With so much to hear and see at the beginning of the interview,
why not consciously set aside the first minute or two for the patient and concentrate on listening and facilitating rather than questioning? Listening attentively instead of moving immediately to a series of questions about the history allows us to achieve more of our objectives. Although it requires very little time, using these early moments of the consultation wisely pays off handsomely. OBTAINING THE AGENDA (CHIEF CONCERN/COMPLAINT AND OTHER ACTIVE PROBLEMS) (STEP 2) In Step 2, you will focus on the patient and setting the agenda for the interview. This fosters the patient-centered interaction to follow (Steps 3 and 4) because it orients and empowers the patient and ensures that her or his concerns are properly prioritized and addressed. Some clinicians unwittingly preclude agenda setting by saying “What brings you in today?” or “How are you doing?” Patients interpret these phrases as an invitation to tell the story of the first concern on their list, rather than generating a list of concerns. This often leads clinicians to miss important information and fail to meet patients’ expectations. Setting an agenda usually takes little time, improves efficiency, empowers patients, and yields increased data. However, it is not necessarily easy and serious pitfalls can arise if it is conducted improperly. 2
The four-part approach to identifying the patient’s agenda,
namely: 1 opening question 2 listening 3 screening 4 confirming offers many advantages to the doctor and the patient over the more traditional alternative of: 1 asking 2 assuming 3 proceeding. The following four substeps, summarized in Table 3-2, usually are performed in the order given. It generally takes no more than 1–2 minutes, but can take longer if the patient has many concerns. 1 Indicate time available 2. Forecast what you would like to have happen in the interview 3. Obtain list of all issues patient wants to discuss; eg, specific symptoms, requests, expectations, understanding 4 Summarize and finalize the agenda; negotiate specifics if too many agenda items TABLE 3-2. Step 2: Chief Concern/Agenda Setting (1–2 min) 3
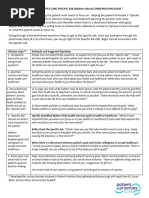
Step 2 Elicit chief concern & set agenda (1–2 min.)
7. Indicate time available (e.g. “We’ve got about 20 minutes together today…”) 8. Forecast what you would like to have happen in the interview (e.g. “…and I see that we need to review the blood tests you had done yesterday,…”) 9. Obtain list of all issues patient wants to discuss; specific symptoms, requests, expectations, understanding (e.g. “…but before we do that, it would help me to get a list of the things you wanted to discuss today.” “Is there something else?”) 10. Summarize and finalize the agenda; negotiate specifics if too many agenda items (e.g., “You mentioned 8 things you were hoping to cover. In the time we have together today, I don’t think we can address them all. Can you tell me which one or two are most troublesome for you; we’ll do a good job with those and I’ll see you back soon to work on some of the others.”) 4
Screening In the discussion above, we have seen how using an appropriate opening question combined with attentive listening and specific facilitation skills allows the physician to discover more of the patient’s agenda in the early part of the consultation. Now we would like to explore how making a further deliberate attempt to discover all of the patient's problems before actively exploring any one of them can further increase the accuracy and efficiency of consultations. Screening is the process of deliberately checking with the patient that you have discovered all that they wish to discuss by asking further open-ended enquiries. Rather than assuming that the patient has mentioned all of their difficulties double-check: 'So you've been getting headaches and dizziness lately. Has anything else been bothering you?' If the patient continues, resume listening until they stop again. Then repeat the screening process until eventually the patient says that they have finished: 'So you've also been feeling very tired and irritable and were wondering if you might be anemic. Anything else at all?' At the end of this process when the patient says 'NO, THAT'S ABOUT IT', you might wish to confirm your understanding and give the patient an opportunity to know what you have heard: 'So as I understand it, you've been getting headaches and dizziness but have also been feelingtired, rather irritable and a bit low, and your concern was that you might be anemic. Did I get that right?' Often this method of checking reveals symptoms and concerns relating to the initial complaint, but the patient might not yet 5
have revealed a totally separate problem. You might wish to
perform one last check here: 'I can see these symptoms must have been worrying to you and we’ll need to explore them further in a minute: first let me just check whether there are any other areas that you hope I might be able to help you with today as well'. The patient might then produce a second problem area, 'Well, I’ve also got this terrible cough' or a social problem, 'Well, I’m really terribly worried about my daughter'. Without this check, you might first discover these issues at the end of the consultation and not have any time or patience left to deal with them. For the doctor, there is a better chance of discovering the patient's full agenda, negotiating how best to use the time available and pacing the interview appropriately. Screening also provides a way for doctors to check out their expectations and assumptions about why the patient may have come or what they want to talk about, helping the doctor to keep an open mind. For the patient, screening establishes mutually understood common ground and provides the reassurance that you are really interested in their problems and thoughts - both in turn enhance trust and disclosure. Helping the patient to reveal their most important problems early on prevents their attention from remaining focused on how and when to introduce their unstated concern rather than on the agenda in progress (Korsch et al. 1968; Mehrabian and Ksionsky 1974). 6
Screening helps to prevent uncertainty in the patient's mind
leading to distraction and blocking effective communication. Patients may of course still reveal their underlying problem, their hidden agenda, later in the interview when they have tested the water and gained confidence in the relationship. Screening encourages but does not guarantee early problem identification, and we must still remain open to late-arising complaints and be sensitive to the reasons that the patient might have for delaying their introduction. Several North American teaching texts now propose the following sequence for the early part of the consultation (Riccardi and Kurtz 1983; Lipkin 1987; Cohen-Cole 1991): • encouraging the patient to discuss their main concerns by attentive listening without interruption or premature closure • confirming the list identified so far by summarizing • checking repeatedly for additional concerns ('Is there anything else you wish to discuss today?') until the patient indicates that there are none • negotiating an agenda for the consultation. 7
In certain interviews it is possible and beneficial to be quite 'up
front' about screening and to explain your plan to the patient straight away. So, as an example, the patient referred to aspecialist might receive the following introduction: 'Hello, I’m Dr Smith. I’ve got a letter from your GP so I've got some idea of why you've come today, but I’d like to hear the story from you first hand and then try to help as best I can. I’d like to start if you agree with us making a list of all the problems you've been having or things you'd like help with and then we can explore them together in more detail.' This approach makes the structure very clear to the patient. It makes it apparent that the doctor wants to understand the whole of their agenda from the start and will then attend to all of their concerns. Otherwise the patient may not know if they are expected to move ahead with one problem or to mention them all briefly. At the other extreme, a patient who enters the room and immediately breaks into a story that they clearly need to tell, or a patient who on sitting down dissolves into tears because her father has just died, deserves our full attention now. Here listening takes priority over screening, It would be inappropriate to interrupt and say 'We’ll come back to that - is there anything else that you would like to discuss today?'! Some patients come with a pre-written list, giving the doctor a perfect opportunity to screen the agenda and negotiate what is possible in the time available today. Other patients come with a well-rehearsed speech that they have nervously prepared - the telling of it is essential for the patient's peace of mind before the doctor and patient can settle down to work together. Often this 8
opening statement can be so rich in feelings, thoughts, ideas,
concerns and expectations and give such clues to the patient’s life-world that it would be a mistake not to give the patient the floor to express their story. If you do not listen first, you might well miss clues that could be important in helping the patient with their problem. This dilemma can be resolved by another of the principles of communication that we have already discussed, namely dynamism. What is appropriate for one situation is inappropriate for another and we have to continually monitor how best to approach the consultation as we proceed. Knowing that it is helpful to both listen and screen and being flexible enough to use both appropriately in different situations is the key. Agenda setting Screening naturally leads on to negotiating and setting an agenda, taking both the patient’sand the doctor’s needs into account ). In keeping with our emphasis on developing a partnership between patient and physician - a collaborative relationship - this is an overt and involving approach to clarifying how the interview should proceed. There are many advantages to this over simply moving forward without explaining the process to the patient. For the doctor, organisation of thought prevents aimless or unnecessary questioning and incomplete data gathering. For the patient, the structure of the interview is made overt and an opportunity is provided for more involvement and more responsibility in what is taking place. 9
Interestingly, Levinson et al. (1997) showed that primary care
physicians who educated the patient about what to expect and the flow of the visit were less likely to have suffered malpractice claims. Notice that in agenda setting and negotiating you are not just telling the patient what to do but are inviting them to participate in making an agreed plan. One of the principles of communication was that effective communication promotes an interaction rather than a process of direct transmission. Cassata (1978) explained how crystallising agendas at the beginning of the consultation promotes just such an interaction - a two-way communication that encourages the patient to be a more active, responsible and autonomous participant throughout the consultation. Another of our five principles concerned reducing uncertainty. Here, overt agenda setting does just that by establishing mutually understood common ground. 10
Agenda setting is another example of structuring the
consultation. Priorities can be established and negotiated: 'Shall we start with the new problems, the diarrhea and the fever, and then move on to the problems you have been having with your medication?' The doctor's agenda can also be added: 'OK, let's think about your headaches and then look at the rash. I wouldn't mind checking on your blood pressure and your thyroid tablets, too, later on, if that's all right.' Problems with time can be acknowledged and negotiated: 'That's quite a list for us to get through and I'm not sure that we are going to have enough time to do it all justice. How about… ?' In negotiating priorities, a balance may need to be struck between the patient's personal hierarchy of concerns and the doctor's medical understanding of which problems might be more immediately important: 'I can see that the arthritis is the thing that's really bothering you most today, but if you