Report of Two Cases Arwinder Singh Gill 1,2, Muhammad Firdaus 1, Yosafat Kurniawan Sugiarto 3, Farilaila Rayhani 4, Rini Andriani 5, Ahmad Faried 3* 1 Department of Neurosurgery, Dharmais Cancer Hospital – National Cancer Center, Jakarta, Indonesia 2 Faculty of Medicine, Tarumanagara University, Jakarta, Indonesia 3 Department of Neurosurgery, Faculty of Medicine, Universitas Padjajaran – Dr. Hasan Sadikin Hospital, Bandung, Indonesia 4 Department of Anatomical Pathology, Dharmais Cancer Hospital – National Cancer Center, Jakarta, Indonesia; 5 Department of Neurology, Dharmais Cancer Hospital – National Cancer Center, Jakarta, Indonesia
ARTICLE INFO ABSTRACT
Received : 13 June 2023 Introduction: Cerebral tuberculoma, a seldom encountered and severe manifestation of Reviewed : 18 July 2023 tuberculosis (TB), arises from the dissemination of Mycobacterium tuberculosis through the Accepted : 25 September 2023 bloodstream. Its symptoms and radiological characteristics lack specificity, often resulting in diagnostic errors. Management predominantly involves medical intervention, with the treatment Keywords: duration for cerebral tuberculoma ranging from 6 to 36 months. In specific instances, surgical brain tumor, cerebral tuberculoma, intervention may be advised . tuberculosis, mimicking lesion
Case Presentation: We reported two cases of cerebral tuberculoma occurring in patients who presented with seizures, with space-occupying lesions evident on magnetic resonance imaging *Corresponding author: of the brain. There were no symptoms of concurrent extra cranial TB. Surgery was performed Ahmad Faried on both of the cases and anti-TB treatment began as soon as the diagnosis was made with Department of Neurosurgery, Faculty corticosteroid as adjuvant treatment. of Medicine, Universitas Padjadjaran, Jl. Pasteur No. 38, Bandung 40161, Conclusions: A combination of clinical, radiological, and histopathological examination is needed West Java, Indonesia. to confirm the diagnosis and determine the appropriate therapy. If ICP is increased as a result of ahmad.faried@unpad.ac.id the lesion and medical therapy has failed, surgical excision is required.
INTRODUCTION Despite Indonesia’s progress, it remains third in the
world for new TB cases. Pulmonary TB is the predominant Tuberculosis (TB) stands as among the most ancient clinical presentation, accounting for 85.67% of cases, infectious ailments in human history, attributed to contrasting with extrapulmonary TB at 14.75%. Mycobacterium tuberculosis. Its prevalence persists Extrapulmonary TB, particularly affecting the central notably in developing nations, impacting a considerable nervous system (CNS), represents one of the most severe segment of the global populace. TB has the capability manifestations, afflicting approximately 2-15% of cases, to afflict nearly all bodily tissues, encompassing the with the highest incidence among individuals with central nervous system, where it manifests as one of acquired immunodeficiency syndrome (AIDS) [1]. the most severe variants [1]. We report two cases of intracranial tuberculoma The 2020 WHO global report revealed that Southeast without any prior history of immunodeficiency. Both Asia (43%), Africa (25%), and the Western Pacific (18%) cases were managed surgically due to refractory seizures regions harbored the highest incidences of TB cases, and the mass effect of space-occupying lesions. Anti-TB while smaller proportions were observed in the Eastern treatments were administered in both cases with Mediterranean (8.3%), the Americas (3.0%), and Europe corticosteroid as adjuvant therapy. (2.3%). The primary impact of the COVID-19 pandemic on TB was a substantial decrease globally in newly CASE PRESENTATION diagnosed TB cases reported in 2020 compared to 2019. Indonesia, ranking second only to India, significantly This case report has been reported in line with the contributed to this global decline from 2019 to 2020. SCARE 2020 criteria [2] and has been approved by our
Indonesian Journal of Cancer, Vol 18(1), 72–76, March 2024 72 |
DOI: http://dx.doi.org/10.33371/ijoc.v18i1.1084 Cerebral Tuberculomas Mimicking A Brain Tumor Y O S A FAT K U R N I AWA N , E T A L
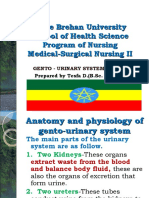
ethics committee No LB.02.01/X.6.5/69/2022. Patients 1.8 cm, with significant perifocal edema and compression provided written consent for the publication of this of the right lateral ventricle as seen in Figure 1. report and the accompanying images. The patient underwent surgery for excision of the tumor mass and histopathological examination of the Case 1 specimen acquired. The tumor was brownish white filled A 59-year-old woman presented to the neurology with yellowish pus. Tuberculoma was confirmed with clinic with focal seizures in her left limb. An episode granulomatous inflammation, locally visible tubercle of clonic-type seizure was reported, without loss of formation consisting of epithelioid proliferation, caseous consciousness during the seizure. She disclosed a history necrosis, and indistinct multinucleated giant cells. Anti- of night sweats and weight loss. He denied having ever HIV examination, expert genes, and cerebrospinal fluid experienced a fever, a seizure, or a lost consciousness. (CSF) culture showed negative results. Anti-TB medication The patient had no substantial family history, no history with isoniazid, rifampicin, pyrazinamide, and ethambutol of surgery, or daily medication. He had a healthy for 18 months with the addition of streptomycin for 2 immune system and had never used immunosuppressive initial months was administered with dexamethasone drugs or experienced repeated infections. Neurological as adjuvant treatment. The patient’s symptoms improved examination showed that the patient was fully conscious after being given dexamethasone adjuvant therapy. with peripheral left side cranial nerve VII, cranial nerve There were no adverse events and the frequency of XII central, left cranial nerve IX, and X palsy with a the seizures decreased gradually and eventually stopped. slight motoric weakness on left upper limb (motor At the end of the treatment, another serial brain MRI strength 5/5/4/5). No sensory or autonomy deficit was was performed for evaluation, and the granulomatous found. 5 years before this visit, the patient had a history lesion of the right parietal lobe was resolved (Figure 2). of pulmonary TB and had completed the anti-TB treatment for 6 months. The patient has had a chest Case 2 X-ray done and there is no sign of TB in the lungs. The A 28-year-old man presented to the neurosurgery HIV test’s serology came out negative, and the ESR clinic with weakness in his left limb and a history of (erythrocyte sedimentation rate) increased by 62 mm/ uncontrolled focal seizure despite already being on hour. The patient’s brain MRI revealed a well-defined medication for six months. With no medical history, nodular lesion with a hemorrhagic component in the presented with the first seizures in her life and a history right parietal lobe which enhanced significantly after of fever, headache, vertigo, nausea, vomiting, and contrast was delivered. The size of the lesion was 2.3 × tendencies to fall to the right side when standing.
Figure 1. Axial section T1-weighted image
with gadolinium contrast on magnetic resonance imaging (MRI). (A) Preoperative; (B) Evaluation after anti-tuberculosis treatment for 18 months was completed.
Figure 2. T1-weighted image
with gadolinium contrast on MRI before the surgery. (A) Axial Section; (B) Coronal Section; (C) Sagittal Section.
www.indonesianjournalofcancer.or.id 73 | P-ISSN: 1978-3744 E-ISSN: 2355-6811 Cerebral Tuberculomas Mimicking A Brain Tumor Y O S A FAT K U R N I AWA N , E T A L
A neurological examination revealed a normal cerebellar immunocompromised risk in the patient. Anti-TB function test. Neurological examination showed that treatment was started as soon as the diagnosis was the patient was fully conscious with motoric weakness made with a combination of isoniazid, rifampicin, on the left lower limb. No sensory or autonomy deficit pyrazinamide, and ethambutol scheduled for 12 months was found. Cranial nerve examinations were normal with the addition of streptomycin for the 2 initial without any deficit. He had previously undergone months. The patient also had dexamethasone therapy craniotomy at another hospital 6 months before the for 1 month. The patient symptoms clinically improved visit with histopathology concluding an atrocytoma. The after dexamethasone adjuvant therapy. Throughout the sample was re-assessed at our center and the new result treatment, episodes of seizure still occurred but with was tuberculoma (Figure 3). longer intervals compared to pre-surgery conditions. The patient never had a previous history of TB. There were continuous focal seizures of the left limb which DISCUSSION could not be controlled by antiepileptic drugs. The patient had done a chest x-ray and no new cavitation Tuberculosis stands as one of the deadliest infectious was found in the lung. The HIV test’s serology came diseases globally. While it typically affects the respiratory out negative, and the erythrocyte sedimentation rate system, CNS TB accounts for approximately 5 to 15% of (ESR) increased by 72 mm/hour. Brain MRI on T1- extrapulmonary cases, posing the highest risks of weighted image showed multiple hyperintense lesions morbidity and mortality. Central nervous system TB can predominantly on the right parietal region with perifocal be categorized into three types: tuberculous meningitis edema. The main lesion was 2.4 x 2.1 cm in size (TBM), spinal arachnoiditis, and cerebral tuberculoma, as surrounded by smaller lesions of 1.3 x 1.3 cm. A exemplified in the cases discussed in our report [3,4,5]. craniotomy was decided as the lesion was not typical It is widely believed that the bacilli enter the central for the diagnosis of astrocytoma. The tumor was firm nervous system through the bloodstream, typically as in consistency with clear margins and had necrotic fluid a result of tuberculosis occurring elsewhere in the body. draining from the center of the lesion. The tumor was Rich and McCordock’s initial description proposed that removed microscopically and the large draining veins tuberculous lesions form in the brain during the were preserved as seen in Figure 4. bacteremia stage [6]. In theory, tuberculosis has the A cerebrospinal fluid culture was performed and potential to breach the blood-brain barrier (BBB) either showed microorganisms and gram stain results were as a free organism outside cells or through monocytes/ negative. HIV testing showed negative results and blood neutrophils carrying the bacilli [7]. The rupture of one sugar levels were within normal limits which ruled out or multiple lesions can lead to the development of CSF
Figure 3. The preparation showed tubercles made up of histiocyte cells, epithelioid cells, lymphocyte cells, and an extensive case of necrosis in the brain tissue. Blood vessels can be found in some of them with original magnification of 4x, 10x, and 40x, respectively.
Figure 4. (A) Necrotic fluid at the center of the mass which was yellowish; (B) The large tumor was firm with marked borders that were adherent to the draining vein; (C) Careful lesion dissection showed total removal with preservation of the vein.
www.indonesianjournalofcancer.or.id 74 | P-ISSN: 1978-3744 E-ISSN: 2355-6811 Cerebral Tuberculomas Mimicking A Brain Tumor Y O S A FAT K U R N I AWA N , E T A L
TB. These lesions commonly originate in the meninges, growths and tend to occur more frequently in the frontal subpia, or subependymal surface of the brain. The and parietal lobes [13]. growth of these lesions is understood to be influenced The inflammatory reaction triggered by TB infection by the immune system [8]. Individuals diagnosed with is characterized by granulomatous inflammation, human immunodeficiency virus (HIV) infection face a featuring epithelioid macrophages and Langhans’ giant significantly heightened risk of tuberculoma, cells, alongside lymphocytes, plasma cells, a small approximately five times greater than those without number of PMNs, fibroblasts with collagen, and HIV. Immunodeficiency, whether due to HIV or organ distinctive caseous necrosis at the core. This inflammatory transplantation and subsequent prolonged use of response is driven by a type IV hypersensitivity reaction immunosuppressive drugs, increases the susceptibility [7,8,13]. Current treatment for CNS TB typically involves to tuberculosis. For recipients of solid organ transplants, medical therapy, comprising a regimen including the likelihood of developing TB rises by 20–74%. isoniazid, ethambutol, pyrazinamide, rifampicin, and Additionally, approximately 8% of tuberculoma cases steroids. This treatment regimen often leads to a are linked to patients having concurrent diabetes [9]. reduction in tuberculoma size and complete resolution In instances where a tuberculoma grows to a within three months, although in some cases, a longer considerable size, it may resemble a brain tumor, duration of up to three years may be necessary. Patients exerting pressure on nearby brain tissue and eliciting with elevated intracranial pressure should undergo symptoms indicative of heightened intracranial pressure immediate neurosurgical evaluation. Surgical resection (ICP), such as headaches, nausea, and vomiting. Seizures may be necessary for tuberculomas to alleviate mass are typically the primary symptom upon presentation effect, as prompt removal can significantly enhance with tuberculoma, as observed in our case. Distinguishing overall outcomes, even in cases of drug resistance or granulomas from other brain-expansive lesions based paradoxical worsening, affecting up to 25% of treated solely on neurological symptoms is challenging, as these TB patients. However, this study’s limitation lies in its symptoms are contingent upon the location and size inability to establish a causal relationship between of the lesion. Manifestations of intracranial hypertension adjuvant steroids and patient outcomes, as well as the and seizures are commonly encountered [1,11]. Cerebral impact of surgery on symptom improvement. Future tuberculomas are solid, non-vascular, rounded growths studies, such as larger case series or multicenter ranging in size from 2 to 10 cm in diameter. They exhibit research, are warranted. The choice of surgical approach well-defined boundaries, and the adjacent brain tissue, may vary based on factors including tuberculoma under pressure, may exhibit swelling and gliosis. Within location, surrounding vascular and nerve structures, the mass, there are regions of necrotic caseation where cortical involvement, and surgeon preference [1,10,13,14]. tubercle bacilli may be detected [12]. These are the primary attributes of these lesions, which were also CONCLUSIONS observed during surgical intervention in our cases. They were successfully excised due to their clearly demarcated Over the past few decades, there has been a borders from the adjacent brain structures. remarkable improvement in the prognosis of cerebral Considering tuberculoma in the list of possible tuberculoma, shifting from a prognosis nearly fatal to diagnoses is crucial when encountering solitary intracranial one where over 80% of patients survive with timely mass lesions. However, diagnosing it poses challenges treatments. Considering the possibility of tuberculoma because the neuroimaging presentations can vary and is essential when evaluating CNS masses, even in lack specificity. Tuberculomas typically appear on brain patients without a history of TB elsewhere, to ensure scans as isodense or hyperdense lesions, sometimes with prompt and appropriate treatment. While imaging calcifications, and exhibit ring enhancement following studies are supportive, they do not conclusively confirm contrast administration. The presence of calcifications on the diagnosis of brain tuberculoma, and both prognosis CT scans along with ring enhancement, termed the “target and treatment differ from other brain lesions. A sign,” is regarded by some authors as potentially specific histological diagnosis achieved through surgical excision to tuberculoma. MRI is more adept than CT scans at not only confirms the diagnosis but also helps alleviate identifying small tuberculomas and those situated in the symptoms of increased intracranial pressure. brainstem. Typically, tuberculomas display intermediate or low signal intensity on T1-weighted images, DECLARATIONS accompanied by ring enhancement post-injection of gadolinium. On T2-weighted sequences, they typically Competing of Interest exhibit low signal intensity with surrounding edema The authors declare no competing interest in this study. [1,12]. The lesion locations align with documented literature, as they can manifest as solitary or multiple Acknowledgment Not applicable
www.indonesianjournalofcancer.or.id 75 | P-ISSN: 1978-3744 E-ISSN: 2355-6811 Cerebral Tuberculomas Mimicking A Brain Tumor Y O S A FAT K U R N I AWA N , E T A L
REFERENCES 8. Bermudez LE, Sangari FJ. Cellular and molecular
mechanisms of internalization of mycobacteria by 1. Perez-Malagon CD, Barrera-Rodriguez R, Lopez- host cells. Microbes Infect. 2001;3(1):37–42. Gonzalez MA, Alva-Lopez LF. Diagnostic and 9. Nelson CA, Zunt JR. Tuberculosis of the central Neurological Overview of Brain Tuberculomas: A nervous system in immunocompromised patients: Review of Literature. Cureus. 2021 Dec 3;13(12):e20133 HIV infection and solid organ transplant recipients. 2. WHO Global. Global Tuberculosis Report 2020 Clin Infect Dis. 2011;53(9):915–26. [Internet]. World Health Organization. 2020. 10. Rajeswari R, Sivasubramanian S, Balambal R, et al. Available from: https://www.who.int/publications/i/ A controlled clinical trial of short-course item/9789240013131 chemotherapy for tuberculoma of the brain. Tuber 3. Prihutomo S, Slamet, Rustandi K. Pedoman Nasional Lung Dis. 1995;76(4):311–7. Pelayanan Kedokteran Tata Laksana Tuberkulosis. 11. Gregol BM, Berres TO, Barreto T, et al. Brain Kementrian Kesehatan Republik Indonesia 2015; 2015. Tuberculoma as a Differential Diagnosis of Single 4. DeLance AR, Safaee M, Oh MC, et al. Tuberculoma Intracranial Lesion: Case Report. Arq Bras Neurocir of the central nervous system. J Clin Neurosci. Brazilian Neurosurg. 2020;39(02):142–5. 2013;20(10):1333–41. 12. Moussa AA, Mahmoud ME, Yousef HA. Intracranial 5. Leonard JM. CNS Tuberculosis. In: Microbiol Spectr. tuberculoma and recent advances in magnetic 2017. p. 17–44. resonance imaging. Egypt J Neurosurg. 2018;33:1–5. 6. Davis AG, Rohlwink UK, Proust A, Figaji AA, 13. Marais S, Van Toorn R, Chow FC, et al. Management Wilkinson RJ. The pathogenesis of tuberculous of intracranial tuberculous mass lesions: how long meningitis. J Leukoc Biol. 2019 Feb;105(2):267-280. should we treat for? Wellcome Open Res. 2019;4. 7. Be N, Kim K, Bishai W, Jain S. Pathogenesis of 14. Jacobs RF, Sunakorn P, Chotpitayasuno T, et al. Central Nervous System Tuberculosis. Curr Mol Intensive short course chemotherapy for tuberculous Med. 2009 Mar 1;9(2):94–9. meningitis. Pediatr Infect Dis J. 1992;11(3):194–7.