CVS Examination Edited
CVS Examination Edited
Download as ppt, pdf, or txt
You might also like
- A Practical Guide To Kinesiology Taping For Injury Prevention and Common Medical Conditions (John Gibbons) (Z-Library)Document105 pagesA Practical Guide To Kinesiology Taping For Injury Prevention and Common Medical Conditions (John Gibbons) (Z-Library)alejuan252100% (1)
- Fletcher Bolter Op ManualDocument56 pagesFletcher Bolter Op Manualbannet100% (1)
- MACRAME Project PlanDocument5 pagesMACRAME Project PlanIvy Talisic100% (1)
- Abnormal Heart Sounds: First Heart Sound (S)Document4 pagesAbnormal Heart Sounds: First Heart Sound (S)Faris Mufid MadyaputraNo ratings yet
- Approach To Cardiac MurmursDocument11 pagesApproach To Cardiac Murmurstouthang0074085No ratings yet
- 7th Heart Sounds and MurmursDocument6 pages7th Heart Sounds and MurmursbabibubeboNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Clinical SignsDocument26 pagesClinical SignswiraandiniNo ratings yet
- GI Exam (RCT)Document6 pagesGI Exam (RCT)kenners100% (11)
- Heart Sounds: Mitral Regurgitation Congestive Heart FailureDocument6 pagesHeart Sounds: Mitral Regurgitation Congestive Heart FailurecindyNo ratings yet
- 4 Abdominal+ExaminationDocument9 pages4 Abdominal+Examinationمرتضى حسين عبدNo ratings yet
- Pons MedullaDocument32 pagesPons MedullaEnaWahahaNo ratings yet
- Examination of Cardiovascular SystemDocument24 pagesExamination of Cardiovascular SystemThilak JayalathNo ratings yet
- Lecture 2: The Heart: Prof. Magidah Alaudi, M.SCDocument62 pagesLecture 2: The Heart: Prof. Magidah Alaudi, M.SCMonicaNo ratings yet
- Syncope and PalpitationsDocument1 pageSyncope and PalpitationsTom MallinsonNo ratings yet
- Asthma Review PDFDocument12 pagesAsthma Review PDFdanielc503No ratings yet
- Chap253-Heart Failure ManagementDocument42 pagesChap253-Heart Failure ManagementDoctor CastleNo ratings yet
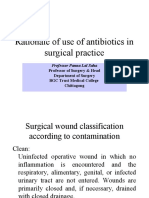
- 1.rationale of Use of Antibiotic in Surgical Patients CDocument22 pages1.rationale of Use of Antibiotic in Surgical Patients CPanna SahaNo ratings yet
- Vessels and CirculationDocument67 pagesVessels and CirculationTio UgantoroNo ratings yet
- TelemetryDocument3 pagesTelemetryKelly PrattNo ratings yet
- Diagnoses and Management Acute Headache Emergency DepartmentDocument37 pagesDiagnoses and Management Acute Headache Emergency DepartmentBendy Dwi IrawanNo ratings yet
- Physio Coursepack 2016Document282 pagesPhysio Coursepack 2016Amanda KimNo ratings yet
- GI Bleeding HXDocument3 pagesGI Bleeding HXBitu JaaNo ratings yet
- Cardiovascular: Surfaces of The HeartDocument6 pagesCardiovascular: Surfaces of The HeartironNo ratings yet
- Cardiac GlycosidesDocument8 pagesCardiac GlycosidesShan Sicat100% (1)
- 1 - Internal Medicine UKIDocument128 pages1 - Internal Medicine UKILewishoppusNo ratings yet
- Rama Id ConceptDocument49 pagesRama Id ConceptpiangpornNo ratings yet
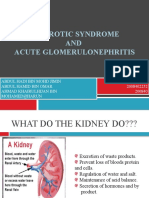
- NEPHROTIC SYNDROME - HamidDocument20 pagesNEPHROTIC SYNDROME - HamidAbdul Hamid OmarNo ratings yet
- Medicine Mneumonics - Copy - 4 - 2Document110 pagesMedicine Mneumonics - Copy - 4 - 2mumbafortune05No ratings yet
- Cardiac Drugs HypertensionDocument5 pagesCardiac Drugs HypertensionEciOwnsMeNo ratings yet
- CVS Examination 3rd MBDocument30 pagesCVS Examination 3rd MBsnowlover boyNo ratings yet
- Pediatric Emergency Medicine Resource 33164 - CSDY - FeverDocument7 pagesPediatric Emergency Medicine Resource 33164 - CSDY - FevervannesNo ratings yet
- Milrinone Can ONLY Be Mixed With NS!: Alpha 1 Beta 1 & Alpha 1Document1 pageMilrinone Can ONLY Be Mixed With NS!: Alpha 1 Beta 1 & Alpha 1njones33No ratings yet
- Mild Pain Treatment Algorithm: Pain Scale Rating 1/5 (0-5 Scale) or 1-3/10 (0-10 Scale)Document4 pagesMild Pain Treatment Algorithm: Pain Scale Rating 1/5 (0-5 Scale) or 1-3/10 (0-10 Scale)VickyNo ratings yet
- 132 Emergency MedicineDocument14 pages132 Emergency MedicineVania NandaNo ratings yet
- WWW Cram Com Flashcards Hematology Slides 872178Document8 pagesWWW Cram Com Flashcards Hematology Slides 872178Anonymous t5TDwdNo ratings yet
- Acute Asthma Exacerbation in AdultsDocument84 pagesAcute Asthma Exacerbation in AdultsAkif Ahamad100% (1)
- CerebellumDocument8 pagesCerebellumMohamed Hassan MohamudNo ratings yet
- Pharmacology RevisedDocument59 pagesPharmacology Revisedjohnstockton12100% (1)
- UTIDocument17 pagesUTIBongkotchakorn Mind PhonchaiNo ratings yet
- Story Board Internal MedicineDocument7 pagesStory Board Internal MedicineSarafina ElwindyNo ratings yet
- Pulmonary EmbolismDocument12 pagesPulmonary EmbolismJohn Paul MatienzoNo ratings yet
- Thrombolytics - Hematology - Medbullets Step 1Document5 pagesThrombolytics - Hematology - Medbullets Step 1aymen100% (1)
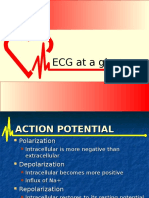
- ECG at A GlanceDocument53 pagesECG at A GlancePetrus TjiangNo ratings yet
- Cardiac InvestigationsDocument17 pagesCardiac InvestigationsTARIQ50% (2)
- PharmacologyDocument120 pagesPharmacologyFluffy_iceNo ratings yet
- GIS Modul 3 History Taking & Physical Examination of Diarrhea%Document3 pagesGIS Modul 3 History Taking & Physical Examination of Diarrhea%Windu Kumara100% (1)
- Pathophysiology of Congenital Heart Diseases PDFDocument8 pagesPathophysiology of Congenital Heart Diseases PDFdramitjainNo ratings yet
- Vital SignsDocument2 pagesVital SignsVSNo ratings yet
- Action Potential ECGDocument11 pagesAction Potential ECGAndrei ManeaNo ratings yet
- 115-NCLEX-RN Review Made Incredibly Easy, Fifth Edition (Incredibly Easy Series) - Lippincott-16083 - p87Document1 page115-NCLEX-RN Review Made Incredibly Easy, Fifth Edition (Incredibly Easy Series) - Lippincott-16083 - p87MuhNatsirNo ratings yet
- DVTDocument46 pagesDVTLuqman ArifNo ratings yet
- Cardiovascular BigDocument37 pagesCardiovascular Bigfaiz nasirNo ratings yet
- Audiometry Screening and Interpretation Aafp PDFDocument8 pagesAudiometry Screening and Interpretation Aafp PDFMaram AbdullahNo ratings yet
- JVP - WL GanDocument1 pageJVP - WL GanWeh Loong GanNo ratings yet
- Paeds Revisional SummaryDocument48 pagesPaeds Revisional SummaryJujhar BoparaiNo ratings yet
- TABLE 132 - Recreational Substances - Intoxication WithdrawalDocument3 pagesTABLE 132 - Recreational Substances - Intoxication WithdrawalDragutin PetrićNo ratings yet
- Medicine CPDocument127 pagesMedicine CPDipesh Shrestha100% (1)
- Biostatistics - Epidemiology Book 2023 (B&B) (Medicalstudyzone - Com)Document52 pagesBiostatistics - Epidemiology Book 2023 (B&B) (Medicalstudyzone - Com)Vincent DaoNo ratings yet
- Physiology of PainDocument43 pagesPhysiology of PainNashwan ANo ratings yet
- Essential DrugsDocument358 pagesEssential Drugsshahera rosdiNo ratings yet
- Community-Acquired Pneumonia: Strategies for ManagementFrom EverandCommunity-Acquired Pneumonia: Strategies for ManagementAntoni TorresRating: 4.5 out of 5 stars4.5/5 (2)
- Oil Gas Corporate Business Plan DevelopmentDocument6 pagesOil Gas Corporate Business Plan Developmentmule abadiNo ratings yet
- Mces MCQDocument50 pagesMces MCQshrimanNo ratings yet
- Vidya Bharti Ncert Chemistry Half Yearly Exam Paper #Paper LeakDocument4 pagesVidya Bharti Ncert Chemistry Half Yearly Exam Paper #Paper LeakAaditya KumarNo ratings yet
- Service Manual Videocon Ff-Vz330l, 280l, 250lDocument39 pagesService Manual Videocon Ff-Vz330l, 280l, 250ljitendraNo ratings yet
- HC Brochure 2019Document33 pagesHC Brochure 2019abul_1234No ratings yet
- Kumait@steelplantech - Co.jp Kikkawat@steelplantech - Co.jpDocument10 pagesKumait@steelplantech - Co.jp Kikkawat@steelplantech - Co.jpSANTOSH TIWARINo ratings yet
- The Apocalypse of ElijahDocument8 pagesThe Apocalypse of Elijahkamion0100% (1)
- Ball-Flange Impact Using Surface To Surface Contact ElementsDocument8 pagesBall-Flange Impact Using Surface To Surface Contact Elementsrishit_aNo ratings yet
- IN2010 Structured NotesDocument24 pagesIN2010 Structured NotesBjorn BirkelundNo ratings yet
- Flush Valve Systems by Schell SpecifierDocument7 pagesFlush Valve Systems by Schell SpecifierThasleem ThasliNo ratings yet
- 2010 Article 9566Document5 pages2010 Article 9566Shimul HalderNo ratings yet
- C 06 Momentum Energy and Simple SystemsDocument22 pagesC 06 Momentum Energy and Simple Systemsbhawnagaur1189No ratings yet
- Factsheet NIFTY LargeMidcap 250 IndexDocument2 pagesFactsheet NIFTY LargeMidcap 250 IndexRahul RanjanNo ratings yet
- Microsoft Word - AppearanceMEnetDocument1 pageMicrosoft Word - AppearanceMEnetinmaNo ratings yet
- Sant Gadge Baba Amravati University: Programme For Theory TIME: 09.00 AM To 12.00 NOON Subject Date DAYDocument6 pagesSant Gadge Baba Amravati University: Programme For Theory TIME: 09.00 AM To 12.00 NOON Subject Date DAYAmol IngleNo ratings yet
- In Gel Finger 2015Document10 pagesIn Gel Finger 2015Dumitrache VicentiuNo ratings yet
- Poerty AssignmentDocument5 pagesPoerty AssignmentJulie Marie BalabatNo ratings yet
- Phenol: A Guide For CAPE StudentsDocument11 pagesPhenol: A Guide For CAPE StudentsJordan SteeleNo ratings yet
- Concrete Utopia: Everyday Life and Socialism in Berlin-Marzahn Eli RubinDocument17 pagesConcrete Utopia: Everyday Life and Socialism in Berlin-Marzahn Eli RubinIoana TurcanuNo ratings yet
- Greedy AlgorithmsDocument110 pagesGreedy AlgorithmsMITALBAHEN DHOLAKIYANo ratings yet
- Pompeii HandoutDocument2 pagesPompeii Handoutapi-284672740No ratings yet
- Skyfire AvenueDocument162 pagesSkyfire AvenueMegumiNo ratings yet
- Dell Connectrix B-Series Fos 9-1-1c Rev 14 PDFDocument46 pagesDell Connectrix B-Series Fos 9-1-1c Rev 14 PDFmm.ashkanNo ratings yet
- Unseen PartnerDocument1 pageUnseen PartnerProcalimersNo ratings yet
- FWNSumm 13 LRDocument72 pagesFWNSumm 13 LRsabah8800No ratings yet
- Module 1 DDCODocument20 pagesModule 1 DDCOarshadahmedkkpNo ratings yet
- Huawei Optixstar P670E Series Datasheet: Product OverviewDocument3 pagesHuawei Optixstar P670E Series Datasheet: Product Overviewtang alexNo ratings yet