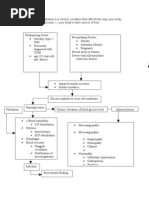
Pa Tho Physiology of Diabetes Mellitus
Pa Tho Physiology of Diabetes Mellitus
Download as docx, pdf, or txt
You might also like
- Concept Map Worksheet Mary Richards Heart Failure Jasgou1752Document3 pagesConcept Map Worksheet Mary Richards Heart Failure Jasgou1752Jasmyn Rose100% (1)
- Nephrotic Syndrome PathophysiologyDocument1 pageNephrotic Syndrome PathophysiologyKrisianne Mae Lorenzo FranciscoNo ratings yet
- Ap Psychology Multiple Choice QuestionsDocument9 pagesAp Psychology Multiple Choice Questionsapi-319829528No ratings yet
- Aphasia Treatment Goals and Targets-1Document16 pagesAphasia Treatment Goals and Targets-1Emily UlaNo ratings yet
- Pahtophysiology of EsrdDocument5 pagesPahtophysiology of EsrdCarl JardelezaNo ratings yet
- Pathophysiology of Heart FailureDocument4 pagesPathophysiology of Heart FailureTiger Knee100% (2)
- Aan 202 CourseworkDocument17 pagesAan 202 CourseworkCris GalendezNo ratings yet
- Metabolic EncephalopathyDocument26 pagesMetabolic Encephalopathywirdahaja100% (3)
- SY 2020-2021 Learning Area Week Grade Date Section Quarter Class Adviser Subject TeacherDocument4 pagesSY 2020-2021 Learning Area Week Grade Date Section Quarter Class Adviser Subject TeacherJanel Flores0% (1)
- Pa Tho PhysiologyDocument11 pagesPa Tho PhysiologyJonathan CuaNo ratings yet
- Endocrinology Notes for Medical StudentsFrom EverandEndocrinology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (1)
- Congestive Heart Failure PathophysiologyDocument16 pagesCongestive Heart Failure PathophysiologyDale LaurenteNo ratings yet
- Pathogenesis of Micro and Macrovascular Complications of DiabetesDocument4 pagesPathogenesis of Micro and Macrovascular Complications of DiabetesFrancesca LiNo ratings yet
- Liver CirrhosisDocument69 pagesLiver CirrhosisAhmed Alboun75% (4)
- Renal Case Study Final1Document41 pagesRenal Case Study Final1api-202881815100% (1)
- ESRD PathophysiologyDocument2 pagesESRD Pathophysiologynursing concept mapsNo ratings yet
- DM Case StudyDocument21 pagesDM Case StudyBern TolentinoNo ratings yet
- Diabetes Mellitus - Diabetic KetoacidosisDocument21 pagesDiabetes Mellitus - Diabetic KetoacidosisJamil Lorca100% (5)
- Liver Cirrhosis LectureDocument83 pagesLiver Cirrhosis LectureSheila Regina Tiza100% (1)
- General Pathophysiology: Predisposing Factors: Precipitating FactorsDocument2 pagesGeneral Pathophysiology: Predisposing Factors: Precipitating FactorsIrish Nicole DCNo ratings yet
- Diabetes PathoDocument2 pagesDiabetes Pathodrewcel100% (1)
- HCVDDocument5 pagesHCVDkhrizaleehNo ratings yet
- DkaDocument29 pagesDkaShadowSpectre0No ratings yet
- Liver Case StudyDocument6 pagesLiver Case StudyGhulam MustafaNo ratings yet
- Pathophysiology of AnginaDocument3 pagesPathophysiology of AnginaPhilip SimanganNo ratings yet
- Heart Failure With Preserved Ejection FractionDocument19 pagesHeart Failure With Preserved Ejection Fractioncosmin balanNo ratings yet
- Chronic Kidney Disease (CKD) - McMaster Pathophysiology ReviewDocument5 pagesChronic Kidney Disease (CKD) - McMaster Pathophysiology ReviewAnonymous uziTjed5j100% (1)
- Chronic Heart FailureDocument222 pagesChronic Heart FailureGustavo Meneo100% (1)
- Presentation Liver CirrhosisDocument26 pagesPresentation Liver CirrhosisFaye Dominique Roxas PalmaresNo ratings yet
- Chronic Kidney Disease Secondary To Type 2 Diabetes MellitusDocument84 pagesChronic Kidney Disease Secondary To Type 2 Diabetes Mellituswar5No ratings yet
- Chronic Renal FailureDocument37 pagesChronic Renal Failuredorkiebaby100% (10)
- Stroke and Cerebrovascular DiseaseDocument14 pagesStroke and Cerebrovascular DiseaseMarwan M.No ratings yet
- AnemiaDocument10 pagesAnemiaBia Payawal100% (2)
- Cerebral HemorrhageDocument10 pagesCerebral HemorrhageJayd Lorenz Vicente ChuanNo ratings yet
- Pathophysiology Diagram of Congestive Heart FailureDocument3 pagesPathophysiology Diagram of Congestive Heart FailureLeng Royo BrionesNo ratings yet
- Predisposing Conditions, Management and Prevention of Chronic Kidney DiseaseDocument52 pagesPredisposing Conditions, Management and Prevention of Chronic Kidney DiseaseSaad MotawéaNo ratings yet
- A Review: Nutrition in Chronic Kidney Disease PatientsDocument13 pagesA Review: Nutrition in Chronic Kidney Disease Patientsscience worldNo ratings yet
- Schematic Diagram: Signs and Symptoms: Headache, Unconsciousness, Nausea and Vomiting, Visual DisturbancesDocument3 pagesSchematic Diagram: Signs and Symptoms: Headache, Unconsciousness, Nausea and Vomiting, Visual DisturbancesJosett RomanoNo ratings yet
- Cerebrovascular AccidentDocument79 pagesCerebrovascular AccidentKathy B. AbuanNo ratings yet
- Case Study PPT Patho NLNGDocument36 pagesCase Study PPT Patho NLNGKate ChavezNo ratings yet
- Congestive Heart Failure PathophysiologyDocument7 pagesCongestive Heart Failure PathophysiologyAileen Grace RodrigoNo ratings yet
- Pathophysiology HPN CvaDocument1 pagePathophysiology HPN Cvatresdos09No ratings yet
- CAD PathoDocument3 pagesCAD PathoMark Anthony YabresNo ratings yet
- Hypertensive Cardiovascular DiseaseDocument16 pagesHypertensive Cardiovascular DiseaseTintin Ponciano100% (1)
- MNT For Liver DiseaseDocument44 pagesMNT For Liver Diseasemedikasudirman118100% (4)
- Chronic Kidney DiseaseDocument33 pagesChronic Kidney DiseasesexiiimammaNo ratings yet
- Acute Liver Failure in Adults: Etiology, Clinical Manifestations, and Diagnosis - UpToDateDocument14 pagesAcute Liver Failure in Adults: Etiology, Clinical Manifestations, and Diagnosis - UpToDateIatros GarciniNo ratings yet
- Sepsis Is The Consequence of A Dysregulated Inflammatory Response To An Infectious InsultDocument11 pagesSepsis Is The Consequence of A Dysregulated Inflammatory Response To An Infectious InsultShrests SinhaNo ratings yet
- Case Study NSTEMIDocument35 pagesCase Study NSTEMInikaaraaaNo ratings yet
- Alcoholic Hepatitis: Ekaterine Labadze MDDocument18 pagesAlcoholic Hepatitis: Ekaterine Labadze MDsushant jainNo ratings yet
- 25 Cardiovascular DiseaseDocument35 pages25 Cardiovascular DiseaseBramantyo NugrosNo ratings yet
- Pathophysiology ErDocument3 pagesPathophysiology ErAlexa A. AldayNo ratings yet
- CellulitisDocument12 pagesCellulitisAlma Bertos-Agub100% (1)
- Congestive Heart FailureDocument28 pagesCongestive Heart Failuresarguss1480% (5)
- Case Presentation On Chronic Kidney Disease1Document18 pagesCase Presentation On Chronic Kidney Disease1d100% (1)
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Hypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Diabetic Ketoacidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Ketoacidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pulmonary Arterial Hypertension in Congenital Heart Disease: Eisenmenger’s Syndrome - A Global PerspectiveFrom EverandPulmonary Arterial Hypertension in Congenital Heart Disease: Eisenmenger’s Syndrome - A Global PerspectiveNo ratings yet
- Vasculitis Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandVasculitis Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Data/Cues Diagnosis Scientific Rationale Planning Implementation RationaleDocument6 pagesData/Cues Diagnosis Scientific Rationale Planning Implementation RationalePong's Teodoro SalvadorNo ratings yet
- Pa Tho Physiology of Primary ComplexDocument1 pagePa Tho Physiology of Primary ComplexPong's Teodoro SalvadorNo ratings yet
- Pa Tho Physiology of Primary ComplexDocument1 pagePa Tho Physiology of Primary ComplexPong's Teodoro SalvadorNo ratings yet
- STI College of Nursing Sta. Cruz, Laguna College of Nursing: Submitted To: Mrs. Aurea Celino, RN Clinical InstructorDocument41 pagesSTI College of Nursing Sta. Cruz, Laguna College of Nursing: Submitted To: Mrs. Aurea Celino, RN Clinical InstructorPong's Teodoro SalvadorNo ratings yet
- Preterm PathoDocument1 pagePreterm PathoPong's Teodoro SalvadorNo ratings yet
- Congestive Heart Failure - PathophysiologyDocument1 pageCongestive Heart Failure - PathophysiologyPong's Teodoro SalvadorNo ratings yet
- Pa Tho Physiology of Primary ComplexDocument1 pagePa Tho Physiology of Primary ComplexPong's Teodoro SalvadorNo ratings yet
- Pa Tho Physiology of Broncho PneumoniaDocument1 pagePa Tho Physiology of Broncho PneumoniaPong's Teodoro SalvadorNo ratings yet
- Basic Occupational Safety and Health: Prepared By: Engr. Orik Niko SantosDocument79 pagesBasic Occupational Safety and Health: Prepared By: Engr. Orik Niko SantosNICE ONE100% (1)
- Abnormal Psychology Mock Boards - WIth AnswersDocument47 pagesAbnormal Psychology Mock Boards - WIth AnswersEunicaSelrabNo ratings yet
- Role PlayDocument8 pagesRole Playmjtan730No ratings yet
- Fdocuments - in - Lesson Plan Avaids Nursing EducationDocument9 pagesFdocuments - in - Lesson Plan Avaids Nursing Educationjuliya ShNo ratings yet
- ComEngpdf MergedDocument29 pagesComEngpdf MergedSujan ShresthaNo ratings yet
- Introduction To Market Access For Pharmaceuticals 1st Edition Mondher Toumi (Editor) Download PDFDocument52 pagesIntroduction To Market Access For Pharmaceuticals 1st Edition Mondher Toumi (Editor) Download PDFchayladanchi100% (3)
- Program of The: Online Conference &Document39 pagesProgram of The: Online Conference &Iulian ApostuNo ratings yet
- Modul.eng.Practice.new Sts'.Sep.2024Document31 pagesModul.eng.Practice.new Sts'.Sep.2024KiplyNo ratings yet
- Unit-2: Rural Development Programmes: Prepared By: Ankur Sachdeva Assistant Professor, MEDocument36 pagesUnit-2: Rural Development Programmes: Prepared By: Ankur Sachdeva Assistant Professor, MEAnupriyaNo ratings yet
- Entrepreneurship and The Entrepreneurial Mind-Set: Hisrich Peters ShepherdDocument19 pagesEntrepreneurship and The Entrepreneurial Mind-Set: Hisrich Peters ShepherdAwab HamidNo ratings yet
- ASD in PregnancyDocument15 pagesASD in PregnancyAiman ArifinNo ratings yet
- FDA-3537 Stat Sec Ext 01-04-23Document10 pagesFDA-3537 Stat Sec Ext 01-04-23Erick BellidoNo ratings yet
- La Grange Issues With 30 S. La Grange RoadDocument61 pagesLa Grange Issues With 30 S. La Grange RoadDavid GiulianiNo ratings yet
- Research Presentation BasherDanielaDocument13 pagesResearch Presentation BasherDanielaJerome PomentoNo ratings yet
- Infinite Jest in BriefDocument49 pagesInfinite Jest in Briefwilliamsmith1404No ratings yet
- Stasha Andrews-Teacher-Pdp-2019-End of YearDocument5 pagesStasha Andrews-Teacher-Pdp-2019-End of Yearapi-424238197No ratings yet
- Acute Pain Related To Inflammation and Distension of The Colon.Document2 pagesAcute Pain Related To Inflammation and Distension of The Colon.JULIANNE BAYHONNo ratings yet
- NMT 04209 - Basic Pharmacology-1Document126 pagesNMT 04209 - Basic Pharmacology-1Rubeni VENANSI chisiNo ratings yet
- CHN 2Document14 pagesCHN 2Aira PayadNo ratings yet
- Sample Protest Art WriteupDocument2 pagesSample Protest Art Writeupapi-266674779No ratings yet
- CV Buti Azfiani AzhaliDocument3 pagesCV Buti Azfiani AzhaliRANO KURNIADINo ratings yet
- En Stomach Cancer Guide For PatientsDocument51 pagesEn Stomach Cancer Guide For Patientsmanuaf2000No ratings yet
- UG LR-09 Critical ReasoningDocument25 pagesUG LR-09 Critical ReasoningdextuNo ratings yet
- Chuck Sipes Super SeminarDocument47 pagesChuck Sipes Super SeminarWarhammer13100% (9)
- Thesis On Veterinary HospitalDocument8 pagesThesis On Veterinary Hospitalbk156rhq100% (2)
- Full Option Yoga Free eBookDocument35 pagesFull Option Yoga Free eBooklauraparejaextremeraNo ratings yet
- Body Image BrochureDocument2 pagesBody Image Brochureden_a100% (1)