DM 2022
DM 2022
Download as pdf or txt
You might also like
- Diabetes PPT FinalDocument39 pagesDiabetes PPT Finalimee c100% (1)
- Endocrinology Pastest PDFDocument645 pagesEndocrinology Pastest PDFDr-Jahanzaib Gondal100% (1)
- 5 DM - Introduction, Diagnosis& ComplicationsDocument81 pages5 DM - Introduction, Diagnosis& ComplicationsLexis SanchizieNo ratings yet
- Diabetes MellitusDocument43 pagesDiabetes MellitusCece RereNo ratings yet
- 2018 - DR Iin - SLIDE KULIAH DM2Document95 pages2018 - DR Iin - SLIDE KULIAH DM2DhiastikaNo ratings yet
- By: Emad Qassim Khaleel Ghassan Mahmood Khalaf Firas Khalaf EidoDocument38 pagesBy: Emad Qassim Khaleel Ghassan Mahmood Khalaf Firas Khalaf EidoEmad Qasim KhaleelNo ratings yet
- Diabetes MellitusDocument79 pagesDiabetes Mellituskhalid saifur rahman khanNo ratings yet
- DiabetesDocument35 pagesDiabetesyutisharma17No ratings yet
- 222 Diabetes 2Document61 pages222 Diabetes 2Rahman Md.MoshiurNo ratings yet
- Diabetes MellitusDocument25 pagesDiabetes Mellitusdhaaraniss04No ratings yet
- Diabetes MellitusDocument20 pagesDiabetes MellitusMARIA TARIQNo ratings yet
- Bio Project On DiabetesDocument17 pagesBio Project On DiabetesNishant Kumar100% (1)
- Diabetes MellitusDocument6 pagesDiabetes MellitusChristian YuNo ratings yet
- Diabetes Mellitus and HomeopathyDocument9 pagesDiabetes Mellitus and HomeopathyImran Shafqat100% (2)
- Adult Onset Diabetes Mellitus Management Options: DR Muhammad Israr Ul HaqDocument88 pagesAdult Onset Diabetes Mellitus Management Options: DR Muhammad Israr Ul HaqMuhammad Israr Ul HaqNo ratings yet
- Review of Diabetes Mellitus: Loo Hariyanto Raharjo, DR., Msi. Ketua Program Studi Pendidikan Dokter Fk-UwksDocument51 pagesReview of Diabetes Mellitus: Loo Hariyanto Raharjo, DR., Msi. Ketua Program Studi Pendidikan Dokter Fk-UwksBerlia NarayaniNo ratings yet
- Diabetes Melitus Group 4Document10 pagesDiabetes Melitus Group 4ahmad rizalNo ratings yet
- Diabeties NewDocument54 pagesDiabeties NewDipti SharmaNo ratings yet
- 11 DiabetesDocument116 pages11 DiabetesRahman Md.MoshiurNo ratings yet
- "Diabetes": ACADEMIC YEAR: 2020-22 Department: Master in Public Health Assignment ONDocument27 pages"Diabetes": ACADEMIC YEAR: 2020-22 Department: Master in Public Health Assignment ONNeeru ChaudharyNo ratings yet
- 15 - DiabetesDocument49 pages15 - Diabetesallakami777yousefNo ratings yet
- Diabetes Younes Ferwana Mohamed MehgizDocument43 pagesDiabetes Younes Ferwana Mohamed MehgizHakim oğluNo ratings yet
- A Review On Use of Nanoparticles in The Treatment of Diabetes Mellitus (Tichakunda Xavier Mharazanye, Naina, Mninderjeet KaurDocument14 pagesA Review On Use of Nanoparticles in The Treatment of Diabetes Mellitus (Tichakunda Xavier Mharazanye, Naina, Mninderjeet KaurmharazanyetichakundaxavierNo ratings yet
- Diabetes MellitusDocument12 pagesDiabetes Mellitusmarkangelo.pagulayanNo ratings yet
- Diabetes MellitusDocument5 pagesDiabetes MellitussujithasNo ratings yet
- Diabetes Mellitus , Au,Asell BestDocument191 pagesDiabetes Mellitus , Au,Asell Bestnegamebratu2024No ratings yet
- PK - DR Toni - Metab Karbo Dan DMDocument32 pagesPK - DR Toni - Metab Karbo Dan DMAyu DewiNo ratings yet
- 4.2) Diabetes MellitusDocument212 pages4.2) Diabetes MellitusahmedNo ratings yet
- Biology Investigatory ProjectDocument15 pagesBiology Investigatory ProjectRita NayakNo ratings yet
- Bka Case FinalDocument26 pagesBka Case FinalJayson SorianoNo ratings yet
- Diabetes MelitusDocument44 pagesDiabetes MelitusDwi Novianti SugihartiNo ratings yet
- Diabetes Mellitus in PaedDocument37 pagesDiabetes Mellitus in Paedkoromamosesjohn142No ratings yet
- DiabetesDocument42 pagesDiabetesminahil qadeerNo ratings yet
- ENDO DiabetesDocument9 pagesENDO DiabetesHajime NakaegawaNo ratings yet
- Dr. Pragasam Viswanathan Professor, SBSTDocument43 pagesDr. Pragasam Viswanathan Professor, SBSTMaru Mengesha Worku 18BBT0285No ratings yet
- IntroductionDocument22 pagesIntroductionjayrana40No ratings yet
- Diabetes Mellitus: Group 3ADocument8 pagesDiabetes Mellitus: Group 3AAradhanaRamchandaniNo ratings yet
- IntroductionDocument13 pagesIntroductionSaadNo ratings yet
- Diabetes Mellitus Type2: Case StudyDocument48 pagesDiabetes Mellitus Type2: Case StudyJohn Carlo GarciaNo ratings yet
- Diabetes MellitusDocument52 pagesDiabetes MellitusMervis masatunyaNo ratings yet
- Physiology and Causes of DiabatesDocument7 pagesPhysiology and Causes of DiabatesasaadsarfrazNo ratings yet
- Diabetes MellitusDocument24 pagesDiabetes MellitusAnsh Gaurav KumarNo ratings yet
- DIABETES MELLITUS (1)Document33 pagesDIABETES MELLITUS (1)nouman khanNo ratings yet
- Diabetes MellitusDocument13 pagesDiabetes Mellitusdreneavalentinstefan100% (1)
- DIABETES MELLITUS FFDocument131 pagesDIABETES MELLITUS FFCHEGE CAROLYNE NJOKINo ratings yet
- (4-5) Diabetes MellitusDocument18 pages(4-5) Diabetes Mellitusipadhi35No ratings yet
- Continuing Education Activity: Diabetes Mellitus Type 2Document7 pagesContinuing Education Activity: Diabetes Mellitus Type 2Chiki CacaNo ratings yet
- Diabetes MellitusDocument110 pagesDiabetes MellitusToluwani Lade-ige100% (1)
- Dr. Rasha Salama: PHD Public Health, Suez Canal University, Egypt Diabetes MSC, Cardiff University, United KingdomDocument37 pagesDr. Rasha Salama: PHD Public Health, Suez Canal University, Egypt Diabetes MSC, Cardiff University, United Kingdomdwi istutikNo ratings yet
- Management of Diabetis MellitusDocument24 pagesManagement of Diabetis MellitusTasmia TasnimNo ratings yet
- Diabetes Mellitus DMC 6th SemesterDocument23 pagesDiabetes Mellitus DMC 6th SemesterHuzaifa CHNo ratings yet
- DIABETESDocument39 pagesDIABETESSaboorMalikNo ratings yet
- Final Addition ResearchDocument25 pagesFinal Addition Researchweeew930No ratings yet
- Diabetes Mellitus: WAHYUDI, S.Farm., AptDocument31 pagesDiabetes Mellitus: WAHYUDI, S.Farm., AptMayesti FransiskaNo ratings yet
- Diabetes Mellitus3Document62 pagesDiabetes Mellitus3drmohinirajputNo ratings yet
- Diabetes Diabetes Diabetes: ClassificationDocument10 pagesDiabetes Diabetes Diabetes: ClassificationAjay Pal NattNo ratings yet
- Diabetes Mellitus 2021Document61 pagesDiabetes Mellitus 2021Andarge ImperialNo ratings yet
- Diabetes MellitusDocument24 pagesDiabetes MellitusIgwe SolomonNo ratings yet
- Diabetes MellitusDocument15 pagesDiabetes MellitusFathima RaihanNo ratings yet
- DM PresentationDocument28 pagesDM PresentationmymommywowNo ratings yet
- Ultimate Diet Plan for Diabetic Patients: Revolutionizing Diabetic NutritionFrom EverandUltimate Diet Plan for Diabetic Patients: Revolutionizing Diabetic NutritionNo ratings yet
- Instant Download Adrenal Disorders, 100 Cases From The Adrenal Clinic - Ebook PDF PDF All ChaptersDocument41 pagesInstant Download Adrenal Disorders, 100 Cases From The Adrenal Clinic - Ebook PDF PDF All Chapterslialkocarido100% (3)
- C.F.A.S. Hba1C: Value Sheet Ver.1 Cobas Integra 800 AnalyzerDocument8 pagesC.F.A.S. Hba1C: Value Sheet Ver.1 Cobas Integra 800 AnalyzertechlabNo ratings yet
- Blood Glucose MonitorDocument1 pageBlood Glucose MonitorCarolina TessandoriNo ratings yet
- Survey of Knowledge-Attitude-Practice (KAP) Concerning Insulin Use in Adult Diabetic Patients at A Tertiary Care HospitalDocument5 pagesSurvey of Knowledge-Attitude-Practice (KAP) Concerning Insulin Use in Adult Diabetic Patients at A Tertiary Care HospitalChandresh DumatarNo ratings yet
- HyperglycemiaDocument3 pagesHyperglycemiadaks89No ratings yet
- Penanganan Pasien Status Hiperglikemik Hiperosmoler Yang Disertai Pankreatitis AkutDocument6 pagesPenanganan Pasien Status Hiperglikemik Hiperosmoler Yang Disertai Pankreatitis AkutOvelin LarasatiNo ratings yet
- Thyroid FunctionDocument2 pagesThyroid FunctionSm Bikash Kumar MohonNo ratings yet
- FinalDocument1 pageFinallowkeyo4daitoNo ratings yet
- El Cateterismo Bilateral y Simultáneo de Los Senos Petrosos InferioresDocument8 pagesEl Cateterismo Bilateral y Simultáneo de Los Senos Petrosos InferioresPaoloNo ratings yet
- TRH Stimulation TestDocument3 pagesTRH Stimulation TestsakuraleeshaoranNo ratings yet
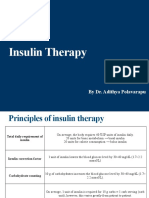
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- HbA1c To eAG v2Document15 pagesHbA1c To eAG v2Sudhir KumarNo ratings yet
- Unit 7 Diabetes Student ResourcesDocument7 pagesUnit 7 Diabetes Student ResourcesScribdNo ratings yet
- Standards of Care in Diabetes - 2024Document19 pagesStandards of Care in Diabetes - 2024ElizabethNo ratings yet
- Certificate of Analysis: Liaison Control Thyroid 3Document1 pageCertificate of Analysis: Liaison Control Thyroid 3Khaled AlkhawaldehNo ratings yet
- Dr. Muhammad Faiz Rasmi-24 PagesDocument37 pagesDr. Muhammad Faiz Rasmi-24 PagesNavine NalechamiNo ratings yet
- Kuliah HyperthyroidDocument18 pagesKuliah HyperthyroidFreddyNo ratings yet
- Diabetes MelitusDocument44 pagesDiabetes MelitusDwi Novianti SugihartiNo ratings yet
- TEMD - Diabetus Mellitus-2022Document324 pagesTEMD - Diabetus Mellitus-2022ali sağdıçNo ratings yet
- DSA 6 Adrenal13Document17 pagesDSA 6 Adrenal13Jason ShoreNo ratings yet
- Endocrine System: Capillary Glucose MonitoringDocument34 pagesEndocrine System: Capillary Glucose Monitoringjoel david knda mj100% (1)
- MCQ DentalDocument20 pagesMCQ DentalKovoor LedchumananNo ratings yet
- JBDS 01 Hypo Algorithm January 2023Document1 pageJBDS 01 Hypo Algorithm January 2023MUHAMMAD09No ratings yet
- Daftar Pustaka: Diabetes, Metabolic Syndrome, and Obesity: Targets and Therapy. 2011 3:49-53Document2 pagesDaftar Pustaka: Diabetes, Metabolic Syndrome, and Obesity: Targets and Therapy. 2011 3:49-53Dina Ikrama PutriNo ratings yet
- Hypothyroidism (Myxedema)Document25 pagesHypothyroidism (Myxedema)Arzo AnumNo ratings yet
- Diabetes Mellitus: Specialty Icd 10 Icd 9-Cm Medlineplus Emedicine Patient Uk MeshDocument2 pagesDiabetes Mellitus: Specialty Icd 10 Icd 9-Cm Medlineplus Emedicine Patient Uk MeshMidaSimamoraNo ratings yet
- Pre-Lecture Quiz Introduction To The Endocrine System True/FalseDocument4 pagesPre-Lecture Quiz Introduction To The Endocrine System True/FalseLovely LadyNo ratings yet
- Champa Debnath-30Document1 pageChampa Debnath-30Sanjoy DasNo ratings yet
- How To Identify Hypoglycaemia-Induced Hyperglycaemia (Somogyi Effect)Document3 pagesHow To Identify Hypoglycaemia-Induced Hyperglycaemia (Somogyi Effect)Onur BalNo ratings yet