group and
The creation of pneumoperitoneum was achieved by an opening two recurrences in the second group (Table 2).
in the abdominal wall (open laparoscopy) in 27 patients and by a
Veress needle in three patients. In the laparoscopic repair group, Table 2: Complications and recurrences.
hernia repair was performed by three trocars in 96.6% of cases, Laparoscopy Open Total
Complications Khi-deux
with dissection and hernial sac release required in 16.6% of N (%) N (%) N (%)
patients. Persistent pain" 2 (7) 3 (10) 5 (8.6) NS
Seroma 2 (7) 0 (0) 2 (3.4) NS
Adesiolysis was difficult in two patients operated by laparoscopy and Parietal hematoma 1 (3.5) 2 (6.6) 3 (5) NS
Parietal infection" 1 (3.5) 6 (20) 7 (12) <0.05
seven patients operated by open surgery. In two cases, conversion
Rate of
to open surgery was required, representing a conversion rate of complications
6 (21.4) 11 (36.6) 17 (29.3) NS
6.6%. The size of the parietal defect, measured during surgery, Recurrence
was identical to radiological data in 17 patients, underestimated
in 42 patients and overestimated in a single patient. The average Discussion
duration of surgery was 81.51 minutes for laparoscopic repairs and Incisional hernia is a major complication of any abdominal surgery.
92.06 minutes for open surgery repairs. Its incidence varies between 13% and 20% after a laparotomy and
is common in the first five years postoperatively. About 50% of
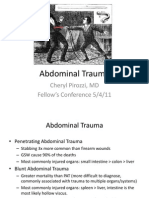
In the first group, repair of incisional ventral hernias was performed cases occur within the first two years [2-6].
using intraperitoneal prostheses in 28 patients (46.66%), (Figures
1 a, b, and c). However, in two patients in this group, laparoscopic The predominance of women is found in most studies published in
repair was impossible due to dissecting difficulties in one patient the literature [5,6]. Obesity is one of the main causes of postoperative
and an iatrogenic intestinal wound in the other. Both cases required complications affecting cardiorespiratory and metabolic function
conversion to retromuscular repair in one of the patients, while the and can be life-threatening with an insignificant mortality rate. The
other patient did not receive immediate repair. laparoscopic approach offers the possibility of incisional hernia
repair in patients with morbid obesity with a significant reduction
in postoperative complications especially those related to parietal
infection [7,8]. Previous research has demonstrated the feasibility
and safety of laparoscopic repair of VIH in obese patients and
those with morbid obesity (BMI ≥ 35kg/m2) [9,10].
In some situations where difficulties prevent the continuation
of laparoscopic surgery, it is sometimes necessary to resort
to perform open surgery. In our study, we encountered two
situations where we were no longer able to continue the procedure
a b c laparoscopically, resulting in conversion to open surgery. The
Figure 1: Laparoscopic hernia repair. conversion rate generally varies between 2.1% and 3.2% [5,11].
a. M3 hernia Dissection difficulties, intestinal wounds and intraoperative
b. Adhesiolysis and hernia content reduction hemorrhages are the most common causes of conversions to open
c. Fixation of the prosthesis surgery. The incidence of iatrogenic intestinal wounds that require
conversion to open surgery typically ranges from 1% to 3%. In
In the second group, implantation of the prosthesis was performed contrast, intraoperative bleeding as a cause of conversion is not
using an extraperitoneal technique in 29 patients. In one patient often reported by most practitioners and researchers. In some
in this group, parietal repair was delayed due to an iatrogenic series, conversions relating to the occurrence of intraoperative
intestinal wound. complications are clearly indicated and range from 1% to 5%
[5,10-13].
In laparoscopic repairs, the size of the prosthesis used ranged from
15 to 20 cm. In the open repair group, 30 cm prostheses were used In our study, the conversion rate is 6.6%. This is due to an iatrogenic
in 11 patients. An intestinal wound occurred during adhesiolysis wound of the small intestine in one case, where parietal repair was
in one patient in each group, which resulted in the postponement performed by simple plasty and final repair was postponed. In
of incisional hernia repair. Two patients operated by laparoscopy another case, dissection proved impossible due to enteroparietal
experienced significant postoperative pain (3.5%), requiring first- adhesions, and as a precaution, we preferred to complete the
Surg Res, 2023 Volume 5 | Issue 2 | 3 of 6
procedure with open surgery. The conversion rate in some series Postoperative comfort is one of the major advantages of laparoscopic
remains low, ranging from 0.5 to 1% [14-16]. parietal repairs of incisional hernias. Patients who have undergone
this surgical approach usually express great satisfaction and
The duration of surgery for laparoscopic hernia repairs is usually recommend this method to their relatives. In addition, the early
shorter than that of open surgery. However, the duration of the resumption of social activities is also an objective of this technique.
operation can vary depending on several factors, including the The main goal of laparoscopic parietal repairs of incisional hernias
experience of the surgeon. In our study, the average duration of the is to reduce the rate of postoperative recurrence. This rate can vary
intervention was 81.51 minutes, with a range of 40 to 185 minutes. from one series to another in a large series of 7516 laparoscopic
For open surgery, the operating time ranged from 40 to 150 ventral incisional hernia repairs. Moreau [23], finds a recurrence
minutes, with an average duration of 92.02 minutes. These results rate of 4.6%, comparable to the results obtained by Heniford [17].
are consistent with those reported in the literature [10,13,14,17]. The recurrence rate is lower in Cardin's study [5], but this rate is
It's worth noting that the reported duration of HIV surgery in a 13.5% in the Levard study [12].
large series of 1029 laparoscopic procedures was 40 minutes.
However, this result might not have taken into consideration the The difference in the prevalence of complications after laparoscopic
learning curve of the techniques [13]. In another series of 819 repair of incisional ventral hernias depending on the modalities
laparoscopic cures reported by Herniford, the average duration of fixation of the prosthesis is not very significant. Postoperative
was 120 minutes [17]. complications are related to adhesions. The detection of these
adhesions radiologically is possible thanks to high-resolution
Postoperative complications of primary or incisional ventral ultrasound [6,24-27]. The effectiveness of laparoscopic repair
hernia repairs by laparoscopic surgery mainly include seromas, of incisional ventral hernias in large hernias in obese patients is
persistent postoperative pain at 3 months, surgical site infection, possible and even with encouraging results [6,28].
and hemorrhage. It is important to note that the prevalence of these
complications may vary depending on the surgeon's experience In a comparative meta-analysis of retrospective studies based on
[18]. The American Hernia Society confirms the decrease in the several outcomes, Rudmik et al. [25] have proven the optimal
rate of postoperative complications after laparoscopic incisional approach for laparoscopic repair of incisional ventral hernias. The
hernia repair compared to open surgery repairs (05% to 30% repair of incisional ventral hernias has become a gold standard.
versus 27% to 34%), the same findings are made by Mc Greey et The effectiveness and safety of this technique is based on its
al., in a prospective study published in 2003 [19]. Similarly, in our
advantages over open repair, regardless of the site of implantation,
study, the postoperative complication rate of laparoscopic parietal
in terms of the incidence of early complications, and especially
repairs is significantly lower than the complication rate of open
the rate of recurrence. Other factors were also analyzed, mainly
repairs (P<0.005).
operating time, hospital stay, and resumption of postoperative
activities [3,20,29,30].
The duration of postoperative hospitalization is one of the
advantages of laparoscopic surgery. In our study, the average
hospital stay in the laparoscopic repair group was 2 days, but the The laparoscopic approach in the repair of incisional ventral
stay in patients operated on by the open route was longer (5.63 hernias is considered a valid and safe technique. Some consider
days). This benefit of laparoscopic incision hernia surgery is it the best technique. Although, the financial impact related to the
reported by the majority of authors [15, 20-22]. This route first prosthetic equipment used is high, the good results expected, in
makes possible the application of the ambulatory concept in the terms of length of stay, the resumption of activities, and especially
treatment of incisional hernias, the duration of hospitalization in a low rate of postoperative complications and recurrence, has put
fifteen patients of our study did not exceed 24 hours (Single Night). the balance of the financial cost in its favor compared to open
surgery techniques [29]. All these benefits have led surgeons to
The reoperation rate for postoperative surgical complications varies use this route, and thus the increased incidence of laparoscopic
from 0 to 3.5% depending on the series [6,15,17,23]. The main ventral incision hernia repairs over the years compared to open
causes of revision surgery are mainly postoperative hemorrhages, surgery [29,30].
unknown intestinal wounds, and intestinal obstructions. Persistent
pain resistant to medical treatment was also reported as a cause of Conclusion
early postoperative recovery, this pain is usually related to stapling Laparoscopic repair of ventral incisional hernias offers many
the prosthesis [6,24]. benefits. This technique is feasible and easy to perform by
respecting the protocols and tips specific to hernia repair. It is
The operative mortality of laparoscopic incisional ventral hernia particularly suitable for obese patients. In addition, it allows a
repairs is low, in addition to medical complications, such as reduction in the duration of hospitalization, with the possibility of a
pulmonary embolism, unknown intraoperative intestinal wounds discharge the day after the intervention for the majority of patients
discovered at the stages of advanced peritonitis are the most - "single night". The reduction in the incidence of postoperative
common mortality factors [14,17,23]. complications, especially hernia recurrences, as well as the early
Surg Res, 2023 Volume 5 | Issue 2 | 4 of 6
resumption of usual social activities, contribute to the overall 14. Alfredo Moreno-Egea, José Antonio Castillo Bustos, Enrique
satisfaction of operated patients. Girela, et al, Long-term results of laparoscopic repair of
incisional hernias using an intraperitoneal composite mesh.
References Surgical Endoscopy. 2010; 24: 359-365.
1. Lechaux JP, Lechaux D, Chevrel JP. Traitement des 15. DeMaria EJ, Moss JM, Sugerman HJ. Laparoscopic
éventrations de la paroi abdominale. EMC-Chirurgie. 2004; intraperitoneal polytetrafluoroethylene (PTFE) prosthetic
1: 601-619. patch repair of ventral hernia. Surgical Endoscopy. 2000; 14:
2. Höer J, Lawong G, Klinge U, et al. Factors influencing the 326-329.
development of incisional hernia. A retrospective study of 16. Holzman MD, Purut CM, Reintgen K, et al. Laparoscopic
2,983 laparotomy patients over a period of 10 years. Der ventral and incisional hernioplasty. Surgical Endoscopy.
Chirurg. 2002; 73: 474-480. 1997; 11: 32-35.
3. Riet M van't, Vrijland WW, Lange JF, et al. Mesh repair of 17. Todd Heniford B, Adrian Park, Bruce J Ramshaw, et al.
incisional hernia: comparison of laparoscopic and open repair. Laparoscopic repair of ventral hernias: nine years’ experience
The European journal of surgery. 2002; 168: 684-689. with 850 consecutive hernias. Annals of Surgery. 2003; 238:
391-400.
4. Park A, Birch DW, Lovrics P. Laparoscopic and open
incisional hernia repair: a comparison study. Surgery. 1998; 18. LeBlanc KA, Whitaker JM, Bellanger DE, et al. Laparoscopic
124: 816-822. incisional and ventral hernioplasty: lessons learned from 200
patients. Hernia. 2003; 7: 118-124.
5. Cardin JL, Johanet H. Incidents et accidents peropératoires:
suites de 4000 laparoscopies. La série du Club Cœlio. Journal 19. McGreevy JM, Goodney PP, Birkmeyer CM, et al. A
de Chirurgie Viscérale. 2011; 148: 336-344. prospective study comparing the complication rates between
laparoscopic and open ventral hernia repairs. Surgical
6. Wassenaar E, Schoenmaeckers E, Raymakers J, et al. Mesh- Endoscopy and Other Interventional Techniques. 2003; 17:
fixation method and pain and quality of life after laparoscopic 1778-1780.
ventral or incisional hernia repair: a randomized trial of three
20. Byron E Wright, Brian D Niskanen, Debra J Peterson, et al.
fixation techniques. Surgical Endoscopy. 2010; 24: 1296-
Laparoscopic ventral hernia repair: Are there comparative
1302.
advantages over traditional methods of repair? /Discussion.
7. Giovanni Carlo Ferrari, Angelo Miranda, Stefano Di Lernia, The American surgeon. 2002; 68: 291-295.
et al. Laparoscopic repair of incisional hernia: outcomes of
21. Olmi S, Scaini A,Cesana GC, et al. Laparoscopic versus open
100 consecutive cases comprising 25 wall defects larger than
incisional hernia repair: an open randomized controlled study.
15 cm. Surgical Endoscopy. 2008; 22: 1173-1179.
Surgical Endoscopy. 2007; 21: 555-559.
8. Raquel Maia, Hrishikesh Salgaonkar, Davide Lomanto, et al.
22. Paolo Baccari, Jacopo Nifosi, Luca Ghirardelli, et al.
Ventral hernia and obesity: is there a consensus. Ann Laparosc Laparoscopic incisional and ventral hernia repair without
Endosc Surg. 2019; 4: 17. sutures: a single-center experience with 200 cases. Journal of
9. Ioannis Raftopoulos, Daniel Vanuno, Jubin Khorsand, et al. Laparoendoscopic & Advanced Surgical Techniques. 2009;
Outcome of laparoscopic ventral hernia repair in correlation 19: 175-179.
with obesity, type of hernia, and hernia size. Journal of 23. Moreau PE, N. Helmy N, Vons C. Traitement des éventrations
Laparoendoscopic & Advanced Surgical Techniques. 2002; par laparoscopie. Quel bilan en 2012? Journal de Chirurgie
12: 425-429. Viscérale. 2012; 149: S42-S50.
10. Yuri W Novitsky, William S Cobb, Kent W Kercher, et al. 24. Mussack T, Fischer T, Ladurner R, et al. Cine magnetic
Laparoscopic ventral hernia repair in obese patients: a new resonance imaging vs high-resolution ultrasonography for
standard of care. Archives of Surgery. 2006; 141: 57-61. detection of adhesions after laparoscopic and open incisional
11. Sharma A, Mehrotra M, Khullar R, et al. Limited-conversion hernia repair: a matched pair pilot analysis. Surgical Endoscopy
technique: a safe and viable alternative to conversion in and Other Interventional Techniques. 2005; 19: 1538-1543.
laparoscopic ventral/incisional hernia repair. Hernia. 2008; 25. Rudmik LR, Schieman C, Dixon E, et al. Laparoscopic
12: 367-371. incisional hernia repair: a review of the literature. Hernia.
12. Levard H, Curt F, Perniceni T, et al. Laparoscopic incisional 2006; 10: 110-119.
hernia repair: prospective non randomized trial in 51 cases. 26. Wassenaar EB, Raymakers JTFJ, Rakic S. Impact of the mesh
Annales de chirurgie. 2005; 131: 244-249. fixation technique on operation time in laparoscopic repair of
13. Stefano Olmi, Matteo Uccelli, Giovanni Carlo Cesana, et al. ventral hernias. Hernia. 2008; 12: 23-25.
Laparoscopic abdominal wall hernia repair. JSLS: Journal of 27. Carbajo MC, Martp del Olmo JC, Blanco JI, et al. Laparoscopic
the Society of Laparoscopic & Robotic Surgeons. 2020; 24: approach to incisional hernia. Surgical Endoscopy and Other
e2020.00007. Interventional Techniques. 2003; 17: 118-122.
Surg Res, 2023 Volume 5 | Issue 2 | 5 of 6
28. Mario Junior Nardi, Paolo Millo, Riccardo Brachet Contul, et laparoscopic surgery for incisional hernia repair. BMC
al. Laparoscopic incisional and ventral hernia repair (LIVHR) surgery. 2013; 13: 1-6.
with PARIETEX™ Composite mesh. Minimally Invasive 30. Radha Govind Khandelwal, Monika Bibyan, Prasanna K
Therapy & Allied Technologies. 2012; 21: 173-180. Reddy. Transfascial suture hernia: a rare form of recurrence
29. Marijn Poelman, Jan Apers, Han van den Brand, et al. The after laparoscopic ventral hernia repair. Journal of
INCH-Trial: a multicentre randomized controlled trial Laparoendoscopic & Advanced Surgical Techniques. 2010;
comparing the efficacy of conventional open surgery and 20: 753-755.
© 2023 LAMARA A, et al. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License
Surg Res, 2023 Volume 5 | Issue 2 | 6 of 6
You might also like
- Step 2 CK NBME Form 4 Edited AnswersDocument10 pagesStep 2 CK NBME Form 4 Edited AnswersBilal Nasir100% (3)
- PNLE Maternal and Child Health Nursing Exam - Reviewer PDFDocument29 pagesPNLE Maternal and Child Health Nursing Exam - Reviewer PDFSheng DekitNo ratings yet
- Abdominal TraumaDocument47 pagesAbdominal TraumaWidya Rahayu100% (1)
- Atlas of Operative Procedures in Surgical OncologyFrom EverandAtlas of Operative Procedures in Surgical OncologyNo ratings yet
- Robotic Hernia Surgery: A Comprehensive Illustrated GuideFrom EverandRobotic Hernia Surgery: A Comprehensive Illustrated GuideOmar Yusef KudsiNo ratings yet
- Maintenance Therapy For Teeth and ImplantsDocument10 pagesMaintenance Therapy For Teeth and Implantspatricia sotoNo ratings yet
- Campos, Mesh, 2021Document8 pagesCampos, Mesh, 2021Tarek AbouzeidNo ratings yet
- Laparoscopic Ventral Hernia Repair With Tacker Only Mesh Fixation: Single Centre ExperienceDocument5 pagesLaparoscopic Ventral Hernia Repair With Tacker Only Mesh Fixation: Single Centre ExperienceMudassar SattarNo ratings yet
- Laparoscopic Vs Open Ventral Hernia RepairDocument4 pagesLaparoscopic Vs Open Ventral Hernia RepairLouis FortunatoNo ratings yet
- Open Retromuscular Sublay Mesh Repair Versus Laparoscopic Intraperitoneal Onlay Mesh Repair For Ventral Hernias A Randomized Control TrialDocument7 pagesOpen Retromuscular Sublay Mesh Repair Versus Laparoscopic Intraperitoneal Onlay Mesh Repair For Ventral Hernias A Randomized Control TrialAthenaeum Scientific PublishersNo ratings yet
- Armijo 2020Document7 pagesArmijo 2020Yeudiel SuroNo ratings yet
- Abu Saleh, Routine Mesh, 2018Document10 pagesAbu Saleh, Routine Mesh, 2018Tarek AbouzeidNo ratings yet
- tmp9F73 TMPDocument5 pagestmp9F73 TMPFrontiersNo ratings yet
- Umesh Singh. TLTK-47Document5 pagesUmesh Singh. TLTK-47HẢI HOÀNG THANHNo ratings yet
- cambareri2016-2Document7 pagescambareri2016-2mukhlis akmalNo ratings yet
- Reoperative Antireflux Surgery For Failed Fundoplication: An Analysis of Outcomes in 275 PatientsDocument8 pagesReoperative Antireflux Surgery For Failed Fundoplication: An Analysis of Outcomes in 275 PatientsDiego Andres VasquezNo ratings yet
- Laparaskopi PeritonitisDocument5 pagesLaparaskopi PeritonitisPutri RiszaNo ratings yet
- Guillot Re Au 2009Document6 pagesGuillot Re Au 2009nimaelhajjiNo ratings yet
- IRJP MAY 23 GEN+SURG5 Intermittent+and+Continuous+Aberdeen+Sutures+for+Closure+of+Document4 pagesIRJP MAY 23 GEN+SURG5 Intermittent+and+Continuous+Aberdeen+Sutures+for+Closure+of+k.smilyopenventioNo ratings yet
- f194 DikonversiDocument5 pagesf194 DikonversiFarizka Dwinda HNo ratings yet
- Utd 04524 Clinical - Article KunduzDocument5 pagesUtd 04524 Clinical - Article Kunduzzenatihanen123No ratings yet
- Ismaeil 2018Document15 pagesIsmaeil 2018Javier ZaquinaulaNo ratings yet
- Comparison Between On Lay and in Lay Mesh in Repair of Incisional HerniaDocument15 pagesComparison Between On Lay and in Lay Mesh in Repair of Incisional HerniaAshok kumarNo ratings yet
- 1 s2.0 S2049080118300967 MainDocument4 pages1 s2.0 S2049080118300967 MainNikhilesh GowdaNo ratings yet
- Irjp June 2Document6 pagesIrjp June 2k.smilyopenventioNo ratings yet
- 1503-Article Text-5213-2-10-20240122Document4 pages1503-Article Text-5213-2-10-20240122dr syed qasim ali jafriNo ratings yet
- Gastrectomía LaparoscópicaDocument7 pagesGastrectomía LaparoscópicaGreyza VelazcoNo ratings yet
- FLOT 3 QuimioterapiaDocument8 pagesFLOT 3 Quimioterapiaerica corral corralNo ratings yet
- World Journal of Emergency Surgery: Emergency Laparoscopy - Current Best PracticeDocument9 pagesWorld Journal of Emergency Surgery: Emergency Laparoscopy - Current Best PracticeHendra JojoNo ratings yet
- Omentum OverlayDocument10 pagesOmentum OverlayAlin MihetiuNo ratings yet
- Versus: Laparoscopic Open Appendectomy: Which Way To Go?Document6 pagesVersus: Laparoscopic Open Appendectomy: Which Way To Go?Claudiu Ungureanu ClauNo ratings yet
- Cirugía Española 2023 Power 4Document13 pagesCirugía Española 2023 Power 485v9jr5vdzNo ratings yet
- Journal AppDocument3 pagesJournal AppliqqamuqitaNo ratings yet
- Small Intestine Anastomosis by Full Thickness, Single Layer and Interrupted Suture Technique: Results of A Comparative StudyDocument4 pagesSmall Intestine Anastomosis by Full Thickness, Single Layer and Interrupted Suture Technique: Results of A Comparative StudyS3V4_9154No ratings yet
- Effect of Self Expandable Metal Stent 2022Document10 pagesEffect of Self Expandable Metal Stent 2022javardiNo ratings yet
- L Ess-49140-Research - Article-GokcalDocument8 pagesL Ess-49140-Research - Article-Gokcaljulianaperalta97No ratings yet
- Results of Laparoscopic Colorectal Surgery From a Nat 2014 Asian Journal ofDocument7 pagesResults of Laparoscopic Colorectal Surgery From a Nat 2014 Asian Journal ofellaha.aslamy1995No ratings yet
- Perbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterDocument7 pagesPerbedaan Penanganan Antara Laparoskopi Vs Open Repair Pada Perforasi GasterAfiani JannahNo ratings yet
- Comapartion SutureDocument7 pagesComapartion SutureGuillermo Nieves PeredoNo ratings yet
- Laparoscopic Peptic Ulcer Perforation Closure: The Preferred ChoiceDocument5 pagesLaparoscopic Peptic Ulcer Perforation Closure: The Preferred ChoiceHanny FadhilaNo ratings yet
- Evaluating The Impact of Technique and Mesh Type in Complicated Ventral Hernia Repair: A Prospective Randomized Multicenter Controlled TrialDocument14 pagesEvaluating The Impact of Technique and Mesh Type in Complicated Ventral Hernia Repair: A Prospective Randomized Multicenter Controlled TrialDaniela Cortez RojasNo ratings yet
- Laparoscopy A Realistic Diagnostic and Theraputic Modality For Abdominal Trauma Our Experience of Laparoscopy in Abdominal Trauma A Prospective StudyDocument6 pagesLaparoscopy A Realistic Diagnostic and Theraputic Modality For Abdominal Trauma Our Experience of Laparoscopy in Abdominal Trauma A Prospective StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Component SeparationDocument23 pagesComponent Separationismu100% (2)
- Outcomes of Laparoscopic-Assisted, Open Umbilical Hernia RepairDocument4 pagesOutcomes of Laparoscopic-Assisted, Open Umbilical Hernia RepairDerian TanwijayaNo ratings yet
- Research ArticleDocument6 pagesResearch ArticleHendry SusantoNo ratings yet
- Aijcr 2009 02 005Document6 pagesAijcr 2009 02 005Apps OmNo ratings yet
- Laparoscopia Versus Laparotomía para El Manejo Del Traumatismo Abdominal - Revisión Sistemática y MetanálisisDocument13 pagesLaparoscopia Versus Laparotomía para El Manejo Del Traumatismo Abdominal - Revisión Sistemática y MetanálisisLuis Miguel Díaz VegaNo ratings yet
- Lap Vs Robotic Inguinal Hernia SnalysisDocument10 pagesLap Vs Robotic Inguinal Hernia SnalysisAshwin JainNo ratings yet
- Diagnostic and Therapeutic Approach To Abdominal Masses in A Country With Limited ResourcesDocument8 pagesDiagnostic and Therapeutic Approach To Abdominal Masses in A Country With Limited ResourcesbrendaNo ratings yet
- Fsurg 09 848565Document10 pagesFsurg 09 848565Jairo Farias OrtizNo ratings yet
- Functional Outcomes of Surgical Treatment of Ureteral Injury Following Gynecological and Obstetrical SurgeryDocument4 pagesFunctional Outcomes of Surgical Treatment of Ureteral Injury Following Gynecological and Obstetrical SurgeryKharizmaNo ratings yet
- Hernia 4Document7 pagesHernia 4Juang Arco TangkasNo ratings yet
- Analysis of Predictors of Complications and Mortality in Postoperative Ventral Hernia SurgeryDocument7 pagesAnalysis of Predictors of Complications and Mortality in Postoperative Ventral Hernia SurgeryCentral Asian StudiesNo ratings yet
- Laparoscopic Versus Open Appendicectomy: A Comparative StudyDocument7 pagesLaparoscopic Versus Open Appendicectomy: A Comparative StudyChristianWicaksonoNo ratings yet
- Isj-5899 oDocument5 pagesIsj-5899 oAbhiram MundleNo ratings yet
- Medip, ISJ-5301 ODocument4 pagesMedip, ISJ-5301 OJesus EspinozaNo ratings yet
- Taap VS Tep en Hernias InguinalesDocument10 pagesTaap VS Tep en Hernias Inguinalesmanuel barrientosNo ratings yet
- 01 HepatogastroDocument3 pages01 Hepatogastroyacine26No ratings yet
- Comparison of Perioperative Outcomes Between Laparoscopic and Open Approach For PancreatoduodenectomyDocument9 pagesComparison of Perioperative Outcomes Between Laparoscopic and Open Approach For PancreatoduodenectomyVu Duy KienNo ratings yet
- Abdelhameed Et Al (June 2019)Document6 pagesAbdelhameed Et Al (June 2019)drpklalNo ratings yet
- Laparoscopic Appendectomy PostoperativeDocument6 pagesLaparoscopic Appendectomy PostoperativeDamal An NasherNo ratings yet
- Management of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondFrom EverandManagement of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondAditi BhattNo ratings yet
- Case Studies of Postoperative Complications after Digestive SurgeryFrom EverandCase Studies of Postoperative Complications after Digestive SurgeryNo ratings yet
- Surgery for Pancreatic and Periampullary Cancer: Principles and PracticeFrom EverandSurgery for Pancreatic and Periampullary Cancer: Principles and PracticeMallika TewariNo ratings yet
- Obesity an Ideological and Discursive AnalysisDocument7 pagesObesity an Ideological and Discursive AnalysisScivision PublishersNo ratings yet
- Osteonecrosis of the Hip a Complication of Radiation Therapy in Cervical Cancer Case Study and Literature ReviewDocument4 pagesOsteonecrosis of the Hip a Complication of Radiation Therapy in Cervical Cancer Case Study and Literature ReviewScivision PublishersNo ratings yet
- Neurorehabilitation Recovery Advances Through Cns NeuromodulationDocument4 pagesNeurorehabilitation Recovery Advances Through Cns NeuromodulationScivision PublishersNo ratings yet
- Digital Media Engagement Childrens Health and Wellbeing a Divide by Family StructureDocument7 pagesDigital Media Engagement Childrens Health and Wellbeing a Divide by Family StructureScivision PublishersNo ratings yet
- Provide Continuity of Care to Psychotic and Schizophrenic Patients Followed in Chud BorgouDocument5 pagesProvide Continuity of Care to Psychotic and Schizophrenic Patients Followed in Chud BorgouScivision PublishersNo ratings yet
- Psychology From a Quantum Physics Perspective Tomorrows MedicineDocument5 pagesPsychology From a Quantum Physics Perspective Tomorrows MedicineScivision PublishersNo ratings yet
- Evaluation of The Knowledge of Mental Health First Aid Among Workers Manning Sick Bays in Schools in EGOR Local Government Area of Benin City, NigeriaDocument4 pagesEvaluation of The Knowledge of Mental Health First Aid Among Workers Manning Sick Bays in Schools in EGOR Local Government Area of Benin City, NigeriaScivision PublishersNo ratings yet
- Moroccan Medical Students Perspectives of Their Educational Environment Qadi Ayyad UniversityDocument7 pagesMoroccan Medical Students Perspectives of Their Educational Environment Qadi Ayyad UniversityScivision PublishersNo ratings yet
- 3d Ct Cinematic Rendering Transforming Forensic Imaging With Enhanced Visualization for Skeletal Trauma AnalysisDocument5 pages3d Ct Cinematic Rendering Transforming Forensic Imaging With Enhanced Visualization for Skeletal Trauma AnalysisScivision PublishersNo ratings yet
- Pupils Perceiving of Greatgrandparent With Dementia a Case StudyDocument2 pagesPupils Perceiving of Greatgrandparent With Dementia a Case StudyScivision PublishersNo ratings yet
- Neuropsychiatric-Imaging in the Depressed Occipital Lobe with A Suicidal Link and Pharmaco-Psychotherapy Outcome Among Pediatric Age Group and AdolescentsDocument8 pagesNeuropsychiatric-Imaging in the Depressed Occipital Lobe with A Suicidal Link and Pharmaco-Psychotherapy Outcome Among Pediatric Age Group and AdolescentsScivision PublishersNo ratings yet
- Budesonide –Oral Galenic Formulations For Chron DiseaseDocument6 pagesBudesonide –Oral Galenic Formulations For Chron DiseaseScivision PublishersNo ratings yet
- A Rare Case of Squamous Cell Carcinoma Following a Cactus Spine InjuryDocument3 pagesA Rare Case of Squamous Cell Carcinoma Following a Cactus Spine InjuryScivision PublishersNo ratings yet
- Future Directions To Explore To Develop Ideal Anti-Cancer Progesterone Receptor ModulatorsDocument8 pagesFuture Directions To Explore To Develop Ideal Anti-Cancer Progesterone Receptor ModulatorsScivision PublishersNo ratings yet
- Cancer Treatment With OncoshuttleDocument4 pagesCancer Treatment With OncoshuttleScivision PublishersNo ratings yet
- Plasma Cell-Free RNA PD-L1 and Survival With Immune Checkpoint Inhibitor Therapy in Metastatic Non-Small Cell Lung CancerDocument6 pagesPlasma Cell-Free RNA PD-L1 and Survival With Immune Checkpoint Inhibitor Therapy in Metastatic Non-Small Cell Lung CancerScivision PublishersNo ratings yet
- A Critical Evaluation of Risk and Protective Factors Influencing the Development and Maintenance of Internalizing Disorders in AdolescentsDocument15 pagesA Critical Evaluation of Risk and Protective Factors Influencing the Development and Maintenance of Internalizing Disorders in AdolescentsScivision PublishersNo ratings yet
- An evaluation of the Training and Education of a Work – Based Learning Programme in a Mental Health Hospital in London: The role of the MatronDocument5 pagesAn evaluation of the Training and Education of a Work – Based Learning Programme in a Mental Health Hospital in London: The role of the MatronScivision PublishersNo ratings yet
- Immunohistochemical and Molecular Evaluation of Oncoprotein HER-2 in Women's Breast Cancer in The Republic of CongoDocument9 pagesImmunohistochemical and Molecular Evaluation of Oncoprotein HER-2 in Women's Breast Cancer in The Republic of CongoScivision PublishersNo ratings yet
- Cancer Science & ResearchDocument4 pagesCancer Science & ResearchScivision PublishersNo ratings yet
- Giant Myxoma of The Right Atrium A Rare Location: A Case Report at The Festoc Center in BamakoDocument3 pagesGiant Myxoma of The Right Atrium A Rare Location: A Case Report at The Festoc Center in BamakoScivision PublishersNo ratings yet
- Results of A Multicentric Study of Patients With Multiple Myeloma Treated With Three Different Triplet Regimens Including BortezomibDocument8 pagesResults of A Multicentric Study of Patients With Multiple Myeloma Treated With Three Different Triplet Regimens Including BortezomibScivision PublishersNo ratings yet
- Anticancer and Antioxidant Effects of Bioactive Extracts From Monk Fruit (Siraitia Grosvenori) With Potential Clinical ImplicationsDocument10 pagesAnticancer and Antioxidant Effects of Bioactive Extracts From Monk Fruit (Siraitia Grosvenori) With Potential Clinical ImplicationsScivision PublishersNo ratings yet
- Trends in Nanocarrier Based Delivery Systems of Methotrexate: Update 2020Document7 pagesTrends in Nanocarrier Based Delivery Systems of Methotrexate: Update 2020Scivision PublishersNo ratings yet
- Cancer Science & ResearchDocument7 pagesCancer Science & ResearchScivision PublishersNo ratings yet
- Impact of Clinicoepimiological Characteristics On The Outcome of Neo Adjuvant Concurrent Chemo Radiation in Locally Advanced Rectal Cancer PatientsDocument9 pagesImpact of Clinicoepimiological Characteristics On The Outcome of Neo Adjuvant Concurrent Chemo Radiation in Locally Advanced Rectal Cancer PatientsScivision PublishersNo ratings yet
- Byebyehiv With Thai InnovationDocument7 pagesByebyehiv With Thai InnovationScivision PublishersNo ratings yet
- Conservative Laparoscopic Surgery Plus Mifepristone For Treating Multifocal Renal Cell CarcinomaDocument4 pagesConservative Laparoscopic Surgery Plus Mifepristone For Treating Multifocal Renal Cell CarcinomaScivision PublishersNo ratings yet
- Sarscov2 Neutralizing Antibody Presence in Infected and Vaccinated PatientsDocument6 pagesSarscov2 Neutralizing Antibody Presence in Infected and Vaccinated PatientsScivision PublishersNo ratings yet
- Cancer Science &researchDocument10 pagesCancer Science &researchScivision PublishersNo ratings yet
- TetanusDocument21 pagesTetanusDebjit SahaNo ratings yet
- CHAPTER 3 Nutrition and Hydration Among Elderly PeopleDocument19 pagesCHAPTER 3 Nutrition and Hydration Among Elderly PeopleIbrahim AyasrehNo ratings yet
- An Update On Canine Coronaviruses Viral Evolution and PathobiologyDocument14 pagesAn Update On Canine Coronaviruses Viral Evolution and PathobiologyVictor FelterNo ratings yet
- Principles of PharmacologyDocument9 pagesPrinciples of Pharmacologybencleese100% (1)
- TIMERS Consenso-1Document52 pagesTIMERS Consenso-1Osvaldo BorralhoNo ratings yet
- Oral Malignant Melanoma - A Case ReportDocument6 pagesOral Malignant Melanoma - A Case Reportvaal6316No ratings yet
- Medical Form For All ApplicantsDocument2 pagesMedical Form For All ApplicantsHaason TzNo ratings yet
- Algoritma CKD PDFDocument2 pagesAlgoritma CKD PDFDesla Citra100% (1)
- Vim Ax Extender User ManualDocument7 pagesVim Ax Extender User ManualEnche Engku Wan TanjongNo ratings yet
- Pharma - Week 3 (Drug Calculations)Document5 pagesPharma - Week 3 (Drug Calculations)MIKAELA DAVIDNo ratings yet
- Brief Gelicart Colageno HidrolizadoDocument8 pagesBrief Gelicart Colageno HidrolizadoJenni KortezNo ratings yet
- 4 Advantages of Weight Training For Women by Julie Gabbard-1Document6 pages4 Advantages of Weight Training For Women by Julie Gabbard-1Teodora RadićNo ratings yet
- Overview: Mechanisms of Hypertension: Cells, Hormones, and The KidneyDocument3 pagesOverview: Mechanisms of Hypertension: Cells, Hormones, and The KidneyTemesgen EndalewNo ratings yet
- Auerbach - Frostbite PDFDocument30 pagesAuerbach - Frostbite PDFAlNo ratings yet
- Diabetic Ketoacidosis: ISPAD Clinical Practice Consensus Guidelines 2006-2007Document16 pagesDiabetic Ketoacidosis: ISPAD Clinical Practice Consensus Guidelines 2006-2007ka7lonNo ratings yet
- Articulo Ingles BiopsiaDocument9 pagesArticulo Ingles BiopsiaJamileth MartinezNo ratings yet
- Ketogenic diet and metabolic therapies : expanded roles in health and disease 1st Edition Susan Masino 2024 scribd downloadDocument52 pagesKetogenic diet and metabolic therapies : expanded roles in health and disease 1st Edition Susan Masino 2024 scribd downloadpuricozzo100% (3)
- Artículo Khoury2018Document10 pagesArtículo Khoury2018Basma Derdabi100% (2)
- Dental CariesDocument18 pagesDental CariesRahayu Sukma Dewi0% (1)
- Effectiveness of Self Instructional Module (Sim) On Knowledge Regarding The Prevention of Hiv/aids Among Students Studying in Selected Degree CollegeDocument24 pagesEffectiveness of Self Instructional Module (Sim) On Knowledge Regarding The Prevention of Hiv/aids Among Students Studying in Selected Degree CollegeAnshul Nandi100% (2)
- Frisoni-11 Criterios ADDocument4 pagesFrisoni-11 Criterios ADMARIA MONTSERRAT SOMOZA MONCADANo ratings yet
- Disease Prioritization For Surveillance Workshop Report NIH 2015Document14 pagesDisease Prioritization For Surveillance Workshop Report NIH 2015TanzeerNo ratings yet
- Case StudyDocument12 pagesCase Studyapi-291857811No ratings yet
- Nutrition Journal of Parenteral and EnteralDocument8 pagesNutrition Journal of Parenteral and EnteralFirdausi RiskiviawinandaNo ratings yet
- Training Standards in Implant Dentistry 2016Document13 pagesTraining Standards in Implant Dentistry 2016Ramona RochianNo ratings yet
- Virgin Coconut Oil and Oil PullingDocument3 pagesVirgin Coconut Oil and Oil PullingSusyary SNo ratings yet