DementiaDiagTreat 02 08
DementiaDiagTreat 02 08
Download as ppt, pdf, or txt
You might also like
- Psychiatric Nursing Notes PDFDocument12 pagesPsychiatric Nursing Notes PDFClaire Lautner95% (61)
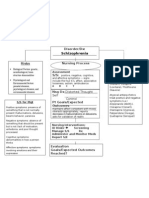
- Schizophrenia Concept MapDocument1 pageSchizophrenia Concept MapGabrielle Franklin86% (7)
- Psychotic Disorders in Elderly Persons: Carl I. Cohen, M.D.Document68 pagesPsychotic Disorders in Elderly Persons: Carl I. Cohen, M.D.Kreshnik IdrizajNo ratings yet
- Etiopathogenesis of DeliriumDocument36 pagesEtiopathogenesis of DeliriumAarti Gupta100% (1)
- RCSI Course Book Chapters 22-27 Week 4Document75 pagesRCSI Course Book Chapters 22-27 Week 4BoyNo ratings yet
- PASS Pharm DrillsDocument36 pagesPASS Pharm DrillsSwisskelly1No ratings yet
- Dementia: Diagnosis and TreatmentDocument53 pagesDementia: Diagnosis and Treatmentakashdeep050% (1)
- Lecture 16 - DementiaDocument44 pagesLecture 16 - Dementiaepic sound everNo ratings yet
- Evaluation of The Patient With Dementia1747Document39 pagesEvaluation of The Patient With Dementia1747Paijo SusenoNo ratings yet
- Dementia: I Wayan Tunjung, DR - Sp.S. Bagian Neurologi RSU Kota MataramDocument67 pagesDementia: I Wayan Tunjung, DR - Sp.S. Bagian Neurologi RSU Kota MataramHerlinawatiHariniNo ratings yet
- Elderly CareDocument69 pagesElderly Caremohamad najeemNo ratings yet
- Althimer's ResearchDocument99 pagesAlthimer's Researchdeemoney3No ratings yet
- Dementia: Sariu Ali DidiDocument31 pagesDementia: Sariu Ali DidiSariu Ali DidiNo ratings yet
- Organic Brain SyndromeDocument28 pagesOrganic Brain SyndromeSena AjahNo ratings yet
- Old Age Psychiatry LectureDocument38 pagesOld Age Psychiatry LectureMo 'Fishpondz' IsmailNo ratings yet
- ConfusionDocument4 pagesConfusionjaffar mahNo ratings yet
- Major Neurocognitive DisorderDocument92 pagesMajor Neurocognitive DisorderJake MillerNo ratings yet
- Delirium, Dementia, and Amnestic and Other Cognitive DisordersDocument78 pagesDelirium, Dementia, and Amnestic and Other Cognitive DisordersjashchiruNo ratings yet
- Delirium, Dementia, and Amnestic and Other Cognitive DisordersDocument78 pagesDelirium, Dementia, and Amnestic and Other Cognitive DisordersrashidNo ratings yet
- SCE Geriatrics CompressedDocument434 pagesSCE Geriatrics CompressedFaris FirasNo ratings yet
- SCE GeriatricsDocument434 pagesSCE GeriatricsFaris FirasNo ratings yet
- PowerPoint Cognitive DisordersDocument22 pagesPowerPoint Cognitive Disordersiqra-j100% (3)
- An Overview of DementiaDocument44 pagesAn Overview of DementiaAnil Kakunje100% (1)
- Alzheimer S Disease and Related Dementias-2014Document34 pagesAlzheimer S Disease and Related Dementias-2014thuhvo100% (1)
- DementiaDocument26 pagesDementianadya100% (4)
- Dementia ReportDocument8 pagesDementia ReportHilas Rosalliv KcinmorNo ratings yet
- Dementia AssignmentDocument19 pagesDementia AssignmentVandna Vikram Novlani50% (2)
- DementiaDocument60 pagesDementiaRuaa HdeibNo ratings yet
- Delirium, Dementia, and Amnestic and Other Cognitive DisordersDocument78 pagesDelirium, Dementia, and Amnestic and Other Cognitive DisordersSachin R BhardwajNo ratings yet
- Dementia and Mental Health Conditions NewDocument48 pagesDementia and Mental Health Conditions NewMedan MusaNo ratings yet
- Alzheimer Disease and Other DementiasDocument28 pagesAlzheimer Disease and Other DementiasIlham 123456No ratings yet
- Sarthak - Neurocognitive Disorders - Behaviour DysfunctionDocument41 pagesSarthak - Neurocognitive Disorders - Behaviour DysfunctionSarthak Kumar SinghNo ratings yet
- DEMENCIJEDocument9 pagesDEMENCIJEMarko MoonRocker TomičevićNo ratings yet
- DementiaDocument38 pagesDementiarajikakurupNo ratings yet
- Psychosis in The Older PatientDocument25 pagesPsychosis in The Older PatientKreshnik Idrizaj100% (1)
- Alzheimer and SocietyDocument10 pagesAlzheimer and SocietyAdriana PalomaresNo ratings yet
- PN0621 CF1 ClinicalApproachDementiaDocument5 pagesPN0621 CF1 ClinicalApproachDementiaSwayang Sudha PandaNo ratings yet
- Dementia Conversion DisordersDocument28 pagesDementia Conversion DisordersAYO NELSON100% (1)
- 17-Delirium DementiaDocument34 pages17-Delirium DementiaNada Ehab100% (1)
- Delirium Dementia and Depression SPR 2011-1Document27 pagesDelirium Dementia and Depression SPR 2011-1advpracrn1No ratings yet
- Failing: Dementia: The BrainDocument4 pagesFailing: Dementia: The BrainAleja ToPaNo ratings yet
- Mci, Dementia, Alzheimer DiseaseDocument60 pagesMci, Dementia, Alzheimer DiseaseDave Siahaan de KaratekaNo ratings yet
- L4 - Alzheimer's Disease, Dementia, and Mild Cognitive ImpairmentDocument9 pagesL4 - Alzheimer's Disease, Dementia, and Mild Cognitive Impairmentlmm20030321No ratings yet
- Neurocognitive DisordersDocument26 pagesNeurocognitive Disordershaidar aliNo ratings yet
- Dementia 1Document32 pagesDementia 1Mahendra ThakreNo ratings yet
- Dementia 2Document70 pagesDementia 2Vennilavan SothithasanNo ratings yet
- The Alzheimer's DiseaseDocument16 pagesThe Alzheimer's Diseasemelanita_99No ratings yet
- Dementia and DeliriumDocument20 pagesDementia and DeliriumWyz ClassNo ratings yet
- DEMENTIA - Neurological DisordersDocument12 pagesDEMENTIA - Neurological Disorderspreveenna100% (1)
- Chapter 14 Cognitive DisordersDocument43 pagesChapter 14 Cognitive DisordersClaire Go TajarrosNo ratings yet
- PT Assessment and Management of Parkinson's DiseaseDocument40 pagesPT Assessment and Management of Parkinson's DiseaseNeha Dubey100% (1)
- DementiaDocument40 pagesDementiakhusnul100% (2)
- Dementia: DR Ayunga A.O Physician/lecturer MedicineDocument34 pagesDementia: DR Ayunga A.O Physician/lecturer MedicineMalueth AnguiNo ratings yet
- Dementia: Dr. Sharlene Alick OrtizDocument32 pagesDementia: Dr. Sharlene Alick OrtizShary AlickNo ratings yet
- Dr. Maximiliano Fürnes ValdésDocument65 pagesDr. Maximiliano Fürnes ValdésfelixperezvNo ratings yet
- Dementia in Neuroscience: Departement of Neurology Christian University of Indonesia Medical FacultyDocument42 pagesDementia in Neuroscience: Departement of Neurology Christian University of Indonesia Medical FacultyDendiNugrahaIsliantoNo ratings yet
- Alzheimers InenglishDocument6 pagesAlzheimers InenglishFrengki PenbainNo ratings yet
- Geriatric Psychiatry LectureDocument113 pagesGeriatric Psychiatry LectureabrihamNo ratings yet
- Chapter 10: Nursing Management of DementiaDocument4 pagesChapter 10: Nursing Management of DementiaJoanne FojaNo ratings yet
- NEUROLOGÍA 2do. TrimestralDocument12 pagesNEUROLOGÍA 2do. TrimestralDaniela SarmientoNo ratings yet
- Cns Degenerative 1Document33 pagesCns Degenerative 1Mashal KhanNo ratings yet
- Psikologi ManulaDocument90 pagesPsikologi ManulaDian PuspaNo ratings yet
- Late Life and Neurocognitive DisordersDocument24 pagesLate Life and Neurocognitive DisordersJonnaNo ratings yet
- Treatment of Depression in 21 Century: Ascent NBI and TMS Center A. Sibel Yasar, MDDocument66 pagesTreatment of Depression in 21 Century: Ascent NBI and TMS Center A. Sibel Yasar, MDANTolaniNo ratings yet
- Synthetic Drugs of Abuse: Spice,' K2' and Bath Salts'Document27 pagesSynthetic Drugs of Abuse: Spice,' K2' and Bath Salts'ANTolaniNo ratings yet
- Recognizing and Responding To Acute SeizuresDocument27 pagesRecognizing and Responding To Acute SeizuresANTolaniNo ratings yet
- Methods RTMS: Department of Physics of Complex Systems, The Weizmann Institute of Science, Rehovot, IsraelDocument1 pageMethods RTMS: Department of Physics of Complex Systems, The Weizmann Institute of Science, Rehovot, IsraelANTolaniNo ratings yet
- Techniques in Cognitive Neuroscience: Transcranial Magnetic Stimulation (TMS)Document33 pagesTechniques in Cognitive Neuroscience: Transcranial Magnetic Stimulation (TMS)ANTolaniNo ratings yet
- TMS Lecture2Document33 pagesTMS Lecture2ANTolaniNo ratings yet
- Transcranial Magnetic Stimulation: Rachel Mcateer Bme 281Document12 pagesTranscranial Magnetic Stimulation: Rachel Mcateer Bme 281ANTolaniNo ratings yet
- Psoriasis For DummiesDocument20 pagesPsoriasis For DummiesANTolaniNo ratings yet
- Diabetes 101: A Brief Overview of Diabetes and The American Diabetes AssociationDocument32 pagesDiabetes 101: A Brief Overview of Diabetes and The American Diabetes AssociationANTolaniNo ratings yet
- Tariq Faridi TMS Presentation To Congressmen GaramendiDocument19 pagesTariq Faridi TMS Presentation To Congressmen GaramendiANTolaniNo ratings yet
- Module1 Overview HivinfectionDocument20 pagesModule1 Overview HivinfectionANTolaniNo ratings yet
- Jonathan M. Meyer, M.D Assistant Professor Department of Psychiatry University of California San DiegoDocument25 pagesJonathan M. Meyer, M.D Assistant Professor Department of Psychiatry University of California San DiegoANTolaniNo ratings yet
- Freud & PsychoanalysisDocument14 pagesFreud & PsychoanalysisANTolaniNo ratings yet
- Catatonia - Treatment and Prognosis - UpToDateDocument12 pagesCatatonia - Treatment and Prognosis - UpToDateTeofilo QuenayaNo ratings yet
- TABLE 56-4 - Neurological Side Effects of Antipsychotic DrugsDocument1 pageTABLE 56-4 - Neurological Side Effects of Antipsychotic DrugsDragutin PetrićNo ratings yet
- Personality DisordersDocument20 pagesPersonality DisordersJunathan DelgadoNo ratings yet
- Reed 2008Document7 pagesReed 2008gustavoppicalloNo ratings yet
- Diagnosis and Management of Agitation 2017Document288 pagesDiagnosis and Management of Agitation 2017SisoesNo ratings yet
- Drug Study 2 de Guzman Miguel Paulo P. NCMHDocument2 pagesDrug Study 2 de Guzman Miguel Paulo P. NCMHMark Angelo SarmientoNo ratings yet
- Interpreting and Implementing The 2018 Pain, Agitation:Sedation, Delirium, Immobility, and Sleep Disruption Clinical Practice Guideline - Balas2018Document7 pagesInterpreting and Implementing The 2018 Pain, Agitation:Sedation, Delirium, Immobility, and Sleep Disruption Clinical Practice Guideline - Balas2018RodrigoSachiFreitasNo ratings yet
- 09 Questions and Rationale On Psychotic DisordersDocument25 pages09 Questions and Rationale On Psychotic DisordersLot RositNo ratings yet
- Pocket Guide To 2015 Beers Criteria PDFDocument7 pagesPocket Guide To 2015 Beers Criteria PDFYuliEdySeringnyungsepNo ratings yet
- What Is Coprolalia, Tourette's SyndromeDocument3 pagesWhat Is Coprolalia, Tourette's Syndromehttp://feelgoodtime.netNo ratings yet
- Psychiatry History & Suicide Risk Assessment TemplatesDocument32 pagesPsychiatry History & Suicide Risk Assessment TemplatesDuncan Jackson100% (6)
- Draft CPG Management of Bipolar Disorder in AdultsDocument63 pagesDraft CPG Management of Bipolar Disorder in AdultsredroseeeeeeNo ratings yet
- Drug Study CCMHDocument35 pagesDrug Study CCMHJose Mari F. EsguerraNo ratings yet
- PsychodynamicsDocument11 pagesPsychodynamicsOrlino PeterNo ratings yet
- A. George Awad Lakshmi N.P. Voruganti Eds. Beyond Assessment of Quality of Life in Schizophrenia ADIS 2016Document226 pagesA. George Awad Lakshmi N.P. Voruganti Eds. Beyond Assessment of Quality of Life in Schizophrenia ADIS 2016Toader AndreiNo ratings yet
- Mina Drug StudyDocument7 pagesMina Drug StudyChi Chaw Giselle HilarioNo ratings yet
- World Psychiatry - October 2013Document100 pagesWorld Psychiatry - October 2013zokica5No ratings yet
- Mood DisordersDocument54 pagesMood Disordersindranilghosh1401100% (1)
- اسئلة وزارية زهايمر + ملخصDocument6 pagesاسئلة وزارية زهايمر + ملخصبراء طاهر حاتمNo ratings yet
- Schizoaffective DisorderDocument6 pagesSchizoaffective DisorderJenish FitnessCoachNo ratings yet
- Salipla, MM DsDocument9 pagesSalipla, MM DsMohamad Masukat SaliplaNo ratings yet
- SM 8Document9 pagesSM 819Ketut Lingga AmritiyaNo ratings yet
- Child and Adolescent Psychiatry: A. Pervasive and Developmental DisordersDocument6 pagesChild and Adolescent Psychiatry: A. Pervasive and Developmental DisordersIsabel CastilloNo ratings yet
- 1ST Drug StudyDocument10 pages1ST Drug Study황춘히No ratings yet
- Cognitive Remediation Therapy (CRT) : Improving Neurocognition and Functioning in SchizophreniaDocument19 pagesCognitive Remediation Therapy (CRT) : Improving Neurocognition and Functioning in SchizophreniaKaterina ChatzNo ratings yet
- Drug Induced Movement DisordersDocument65 pagesDrug Induced Movement DisordersShaunak Patil100% (1)