Wound Care: Jocelyn M. Lledo, MD
Wound Care: Jocelyn M. Lledo, MD
Download as pptx, pdf, or txt
At a glance
Powered by AI
Some of the earliest methods of wound care mentioned include homespun remedies using herbs and rituals from ancient clay tablets dating back to 2200 BC. Joseph Lister introduced the first antiseptic dressings in 1867 by soaking materials in carbolic acid. References to wound care can also be found in ancient religious texts and writings.
Some of the earliest methods mentioned include 'three healing gestures' from an ancient clay tablet involving washing the wound, applying mixtures to aid healing, and bandaging. The Bible and ancient Assyrian and Greek texts also reference applying oils, binding wounds, and using bandages.
Desirable wound dressing characteristics include protecting the wound from bacteria, absorbing exudate, preventing heat/fluid loss, providing compression to minimize edema, being non-adherent to limit disruption, creating a warm moist environment to maximize healing, and being aesthetically attractive.
You might also like
- Wound ClassificationDocument48 pagesWound Classificationzarizi100% (2)
- Negative Pressure Wound TherapyDocument21 pagesNegative Pressure Wound TherapyKathy Real Vills100% (2)
- Wound Healing (James)Document127 pagesWound Healing (James)Ronak Upadhyay100% (7)
- Best Practice Recommendations For Holistic Strategies To Promote and Maintain Skin IntegrityDocument32 pagesBest Practice Recommendations For Holistic Strategies To Promote and Maintain Skin IntegrityisaNo ratings yet
- Wounds and Wound CareDocument26 pagesWounds and Wound Careapi-3697326100% (2)
- Wound CareDocument50 pagesWound CareJan Oliver Yares100% (3)
- Syllabus of Modern Africa or Hist 258Document2 pagesSyllabus of Modern Africa or Hist 258api-148803805No ratings yet
- Wound Care Products: Department of Podiatric SurgeryDocument44 pagesWound Care Products: Department of Podiatric Surgerydrkbarry100% (8)
- Wound Care Dressings and Their Uses: Carolyn Watts MSN, RN, CWON Vanderbilt University Medical Center Nashville, TNDocument34 pagesWound Care Dressings and Their Uses: Carolyn Watts MSN, RN, CWON Vanderbilt University Medical Center Nashville, TNSuciNo ratings yet
- Dressings and DrainsDocument118 pagesDressings and DrainsBhanu PraseedhaNo ratings yet
- Stoma Management: Shankar ZanwarDocument33 pagesStoma Management: Shankar Zanwarpradeep nair100% (1)
- Ostomy Care in Home Health1Document39 pagesOstomy Care in Home Health1api-315120220100% (1)
- Delayed Wound HealingDocument9 pagesDelayed Wound HealingWill JoshNo ratings yet
- VaricoceleDocument10 pagesVaricoceleDenny SetyadiNo ratings yet
- StomaDocument37 pagesStomaAndryHarisNo ratings yet
- Wound CareDocument112 pagesWound CareJaymira Piezas PalobeNo ratings yet
- Surgical Site InfectionsDocument22 pagesSurgical Site InfectionsSheryl DurrNo ratings yet
- Leg UlcersDocument22 pagesLeg UlcersMarera DomnicNo ratings yet
- Exploring The Intricacies of Stoma CareDocument21 pagesExploring The Intricacies of Stoma CareMeta Paramita100% (1)
- HemorrhoidsDocument20 pagesHemorrhoidsEdwin PratamaNo ratings yet
- Wocn Ascrs Stoma Site Marking Fecal 2014 PDFDocument10 pagesWocn Ascrs Stoma Site Marking Fecal 2014 PDFamal.fathullahNo ratings yet
- Surgical Site InfectionDocument14 pagesSurgical Site InfectionSri AsmawatiNo ratings yet
- Wound CareDocument10 pagesWound CareKenima Idao100% (3)
- Pelvic Trauma - PPT 2010Document47 pagesPelvic Trauma - PPT 2010Chamila Senarathna100% (2)
- Wound MGMT Guidelines SEPTDocument93 pagesWound MGMT Guidelines SEPTYuda ArifkaNo ratings yet
- Wound ManagementDocument86 pagesWound ManagementRăzvanAndrei67% (3)
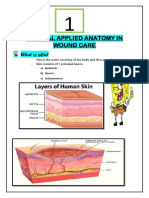
- Clinical Applied Anatomy in Wound CareDocument18 pagesClinical Applied Anatomy in Wound CareKlinik Komuniti Perwira100% (2)
- Skin Grafting SurgeryDocument15 pagesSkin Grafting SurgeryVithikaNo ratings yet
- Wound CareDocument41 pagesWound Carekamardin zakuani100% (3)
- Post Op Wound Care Instructions in Clinic For StudentDocument1 pagePost Op Wound Care Instructions in Clinic For StudentrezzkNo ratings yet
- Covid 19 Psychological Support: Department of Psychiatry, LLRM Medical College MeerutDocument23 pagesCovid 19 Psychological Support: Department of Psychiatry, LLRM Medical College MeerutNaina SharmaNo ratings yet
- Abdominal Trauma: Supervised By: Dr. Hussein Al-HeisDocument63 pagesAbdominal Trauma: Supervised By: Dr. Hussein Al-HeisRashed ShatnawiNo ratings yet
- Wound DebridementDocument53 pagesWound DebridementRahmat Arif Ayieb100% (1)
- Presentation of Wound DressingDocument17 pagesPresentation of Wound DressingGafur TarniNo ratings yet
- Wound HealingDocument75 pagesWound Healingirfan100% (2)
- ClubfootDocument52 pagesClubfootArianto PrabowoNo ratings yet
- Wound and Wound HealingDocument28 pagesWound and Wound HealingObehi Eromosele0% (1)
- Incision and DrainageDocument33 pagesIncision and DrainagemathisyncNo ratings yet
- Wound ManagementDocument72 pagesWound Managementdrsonuchawla100% (1)
- Principles of Wound HealingDocument8 pagesPrinciples of Wound HealingTracy100% (6)
- Orthopaedic SplintingDocument52 pagesOrthopaedic SplintingandhitaNo ratings yet
- MCU 2020 Advances in Pharmaceutical Technology Therapeutic Dressings PDFDocument431 pagesMCU 2020 Advances in Pharmaceutical Technology Therapeutic Dressings PDFLuis Gerardo Sandoval OrtizNo ratings yet
- The Wound CareDocument51 pagesThe Wound CareIosefina DudeanuNo ratings yet
- About Skin Cancer Useful InformationDocument40 pagesAbout Skin Cancer Useful Informationdianp88No ratings yet
- Basic Surgical Skills FinalDocument62 pagesBasic Surgical Skills Finalamel015No ratings yet
- Drains in SurgeryDocument66 pagesDrains in SurgeryBalaji MallaNo ratings yet
- Primary Skin LesionDocument7 pagesPrimary Skin Lesion_carido_No ratings yet
- BurnDocument69 pagesBurnntandayuNo ratings yet
- Class - Burns, Skin Graft & FlapsDocument44 pagesClass - Burns, Skin Graft & FlapsJyoti Sambharwal100% (1)
- Evidence-Based Medicine: Wound ManagementDocument16 pagesEvidence-Based Medicine: Wound ManagementRafael FerreiraNo ratings yet
- Damage Control OrthopaedicsDocument16 pagesDamage Control OrthopaedicsPatrick LukitoNo ratings yet
- (POLI TRAUMA) Decision Making in Trauma SurgeryDocument15 pages(POLI TRAUMA) Decision Making in Trauma SurgeryEdward Ojeda100% (2)
- Suturing Tools and TechniquesDocument51 pagesSuturing Tools and TechniquesIyad Abou-RabiiNo ratings yet
- Wounds & Wound HealingDocument47 pagesWounds & Wound HealingDrSarmad100% (3)
- ABC of Wound Healing WWW - Dof3tna - Net WWW - Egydr.com Drhamdy2009Document49 pagesABC of Wound Healing WWW - Dof3tna - Net WWW - Egydr.com Drhamdy2009steadiNo ratings yet
- Chapter 1 - Central Venous CathetersDocument6 pagesChapter 1 - Central Venous CathetersParth PatelNo ratings yet
- Wounds and Tissue RepairDocument4 pagesWounds and Tissue RepairMuhammad Mohsin Ali Dynamo50% (2)
- Skin Integrity and Wound CareDocument47 pagesSkin Integrity and Wound CareCHALIE MEQUNo ratings yet
- Wound Healing and Skin Integrity: Principles and PracticeFrom EverandWound Healing and Skin Integrity: Principles and PracticeRating: 5 out of 5 stars5/5 (1)
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- PinesDocument5 pagesPinesShona GeeyNo ratings yet
- Hans Eysenck's Biologically Based Factor TheoryDocument17 pagesHans Eysenck's Biologically Based Factor TheoryJoanna Marie SillanoNo ratings yet
- By: Dr. Ahmad Shafaat: A Study of Ahadith About The Determination of Islamic DatesDocument32 pagesBy: Dr. Ahmad Shafaat: A Study of Ahadith About The Determination of Islamic DatesAbdullahNo ratings yet
- VideoJet 43sDocument2 pagesVideoJet 43sDavid Huaman100% (1)
- Yujuico vs. AtienzaDocument2 pagesYujuico vs. AtienzaRenzoSantosNo ratings yet
- Literature Review On Motor Skill and Physical Activity in Preschool Children in New ZealandDocument18 pagesLiterature Review On Motor Skill and Physical Activity in Preschool Children in New ZealandArie AnggaNo ratings yet
- NCM 105 Lec Final NotesDocument3 pagesNCM 105 Lec Final Notescherryle whiteNo ratings yet
- Baylor Graduate Catalog 2013-2014Document504 pagesBaylor Graduate Catalog 2013-2014theapguyNo ratings yet
- Shantanu Agnihotri - HistoryDocument31 pagesShantanu Agnihotri - HistoryShantanu AgnihotriNo ratings yet
- Roan v. GonzalesDocument2 pagesRoan v. GonzalesMoon BeamsNo ratings yet
- Ingilizce Saygiliyim 2 Boyama KitabiDocument18 pagesIngilizce Saygiliyim 2 Boyama KitabiLiaisan KiekbaevaNo ratings yet
- Smoothed Particle Hydrodynamics: From Continuum To ParticlesDocument28 pagesSmoothed Particle Hydrodynamics: From Continuum To Particlesdr_kh_ahmedNo ratings yet
- Physical Development of Infants & ToddlersDocument28 pagesPhysical Development of Infants & ToddlersSanie Gaspar Bautista100% (4)
- Nithya - My Friend's WifeDocument14 pagesNithya - My Friend's Wifegoudtsri42% (19)
- Đề Cương Tiếng Anh 1 Có Đáp ÁnDocument40 pagesĐề Cương Tiếng Anh 1 Có Đáp ÁnNguyendung29031984No ratings yet
- Reflection CSDocument2 pagesReflection CSShamil UsrahNo ratings yet
- Solaris KernelDocument3 pagesSolaris KernelDungNo ratings yet
- Chemistry Project STD XiiDocument2 pagesChemistry Project STD Xiibone fire100% (1)
- Kanchi Periva Forum Newsletter Vol 1Document18 pagesKanchi Periva Forum Newsletter Vol 1Chandra Shekar0% (1)
- An Investigation of Sustainable Maintenance Performance Indicators Identification Expert Validation and Portfolio of Future ResearchDocument18 pagesAn Investigation of Sustainable Maintenance Performance Indicators Identification Expert Validation and Portfolio of Future ResearchMelinda IbrahimNo ratings yet
- Sredni Vashtar: by H H Munro (Saki)Document4 pagesSredni Vashtar: by H H Munro (Saki)Melike ÇelikNo ratings yet
- Premier Inn - Mulit-Channel MarketingDocument27 pagesPremier Inn - Mulit-Channel MarketingOlanrewaju Rasheed OpeyemiNo ratings yet
- Arisha Alif LamhaDocument1 pageArisha Alif LamhaFactory of IntelligenceNo ratings yet
- Nutrigest: A Herbal and Nutritional Therapy For Digestive DisordersDocument34 pagesNutrigest: A Herbal and Nutritional Therapy For Digestive DisordersANo ratings yet
- Measureschool GTM Resource Guide 2018Document10 pagesMeasureschool GTM Resource Guide 2018Матеја МерџановићNo ratings yet
- Judicial Affidavit RapeDocument5 pagesJudicial Affidavit RapeJasOn EvangelistaNo ratings yet
- 16 Personality Factor Score Low Marks and CharacteristicsDocument13 pages16 Personality Factor Score Low Marks and Characteristicssrpati_55555100% (1)
- 10 1016@j Iref 2020 06 026Document47 pages10 1016@j Iref 2020 06 026Graphix GurujiNo ratings yet
- Stronger Than Circumstances 2022Document26 pagesStronger Than Circumstances 2022Cammy87No ratings yet