NCP Loss of Appetite
NCP Loss of Appetite
Download as docx, pdf, or txt
You might also like
- Nursing Care Plan For PostpartumDocument5 pagesNursing Care Plan For PostpartumTheeya Quigao91% (11)
- Nursing Care Plan: Risk For Disuse SyndromeDocument2 pagesNursing Care Plan: Risk For Disuse SyndromeRozsy FakhrurNo ratings yet
- As Fluid Volume Deficit (FVD), Hypovolemia) Is ADocument2 pagesAs Fluid Volume Deficit (FVD), Hypovolemia) Is ATanya Alyssa Untalan AquinoNo ratings yet
- NCP - Altered ComfortDocument2 pagesNCP - Altered ComfortJhudiel Gabriel Go0% (1)
- Adhf NCPDocument3 pagesAdhf NCPkristine keen buanNo ratings yet
- Risk For Deficient Fluid Volume Best NCPDocument2 pagesRisk For Deficient Fluid Volume Best NCPAlbean DelojeroNo ratings yet
- Disturbed Body ImageDocument3 pagesDisturbed Body Imagenura100% (1)
- Generic Name: Acetaminophen Brand Name: Tylenol: ActionDocument22 pagesGeneric Name: Acetaminophen Brand Name: Tylenol: Actionp_dawg100% (14)
- Eriopon R Liq. MSDSDocument10 pagesEriopon R Liq. MSDSraju_hosssenNo ratings yet
- NCP 1Document1 pageNCP 1hsiriaNo ratings yet
- Fluid Volume DeficitDocument3 pagesFluid Volume Deficitprickybiik100% (1)
- NCP Liver CirrhosisDocument7 pagesNCP Liver CirrhosisIris Jimenez-BuanNo ratings yet
- NCP Impaired SkinDocument2 pagesNCP Impaired Skinarjay2306_obcq100% (1)
- Altered Renal Perfusion CRFDocument4 pagesAltered Renal Perfusion CRFKristel Anne Nillo ZepolNo ratings yet
- n320 Peds NCP wk3Document2 pagesn320 Peds NCP wk3api-301826049No ratings yet
- Imbalanced Nutrition Less Than Body Requirements Diabetes NCP PDFDocument5 pagesImbalanced Nutrition Less Than Body Requirements Diabetes NCP PDFashamy acolNo ratings yet
- NCP Imbalanced NutritionDocument3 pagesNCP Imbalanced NutritionAav Canlas100% (1)
- NCP Imbalanced Nutrition Less Than Body RequirementsDocument5 pagesNCP Imbalanced Nutrition Less Than Body Requirementsrusnani100% (1)
- NCPDocument6 pagesNCPKyla Carbonel100% (2)
- NCP For UtiDocument3 pagesNCP For UtiAaron Sanchez100% (1)
- Nursing Care PlanDocument2 pagesNursing Care PlanAldrein GonzalesNo ratings yet
- Nursing Care Plans: Assessment Nursing Diagnosis Planning Implementation Rationale EvaluationDocument2 pagesNursing Care Plans: Assessment Nursing Diagnosis Planning Implementation Rationale EvaluationRheeanne Mae Amilasan100% (1)
- NCP For HemorrhoidsDocument3 pagesNCP For HemorrhoidsTADURAN RENE MAE ANGELLI F.No ratings yet
- NCPDocument2 pagesNCPkatrina_velasco_1No ratings yet
- NCP HyperthermiaDocument6 pagesNCP HyperthermiaGrax DeeNo ratings yet
- NCPDocument1 pageNCPJ. ishtelleNo ratings yet
- NCP For SVTDocument6 pagesNCP For SVTRen VillenaNo ratings yet
- Deficient Fluid Volume (AGEDocument2 pagesDeficient Fluid Volume (AGENursesLabs.com83% (6)
- Llacer FdarDocument2 pagesLlacer FdarRaidis PangilinanNo ratings yet
- NCP LymphomaDocument3 pagesNCP LymphomaJohn Emmanuel Tatad TudNo ratings yet
- NCP - Risk Impaired Skin RT Altered Circulation (Spinal Injury)Document2 pagesNCP - Risk Impaired Skin RT Altered Circulation (Spinal Injury)yanny0350% (2)
- Nursing Care PlanDocument4 pagesNursing Care PlanKath RubioNo ratings yet
- NCP Arra AnemiaDocument2 pagesNCP Arra AnemiaShin GuevaraNo ratings yet
- Short Term: Independent: Independent: Short TermDocument2 pagesShort Term: Independent: Independent: Short TermAndre ImperialNo ratings yet
- NCP GastroenteritisDocument1 pageNCP GastroenteritisFranchesca PaunganNo ratings yet
- Altered Bowel EliminationDocument1 pageAltered Bowel EliminationneoclintNo ratings yet
- NCP HemothoraxDocument3 pagesNCP Hemothoraxroseonabreeze0% (2)
- NCP For DM1Document2 pagesNCP For DM1Pau Hipol Madriaga100% (1)
- Final NCP LeptospirosisDocument6 pagesFinal NCP LeptospirosisKeith Austin100% (1)
- Assessment Objectives: "Masakit Lagi Yung Lalamunan NyaDocument3 pagesAssessment Objectives: "Masakit Lagi Yung Lalamunan Nyaangel_pearl413100% (2)
- Electrolyte Imbalance NCPDocument8 pagesElectrolyte Imbalance NCPManuel Jacob YradNo ratings yet
- NCP Delayed Wound RecoveryDocument5 pagesNCP Delayed Wound RecoveryDarkCeades100% (2)
- Liver Cirrhosis NCP 1Document6 pagesLiver Cirrhosis NCP 1Paolo Rafael D EsguerraNo ratings yet
- NCP Fluid Volume DeficitDocument3 pagesNCP Fluid Volume DeficitNecheal BaayNo ratings yet
- NCP UtiDocument1 pageNCP Utitsunami_cutieNo ratings yet
- NCP of MGH PatientDocument2 pagesNCP of MGH PatientMaverick LimNo ratings yet
- Liver Cirrhosis NCPDocument3 pagesLiver Cirrhosis NCPSharmaine MadlaNo ratings yet
- NCP HypokalemiaDocument2 pagesNCP HypokalemiaJoyVee Pillagara-De Leon40% (5)
- Nursing Care Plan HyperthermiaDocument1 pageNursing Care Plan Hyperthermiasamanthabox50% (2)
- NCP - Altered Tissue PerfusionDocument2 pagesNCP - Altered Tissue PerfusionLeigh Kristel Andrion0% (1)
- Fluid Volume DeficitDocument1 pageFluid Volume DeficitventimiglionNo ratings yet
- NCPDocument2 pagesNCPHippocrates Impressionist CostalesNo ratings yet
- N C P For Perioperative Pts.Document4 pagesN C P For Perioperative Pts.Daisy Palisoc100% (2)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationVecky TolentinoNo ratings yet
- NCP: Acute GastroenteritisDocument3 pagesNCP: Acute GastroenteritishauteanicoleNo ratings yet
- Assessment Explanation of The Problem Objective Nursing Intervention Rationale Evaluation Sto: StoDocument7 pagesAssessment Explanation of The Problem Objective Nursing Intervention Rationale Evaluation Sto: StoclarheenaNo ratings yet
- Nursing Care PlanDocument23 pagesNursing Care PlanLorielle HernandezNo ratings yet
- NCP Icu-CcuDocument6 pagesNCP Icu-CcuJohn CenasNo ratings yet
- Wa0000.Document34 pagesWa0000.Abdelrahman AbdouNo ratings yet
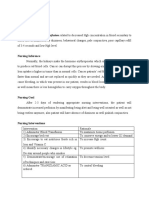
- Ineffective Tissue Perfusion Related To Decreased HGB Concentration in Blood Secondary ToDocument6 pagesIneffective Tissue Perfusion Related To Decreased HGB Concentration in Blood Secondary Toericke_tanNo ratings yet
- "May Mga Sugat Ako.": As Verbalized by The PatientDocument6 pages"May Mga Sugat Ako.": As Verbalized by The Patientedifier_moonNo ratings yet
- Example of Risk Dignosis ,Plan and Intervention (1)Document5 pagesExample of Risk Dignosis ,Plan and Intervention (1)sisay tolosaNo ratings yet
- Leprosy CHN ReportDocument3 pagesLeprosy CHN Reportmaglangitjoannamarie1920No ratings yet
- SDS RK Motorcycle Chain Cleaner - 290720206871Document5 pagesSDS RK Motorcycle Chain Cleaner - 290720206871ListonNo ratings yet
- Activity 1 DRRRDocument2 pagesActivity 1 DRRRFried ChickenNo ratings yet
- Human Capital FormationDocument45 pagesHuman Capital Formationhusaina.badshah17No ratings yet
- FaoDocument2 pagesFaoPhanuel AgbyphNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument15 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationShermayne Mallapre HernandezNo ratings yet
- Days Times Monday Tuesday Wednesday Thursday FridayDocument1 pageDays Times Monday Tuesday Wednesday Thursday FridayChala DabalaNo ratings yet
- Module 4Document29 pagesModule 4ibrahimNo ratings yet
- START and STOPP CriteriaDocument3 pagesSTART and STOPP CriteriasfintokyoNo ratings yet
- Drug-Facilitated Sexual Assault and Other CrimesDocument15 pagesDrug-Facilitated Sexual Assault and Other CrimesManoloGarridoNo ratings yet
- KPI Metro PerformanceDocument28 pagesKPI Metro Performancefelipeo83100% (1)
- Sawdust MSDSDocument4 pagesSawdust MSDSDandika RamdhanNo ratings yet
- 2023 NYS State of The State BookDocument277 pages2023 NYS State of The State BookCarl AldingerNo ratings yet
- Evonik Whitepaper Eudracap Select Examining A Case From Development To Clinical TrialDocument13 pagesEvonik Whitepaper Eudracap Select Examining A Case From Development To Clinical TrialrattychattyNo ratings yet
- AHS BOOT Health Department KEMUDocument10 pagesAHS BOOT Health Department KEMUTariq ManzoorNo ratings yet
- Note MakingDocument7 pagesNote MakingffyyhafxqefqobhaswNo ratings yet
- PsychoEducation Mental Illness. 1Document13 pagesPsychoEducation Mental Illness. 1Sathyanarayanan MarimuthuNo ratings yet
- Ethics Final CoverageDocument36 pagesEthics Final CoverageRoger Yatan Ibañez Jr.No ratings yet
- TheEconomist 2023 04 08Document338 pagesTheEconomist 2023 04 08xuanzhou willNo ratings yet
- Identifying Triggers Worksheet & ExampleDocument10 pagesIdentifying Triggers Worksheet & ExampleДоникаNo ratings yet
- Gwamaka SamsonDocument73 pagesGwamaka SamsonSaami MalikNo ratings yet
- REVISED Personal Financial Wellness of Grade 12 Accountancy Business and Management LICEO Students 4Document82 pagesREVISED Personal Financial Wellness of Grade 12 Accountancy Business and Management LICEO Students 4Rae SlaughterNo ratings yet
- Ting Frost Uhr (2021) Working With Separated FamiliesDocument6 pagesTing Frost Uhr (2021) Working With Separated Families7sunqiiNo ratings yet
- Ghee Saturated Fat: Fat in Ghee Is A Known Fact: But How It Is Heart FriendlyDocument5 pagesGhee Saturated Fat: Fat in Ghee Is A Known Fact: But How It Is Heart FriendlybubuNo ratings yet
- InsideBE Nudgestock Ebook CompressedDocument28 pagesInsideBE Nudgestock Ebook Compressedunreal2No ratings yet
- Acute Lymphoblastic Leukemia Characterizationandits Prognostic ValuesDocument11 pagesAcute Lymphoblastic Leukemia Characterizationandits Prognostic ValuesDebby ApriliaNo ratings yet
- Quit Smoking GuideDocument2 pagesQuit Smoking GuideJayson AguilarNo ratings yet
- Guide-Preventing Diaper Rashes 21Jan2014FNL en PDFDocument5 pagesGuide-Preventing Diaper Rashes 21Jan2014FNL en PDFLina Mahayaty SembiringNo ratings yet