Entamoeba Histoytica
Entamoeba Histoytica
Download as pptx, pdf, or txt
You might also like
- Parasitology MCQ 2Document18 pagesParasitology MCQ 2Adams Zarawu100% (3)
- Cerebro Review Center Parasitology Lecture Notes FINALDocument53 pagesCerebro Review Center Parasitology Lecture Notes FINALqnx6696m7fNo ratings yet
- Animal Behavior Study GuideDocument6 pagesAnimal Behavior Study Guideapi-595420397No ratings yet
- Phylum PoriferaDocument30 pagesPhylum PoriferaEloisa Lopez100% (2)
- Class 9 Biology Chapter 16 Diseases Causes and ControlDocument6 pagesClass 9 Biology Chapter 16 Diseases Causes and ControlwanroyNo ratings yet
- Electronic Atlas of ParasitologyDocument650 pagesElectronic Atlas of Parasitologystormyccs100% (7)
- 2009 Parasitology MCQsDocument12 pages2009 Parasitology MCQsfilchibuff89% (9)
- Parasitology NotesDocument3 pagesParasitology NotesMyrielle Trisha SAYRENo ratings yet
- 2021 Chapter 6 Tissue Most IMP QuestionsDocument11 pages2021 Chapter 6 Tissue Most IMP QuestionsGauravNo ratings yet
- A Larval PR Oject On Ar ThropodaDocument15 pagesA Larval PR Oject On Ar ThropodaShambadip SenNo ratings yet
- Lec4 SocialInsects TheSociety NotesDocument3 pagesLec4 SocialInsects TheSociety NotesAlexandra LvNo ratings yet
- Dr. Archana Rani Associate Professor Department of Anatomy KGMU UP, LucknowDocument44 pagesDr. Archana Rani Associate Professor Department of Anatomy KGMU UP, LucknowlailaNo ratings yet
- Entamoeba HistolyticaDocument18 pagesEntamoeba HistolyticaMayuri VohraNo ratings yet
- Phylum NematodaDocument24 pagesPhylum NematodaKaten KyoukotsuNo ratings yet
- Connective TissueDocument33 pagesConnective Tissue20227730 PRACHI TOMAR100% (1)
- Compound EyeDocument5 pagesCompound EyeWael ElwekelNo ratings yet
- Ocular AnatomyDocument96 pagesOcular AnatomyKawtar VetoamiNo ratings yet
- Medical Entomolgy ContdDocument25 pagesMedical Entomolgy Contdsham147No ratings yet
- M - 23 Polytene ChromosomeDocument3 pagesM - 23 Polytene ChromosomeDr. Tapan Kr. DuttaNo ratings yet
- Evolution of MetamerismDocument3 pagesEvolution of MetamerismBs JanNo ratings yet
- General Protocol For Isolation of DNADocument15 pagesGeneral Protocol For Isolation of DNAS291991No ratings yet
- Fasciola HepaticaDocument38 pagesFasciola HepaticaDeni Susanto100% (1)
- General Characters & Classification: Dr. P. Ravi SekharDocument33 pagesGeneral Characters & Classification: Dr. P. Ravi Sekharneeru.bhagatNo ratings yet
- Accessory Respiratory Organ-FishDocument63 pagesAccessory Respiratory Organ-Fishkaushik mallickNo ratings yet
- Respiratory System: StructureDocument29 pagesRespiratory System: StructureDr. Abir Ishtiaq100% (1)
- AMOEBADocument74 pagesAMOEBAhuyenthanh1807100% (1)
- 01 Introduction To HistologyDocument60 pages01 Introduction To HistologyMartha Orendu Oche AttahNo ratings yet
- Crustaceae Larval Forms PDFDocument12 pagesCrustaceae Larval Forms PDFAfridi ShaikhNo ratings yet
- Insect Reproduction: Entomology (BIOL 409) Fall 2004, Lecture # 21Document18 pagesInsect Reproduction: Entomology (BIOL 409) Fall 2004, Lecture # 21Reube RonnyNo ratings yet
- 06 GastrulationtxtDocument38 pages06 GastrulationtxtHafidzul HalimNo ratings yet
- Acoelomate Bilateral AnimalsDocument31 pagesAcoelomate Bilateral AnimalsHirendra GurnaniNo ratings yet
- HookwormDocument9 pagesHookwormfadilah mutiaNo ratings yet
- Characteristics of Phylum Porifera (Sponges)Document15 pagesCharacteristics of Phylum Porifera (Sponges)Pralex PrajapatiNo ratings yet
- Sericulture, Silkworm Diseases and PestsDocument28 pagesSericulture, Silkworm Diseases and Pestskapil agrawalNo ratings yet
- Techniques For Parasite Assays and Identification in Faecal SamplesDocument15 pagesTechniques For Parasite Assays and Identification in Faecal SamplesSuresh Kumar Ramanathan50% (2)
- Drosophila MelanogasterDocument13 pagesDrosophila MelanogasterDavid MorganNo ratings yet
- Microbiology Blue Print Short AnswersDocument14 pagesMicrobiology Blue Print Short AnswersSpyop LoverNo ratings yet
- Third Week of DevelopmentDocument34 pagesThird Week of DevelopmentAriba Asif100% (1)
- Prepared By: Shella Mae N. Mainit MSF-1Document44 pagesPrepared By: Shella Mae N. Mainit MSF-1Chriseil arts tancioNo ratings yet
- (Advances in Parasitology 76) Louis M. Weiss and Herbert B. Tanowitz (Eds.) - Chagas Disease, Part B-Academic Press, Elsevier (2011)Document283 pages(Advances in Parasitology 76) Louis M. Weiss and Herbert B. Tanowitz (Eds.) - Chagas Disease, Part B-Academic Press, Elsevier (2011)Stoian GoranovNo ratings yet
- Excretion in InsectsDocument58 pagesExcretion in InsectsMani VasagamNo ratings yet
- Describe The Taxonomical of Identification of Cultivable FishesDocument5 pagesDescribe The Taxonomical of Identification of Cultivable FishesNarasimha MurthyNo ratings yet
- Cnidaria: Body Cavity Known As The CoelenteronDocument21 pagesCnidaria: Body Cavity Known As The CoelenteronLakshya GuptaNo ratings yet
- Rickettsia: Introduction, Characteristics, ClassificationDocument5 pagesRickettsia: Introduction, Characteristics, ClassificationMohammed ShahanewzNo ratings yet
- Chapter 9 Diversity Among AnimalsDocument9 pagesChapter 9 Diversity Among Animalssaeeda shoaibNo ratings yet
- Amphibia-Parental CareDocument4 pagesAmphibia-Parental CareAakash VNo ratings yet
- AnimaldistributioniiiDocument22 pagesAnimaldistributioniiiManoo BiliNo ratings yet
- BlastulaDocument4 pagesBlastulaCyanDesNo ratings yet
- Ethology bookDocument20 pagesEthology bookpriyanigoyal07100% (1)
- TS of Mammalian Spleen, Thymus and Lymph NodesDocument5 pagesTS of Mammalian Spleen, Thymus and Lymph Nodesvijaykumarrabidas1033No ratings yet
- Lab Report Cell Bio MitosisDocument4 pagesLab Report Cell Bio Mitosisain syukriahNo ratings yet
- Snakes Biting MechanismDocument7 pagesSnakes Biting Mechanismnancy sharmaNo ratings yet
- Gastropods - Nervous SystemDocument9 pagesGastropods - Nervous SystemKim Esperas SitchonNo ratings yet
- 5 - TrematodesDocument14 pages5 - TrematodesEsther Victoria TolentinoNo ratings yet
- Theories Of: EvolutionDocument13 pagesTheories Of: EvolutionLorenz Dadis AlonosNo ratings yet
- Evolution of Urogenital Ducts Part-2 27.03.2020Document10 pagesEvolution of Urogenital Ducts Part-2 27.03.2020Sonali SahooNo ratings yet
- RNA Plant and Animal Virus Replication PDFDocument9 pagesRNA Plant and Animal Virus Replication PDFmanoj_rkl_07No ratings yet
- The Life Cycle of A Horsehair Worm, Gordius: Robustus (Nematomorpha: Gordioidea)Document4 pagesThe Life Cycle of A Horsehair Worm, Gordius: Robustus (Nematomorpha: Gordioidea)Aisya KhoirunnisaNo ratings yet
- Phylum CnidariaDocument26 pagesPhylum CnidariaAbby SangualNo ratings yet
- Protozoa 1Document46 pagesProtozoa 1Muhammad Abu HurairaNo ratings yet
- Monocystis AgilisDocument16 pagesMonocystis AgilisRavi JaiswalNo ratings yet
- Cestoda and TrematodaDocument42 pagesCestoda and Trematodadeneke100% (1)
- Pathology for Toxicologists: Principles and Practices of Laboratory Animal Pathology for Study PersonnelFrom EverandPathology for Toxicologists: Principles and Practices of Laboratory Animal Pathology for Study PersonnelElizabeth McInnesNo ratings yet
- Micropara Group 4Document40 pagesMicropara Group 4Juliana MendozaNo ratings yet
- Infectious DiseasesDocument96 pagesInfectious DiseasesSuvasish SuvasishNo ratings yet
- Chapter 15 - Hygiene - (A Key To Healthy Life) - Solutions For Class 9 ICSE Concise Biology Selina - KnowledgeBoatDocument8 pagesChapter 15 - Hygiene - (A Key To Healthy Life) - Solutions For Class 9 ICSE Concise Biology Selina - KnowledgeBoatCool BrosNo ratings yet
- Biology G12 Vol1 2023Document160 pagesBiology G12 Vol1 2023thyadiadarsh8113No ratings yet
- University QN Paper 1990 To 2015Document41 pagesUniversity QN Paper 1990 To 2015Ganesh NatarajanNo ratings yet
- Para Midterm ExamDocument10 pagesPara Midterm ExamKlenn Orteza100% (2)
- DysenteryDocument7 pagesDysenterymukulpjrNo ratings yet
- Study: Disease Causing OrganismsDocument1 pageStudy: Disease Causing OrganismsSayandeep DuttaNo ratings yet
- Parasitology ReviewerDocument15 pagesParasitology ReviewerMariel Angelie TuringanNo ratings yet
- Soln DPP 05 Human Health and DiseaseDocument27 pagesSoln DPP 05 Human Health and DiseaseAkshat RastogiNo ratings yet
- Disentri AmoebaDocument9 pagesDisentri Amoebagabb jeeNo ratings yet
- Entamoeba HistolyticaDocument6 pagesEntamoeba HistolyticaWan Nur AnisaNo ratings yet
- Entamoeba HistolyticaDocument16 pagesEntamoeba Histolyticaشموخي عزتيNo ratings yet
- Amaebiasis / Manyoka Aneraza / IsiqathoDocument138 pagesAmaebiasis / Manyoka Aneraza / Isiqatholex tecNo ratings yet
- NCMB 312 Lect Final NotesDocument16 pagesNCMB 312 Lect Final NotesAngie BaylonNo ratings yet
- Lect 04Document16 pagesLect 04brahimodz29No ratings yet
- Lifecycle of EntamoebaDocument86 pagesLifecycle of EntamoebaAman ShaikNo ratings yet
- Laboratory Activity 3: Filamer Christian University Microbiology and Parasitology Laboratory ActivityDocument3 pagesLaboratory Activity 3: Filamer Christian University Microbiology and Parasitology Laboratory Activitykaren joy delgadoNo ratings yet
- Prof Parasitology by HON. UKPOR IYANG IYANGDocument3 pagesProf Parasitology by HON. UKPOR IYANG IYANGokikiolaNo ratings yet
- MTAP Parasitology Notes FILLED OUTDocument29 pagesMTAP Parasitology Notes FILLED OUT5yhxy7tkt4No ratings yet
- Biology Project: Topic: Human Health and DiseasesDocument17 pagesBiology Project: Topic: Human Health and DiseasesSagar Kumar0% (1)
- SEM1 ParasitologyDocument34 pagesSEM1 Parasitologybella xiaoNo ratings yet
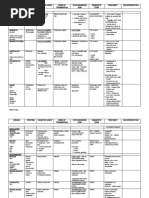
- Disease Synoynm Causative Agent Mode of Transmission Pathognomonic Sign Diagnostic Exam Treatment NSG InterventionDocument5 pagesDisease Synoynm Causative Agent Mode of Transmission Pathognomonic Sign Diagnostic Exam Treatment NSG InterventionhydsNo ratings yet
- Red Book PDFDocument898 pagesRed Book PDFHenry BarberenaNo ratings yet
- Entamoeba HistolyticaDocument15 pagesEntamoeba HistolyticaErnesto De SagoNo ratings yet