Neonatal Cyanosis
Neonatal Cyanosis
Download as key, pdf, or txt
You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Hello Kids 1Document83 pagesHello Kids 1joaquitolindo100% (2)
- Serial Num Ber Name Mobile No. Email Current LocationDocument48 pagesSerial Num Ber Name Mobile No. Email Current LocationNishant Kumar0% (1)
- Integral Calculus Module 1 PDFDocument12 pagesIntegral Calculus Module 1 PDFRara JaveeeNo ratings yet
- Six Thinking HatsDocument26 pagesSix Thinking HatsFrank Calberg80% (5)
- Neonatal Central CyanosisDocument4 pagesNeonatal Central CyanosisRosdiana Elizabeth SiburianNo ratings yet
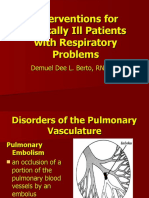
- Pulmonary EdemaDocument18 pagesPulmonary EdemaMohammed Taysier QudaihNo ratings yet
- Acute Heart FailureDocument9 pagesAcute Heart FailureChen Briones100% (1)
- CPCreportDocument3 pagesCPCreport楊力恆No ratings yet
- 2a Cardiology Saq QuestionsDocument7 pages2a Cardiology Saq Questionsnoahngoma41No ratings yet
- Ards AssignmentDocument13 pagesArds AssignmentANJALI NATHNo ratings yet
- Interventions For Critically Ill Patients With Respiratory Problems LectureDocument118 pagesInterventions For Critically Ill Patients With Respiratory Problems LecturedeebertoNo ratings yet
- Gerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistDocument51 pagesGerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistChristian Clyde N. ApigoNo ratings yet
- 8 Summary Major Chronic Illness of Older Adult Understanding The Pathophysiology and Nursing InterventionDocument21 pages8 Summary Major Chronic Illness of Older Adult Understanding The Pathophysiology and Nursing InterventionSteffiNo ratings yet
- CyanosisDocument58 pagesCyanosisCaroline Shira Deori100% (1)
- Gerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistDocument51 pagesGerry B. Acosta, MD, FPPS, FPCC: Pediatric CardiologistChristian Clyde N. ApigoNo ratings yet
- ARDSDocument23 pagesARDSDumora FatmaNo ratings yet
- Aproach To A Patient With CyanosisDocument18 pagesAproach To A Patient With CyanosisEsther AumaNo ratings yet
- Orthopedic: Complications of FracturesDocument11 pagesOrthopedic: Complications of FracturesDrAyyoub AbboodNo ratings yet
- Interventions For Critically Ill Patients With Respiratory Problems HandoutsDocument115 pagesInterventions For Critically Ill Patients With Respiratory Problems HandoutsDemuel Dee L. BertoNo ratings yet
- CardiacDocument43 pagesCardiacStephanie TalbotNo ratings yet
- Approach To A Child With Cyanosis GRP E FINALDocument37 pagesApproach To A Child With Cyanosis GRP E FINALdua.11864No ratings yet
- MEDICAL SURGICAL REVIEWER PrelimDocument34 pagesMEDICAL SURGICAL REVIEWER PrelimLUREY JAMES A. VACALARESNo ratings yet
- Cardiogenic Pulmonary Edema - StatPearls - NCBI BookshelfDocument14 pagesCardiogenic Pulmonary Edema - StatPearls - NCBI BookshelfalbacclNo ratings yet
- Pulmonary Thromboembolism: DR Olubunmi Ogunlade Consultant PulmonologistDocument34 pagesPulmonary Thromboembolism: DR Olubunmi Ogunlade Consultant PulmonologistEmeka Chinedu Precious PetrousNo ratings yet
- Congenital Heart DefectDocument12 pagesCongenital Heart Defectsangkularosmina837No ratings yet
- Pathophysiology CAP and HTNDocument5 pagesPathophysiology CAP and HTNLeonaPunzalanNo ratings yet
- Innocent Heart MurmursDocument10 pagesInnocent Heart Murmurslindsay_weiss_6No ratings yet
- Cardiac FailureDocument63 pagesCardiac FailureNina OaipNo ratings yet
- ShockDocument43 pagesShockAbdul Rahman Ghassan QasemNo ratings yet
- Angelito L. Ramos Jr. RN Clinical InstructorDocument68 pagesAngelito L. Ramos Jr. RN Clinical Instructorraymondblade18100% (17)
- Pulmonary EdemaDocument35 pagesPulmonary Edemawaqas_xsNo ratings yet
- Aortic StenosisDocument3 pagesAortic StenosisMaxine BaraquiaNo ratings yet
- Congestive Heart Failure: Dr. Asif WazirDocument21 pagesCongestive Heart Failure: Dr. Asif WazirHillary BushnellNo ratings yet
- Resp AlkalosisDocument4 pagesResp AlkalosisCas SanchezNo ratings yet
- Approach To Cyanotic Heart Disease Christopher Cheung Santokh Dhillon PDFDocument13 pagesApproach To Cyanotic Heart Disease Christopher Cheung Santokh Dhillon PDFsuckeydluffyNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Cardiopatias CianoticasDocument9 pagesCardiopatias CianoticasAngie CalderónNo ratings yet
- Pulmonary EdemaDocument2 pagesPulmonary EdemaMuhammad Bayu Zohari HutagalungNo ratings yet
- Congestive Heart FailureDocument19 pagesCongestive Heart FailureIlavenil PanduranganNo ratings yet
- Congestive Heart Failure in ChildrenDocument48 pagesCongestive Heart Failure in ChildrenSalman KhanNo ratings yet
- Safari 2 Ro9Document64 pagesSafari 2 Ro9عدنان المطرفيNo ratings yet
- Cardiac Tamponade Aortic DissectionDocument3 pagesCardiac Tamponade Aortic DissectionJhoeverly TebrioNo ratings yet
- LME SelfDocument5 pagesLME SelfJM Mizraime Gallo Dela-peñaNo ratings yet
- djdDocument15 pagesdjdMohammed SadoonNo ratings yet
- Cardio CHFDocument18 pagesCardio CHFHajime NakaegawaNo ratings yet
- Heart FailureDocument37 pagesHeart FailureNaveen KumarNo ratings yet
- Acute Respiratory FailureDocument8 pagesAcute Respiratory FailureCayunk NorlianaNo ratings yet
- Pulmonary Edema - StatPearls - NCBI BookshelfDocument6 pagesPulmonary Edema - StatPearls - NCBI BookshelfbanghirotadagantenkNo ratings yet
- Lesson No 3 Cardiac TamponadeDocument6 pagesLesson No 3 Cardiac TamponadeMary Grace GestiadaNo ratings yet
- Respiratory FailureDocument41 pagesRespiratory FailureM HNo ratings yet
- CARDIAC FAILURE NewDocument60 pagesCARDIAC FAILURE NewJake MillerNo ratings yet
- Capp&Dwe TomeldenfinalDocument74 pagesCapp&Dwe Tomeldenfinaltomeldenalyssa13No ratings yet
- Complications of FracturesDocument10 pagesComplications of FracturesalnuaimialoshNo ratings yet
- Acute Biologic Crisis-ArDocument71 pagesAcute Biologic Crisis-ArJayvee Novenario CasaljayNo ratings yet
- Acute Pulmonary EmbolismDocument82 pagesAcute Pulmonary Embolismincredible Prages100% (1)
- Chronic Obstructive Pulmonary Disease (COPD)Document32 pagesChronic Obstructive Pulmonary Disease (COPD)matrixtrinityNo ratings yet
- Diseases of The Respiratory SystemDocument42 pagesDiseases of The Respiratory SystemHassan DayaxNo ratings yet
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Alert Medical Series: USMLE Alert I, II, IIIFrom EverandAlert Medical Series: USMLE Alert I, II, IIIRating: 2 out of 5 stars2/5 (1)
- Congenital Heart Diseases, A Simple Guide to these Medical ConditionsFrom EverandCongenital Heart Diseases, A Simple Guide to these Medical ConditionsNo ratings yet
- Vsion NowlDocument2 pagesVsion NowlDaneel Olivaw100% (1)
- I Have A Dream - WestlifeDocument2 pagesI Have A Dream - WestlifeSARALA A/P S.K.SUBRAMANYAM MoeNo ratings yet
- Victimless Torts: Introduction To Law of Torts, B.B. PandeDocument8 pagesVictimless Torts: Introduction To Law of Torts, B.B. Pandechirali jainNo ratings yet
- Cloud Computing Security From Single To Mutli CloudsDocument80 pagesCloud Computing Security From Single To Mutli Cloudsppjadhav920No ratings yet
- Vocabulary Unit 3 2BACDocument1 pageVocabulary Unit 3 2BACSoufiane GourirranNo ratings yet
- FeversDocument2 pagesFeversMiranda Castro HomeopathyNo ratings yet
- Role of NGO in Protecting The EnvironmentDocument5 pagesRole of NGO in Protecting The Environmentlin_guardianangel100% (1)
- Yuk Ling Ong Vs Co 40-56Document2 pagesYuk Ling Ong Vs Co 40-56Theodore01760% (1)
- Notice: Ocean Transportation Intermediary Licenses: JMC Global, Et Al.Document2 pagesNotice: Ocean Transportation Intermediary Licenses: JMC Global, Et Al.Justia.comNo ratings yet
- COMP1649 Coursework Term1 - 2223Document7 pagesCOMP1649 Coursework Term1 - 2223Chembe MulabiNo ratings yet
- On Recurrence RelationDocument25 pagesOn Recurrence Relationreazaurrahman0786100% (1)
- Keta Port Request For Expression of InterestDocument4 pagesKeta Port Request For Expression of InterestHevie MichaelNo ratings yet
- Module 2 His003Document4 pagesModule 2 His003CARL JACOB MERCADONo ratings yet
- Gas Module 1 PDFDocument58 pagesGas Module 1 PDFHIEZEL BAYUGNo ratings yet
- GR 7 Term 3 2022 Psrip Efal Lesson PlanDocument260 pagesGR 7 Term 3 2022 Psrip Efal Lesson PlanlindyzindelaNo ratings yet
- LD3C 2 60W照度Document12 pagesLD3C 2 60W照度gorbytjokNo ratings yet
- Detail of LPG Marketing Companies Dated September 15 2022Document16 pagesDetail of LPG Marketing Companies Dated September 15 2022Irfan KhokharNo ratings yet
- Air Fryer Ranch Chicken WingsDocument2 pagesAir Fryer Ranch Chicken WingsUn OwenNo ratings yet
- How To Make PCB at Home-PcbwayDocument11 pagesHow To Make PCB at Home-PcbwayIced CoolzNo ratings yet
- Samsung ML-2160 Series PDDocument211 pagesSamsung ML-2160 Series PDAroma Aamir100% (1)
- Conditions For Learning Process of LearningDocument41 pagesConditions For Learning Process of LearningadindaNo ratings yet
- Getting Started With General Purpose Input/Output (Gpio) : View The Atmega4809 Code Examples On GithubDocument20 pagesGetting Started With General Purpose Input/Output (Gpio) : View The Atmega4809 Code Examples On GithubGion AndrásNo ratings yet
- Summative Test Week 1Document1 pageSummative Test Week 1Gladys Anne EspirituNo ratings yet
- NUS Coop Academic Dress Online OrderDocument1 pageNUS Coop Academic Dress Online OrderChristine ChowNo ratings yet
- Zero Trusted InfraDocument10 pagesZero Trusted InfraAmiraNo ratings yet
- TM 10-5411-239-13P CBC M105a2 Trailer, Type Iia1Document200 pagesTM 10-5411-239-13P CBC M105a2 Trailer, Type Iia1AdvocateNo ratings yet