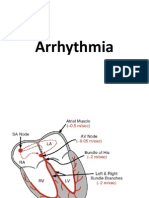
Atrial Fibrillation
Atrial Fibrillation
Download as ppt, pdf, or txt
You might also like
- Social Media and Eating Disorders Power Point 1Document20 pagesSocial Media and Eating Disorders Power Point 1dludwig127100% (1)
- Glanders in HorseDocument43 pagesGlanders in HorseWerner AlbuquerqueNo ratings yet
- Vital SignsDocument2 pagesVital SignsVSNo ratings yet
- Regulation of Heart Rate, Stroke Volume, Cardiac Output, Blood FlowDocument20 pagesRegulation of Heart Rate, Stroke Volume, Cardiac Output, Blood FlowShveta MahajanNo ratings yet
- Disease Mechanism of Action NoteDocument3 pagesDisease Mechanism of Action Noteamoody95No ratings yet
- Hypertension Treatment Steps For HypertensionDocument15 pagesHypertension Treatment Steps For Hypertensionfreelancer08100% (1)
- Patofisiologi AritmiaDocument27 pagesPatofisiologi AritmiaVedora Angelia GultomNo ratings yet
- Raised Intracranial PressureDocument6 pagesRaised Intracranial PressureindihimmakhairaniNo ratings yet
- Electrocardiogram Interpretation: A Brief OverviewDocument49 pagesElectrocardiogram Interpretation: A Brief Overviewnana wandhana100% (1)
- Pericardial Diseases - Dr. BartolomeDocument8 pagesPericardial Diseases - Dr. BartolomeMedisina101No ratings yet
- Sick Sinus Syndrom PDFDocument8 pagesSick Sinus Syndrom PDFSigit PratamaNo ratings yet
- Action Potential ECGDocument11 pagesAction Potential ECGAndrei ManeaNo ratings yet
- Journal of Arrhythmia - 2022 - Ono - JCS JHRS 2020 Guideline On Pharmacotherapy of Cardiac ArrhythmiasDocument141 pagesJournal of Arrhythmia - 2022 - Ono - JCS JHRS 2020 Guideline On Pharmacotherapy of Cardiac ArrhythmiastochtliNo ratings yet
- Cardio-Vascular Disease: Mitral Stenosis & Mitral RegurgitationDocument25 pagesCardio-Vascular Disease: Mitral Stenosis & Mitral Regurgitationyulia silviNo ratings yet
- ARRHYTHMIADocument25 pagesARRHYTHMIAAsma MuhammadiNo ratings yet
- ArrhythmiaDocument25 pagesArrhythmiad_94No ratings yet
- Show Questions One by OneDocument12 pagesShow Questions One by OneCharlie Cheng-Ying HsiehNo ratings yet
- Chest Pain: LSU Medical Student Clerkship, New Orleans, LADocument56 pagesChest Pain: LSU Medical Student Clerkship, New Orleans, LAGlucose DRglucoseNo ratings yet
- Clinical Use of DiureticsDocument9 pagesClinical Use of DiureticsAnonymous ZUaUz1wwNo ratings yet
- Seizure in AdultsDocument30 pagesSeizure in AdultsDaniela GonzalezNo ratings yet
- Ischemic Heart Disease (IHD)Document37 pagesIschemic Heart Disease (IHD)Yowan SusantiNo ratings yet
- Myocardial Perfusion ScanDocument47 pagesMyocardial Perfusion ScanAkram100% (1)
- Ranolazine An Update - AbbottDocument15 pagesRanolazine An Update - Abbottiloveit52252100% (1)
- Cardiovascular SyllabusDocument13 pagesCardiovascular SyllabusBrandonGilbertNo ratings yet
- ECGDocument33 pagesECGTamia PutriNo ratings yet
- Pulmonary Hypertension A Brief Guide For CliniciansDocument11 pagesPulmonary Hypertension A Brief Guide For CliniciansMarvin Josue Bustamante GutierrezNo ratings yet
- Cardiac MurmursDocument53 pagesCardiac MurmursdrgashokNo ratings yet
- Liver and Biliary System: DR Anil Chaudhary Associate Professor PhysiologyDocument31 pagesLiver and Biliary System: DR Anil Chaudhary Associate Professor Physiologylion2chNo ratings yet
- ArrhythmiasDocument57 pagesArrhythmiasAmra ahmedNo ratings yet
- Resistant Hypertension - Cleveland Clinic (2023)Document11 pagesResistant Hypertension - Cleveland Clinic (2023)Areli KamuiNo ratings yet
- Chronic Congestive Heart Failure: American Heart Association Sociedad Española de CardiologíaDocument94 pagesChronic Congestive Heart Failure: American Heart Association Sociedad Española de Cardiologíaladyminervs08100% (2)
- Myocardial InfarctionDocument25 pagesMyocardial Infarctionfam111222No ratings yet
- Cardiac CycleDocument30 pagesCardiac CycleAdel100% (1)
- Blood Pressure and Heart PulseDocument7 pagesBlood Pressure and Heart PulseHuda Behrooz0% (1)
- Acid-Base BalanceDocument38 pagesAcid-Base BalanceNym Angga SantosaNo ratings yet
- Adult Respiratory Distress Syndrome: Mazen Kherallah, MD, FCCPDocument51 pagesAdult Respiratory Distress Syndrome: Mazen Kherallah, MD, FCCPArsitoNo ratings yet
- Pharmacotherapy of Heart Failure: Abera J. (Bpharm., MSC in Clinical Pharmacy) School of Pharmacy, CHMS, HuDocument79 pagesPharmacotherapy of Heart Failure: Abera J. (Bpharm., MSC in Clinical Pharmacy) School of Pharmacy, CHMS, HuAbera JamboNo ratings yet
- Neurological Exam Lecture Notes PDFDocument26 pagesNeurological Exam Lecture Notes PDFSrinivas Pingali100% (1)
- Atrial Fibrillation: Presented by ShehzadiDocument17 pagesAtrial Fibrillation: Presented by ShehzadisamNo ratings yet
- Arrhythmia 2Document31 pagesArrhythmia 2rittvedNo ratings yet
- Hypertension Study GuideDocument4 pagesHypertension Study GuideCarl Elexer Cuyugan AnoNo ratings yet
- Cardiomyopathy: By: P.Dhilip KumarDocument29 pagesCardiomyopathy: By: P.Dhilip Kumarpreet kaur100% (1)
- ArrhythmiasDocument55 pagesArrhythmiasAzmi Ikhsan AzharyNo ratings yet
- Rare Case of Autoimmune Thyroid Disease - Hashimotosis With Microcytic Anaemia - in Seven Year Male Child (Chronic Lymphocytic Thyroiditis)Document2 pagesRare Case of Autoimmune Thyroid Disease - Hashimotosis With Microcytic Anaemia - in Seven Year Male Child (Chronic Lymphocytic Thyroiditis)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Types of ArrhythmiaDocument10 pagesTypes of ArrhythmiaRonilyn Mae AlvarezNo ratings yet
- CHF PathophysiologyDocument4 pagesCHF PathophysiologyVirtudazo JessaNo ratings yet
- Arrhythmia For NursesDocument49 pagesArrhythmia For NursesRajesh T EapenNo ratings yet
- AlopeciaDocument1 pageAlopeciachoobiNo ratings yet
- Ebm Therapeutics Lecture For MsucomDocument51 pagesEbm Therapeutics Lecture For MsucomKenneth NuñezNo ratings yet
- Cardiovascular - Anatomy & PhysiologyDocument23 pagesCardiovascular - Anatomy & PhysiologySanthoshi Sadhanaa Sankar100% (1)
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 pagesCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoNo ratings yet
- Understanding Coronary Heart DiseaseDocument22 pagesUnderstanding Coronary Heart DiseaseJa ClementeNo ratings yet
- Coronary Artery Disease Cad2Document182 pagesCoronary Artery Disease Cad2Mamot Mot0% (1)
- MigraineDocument9 pagesMigraineRose Athena SibalaNo ratings yet
- DysrhythmiasDocument85 pagesDysrhythmiasDipika JangpangiNo ratings yet
- Arrhythmia ReviewDocument33 pagesArrhythmia ReviewMark Hammerschmidt100% (3)
- Approach To Arrythmia RecognitionDocument64 pagesApproach To Arrythmia RecognitionSumiJoseNo ratings yet
- Pulse and Blood PressureDocument9 pagesPulse and Blood PressureadminchemNo ratings yet
- Descending TractDocument10 pagesDescending TractQairul AzmanNo ratings yet
- Brugada SyndromeDocument12 pagesBrugada SyndromeIslam KhedrNo ratings yet
- Supraventricular ArrhythmiasDocument56 pagesSupraventricular ArrhythmiasGading AuroraNo ratings yet
- Practice Essentials: Signs and SymptomsDocument7 pagesPractice Essentials: Signs and Symptomsliya larassatiNo ratings yet
- Spirometer Users and Buyers Guide 2015 UpdatedDocument28 pagesSpirometer Users and Buyers Guide 2015 UpdatedNikhil KumarNo ratings yet
- TOC MillerDocument5 pagesTOC MillerNikhil KumarNo ratings yet
- EntDocument105 pagesEntNikhil KumarNo ratings yet
- Stage 3 Handbook 2012Document21 pagesStage 3 Handbook 2012Nikhil KumarNo ratings yet
- Tableofinternshipcapacitybynetworks2012 ForwebsiteDocument1 pageTableofinternshipcapacitybynetworks2012 ForwebsiteNikhil KumarNo ratings yet
- 2chain of DiseaseDocument43 pages2chain of Diseaseyuuki konno100% (1)
- A Chronic Lymphocytic Leukemia Patient With Progressive Multifocal Leukoencephalopathy Caused by John Cunningham VirusDocument8 pagesA Chronic Lymphocytic Leukemia Patient With Progressive Multifocal Leukoencephalopathy Caused by John Cunningham VirusYtyNo ratings yet
- Psychiatric NursingDocument26 pagesPsychiatric Nursingshenric16No ratings yet
- Chronic Kidney DiseaseDocument8 pagesChronic Kidney DiseaseSally MavyNo ratings yet
- Nutritional AssessmentDocument6 pagesNutritional AssessmentReyna Mee Ahiyas100% (1)
- GI Bleeding (Text)Document11 pagesGI Bleeding (Text)Hart ElettNo ratings yet
- Nclex Pedia DisordersDocument7 pagesNclex Pedia Disordersarcci balinasNo ratings yet
- Role of The Kidney in Long Term RegulationDocument19 pagesRole of The Kidney in Long Term RegulationMelisa NovitasariNo ratings yet
- Critical Limb IschemiaDocument29 pagesCritical Limb IschemiadockunNo ratings yet
- Singkatan Diagnosa A-ZDocument23 pagesSingkatan Diagnosa A-ZElisabeth AnitaNo ratings yet
- Application CoopMED Health Insurance Plan BarbadosDocument2 pagesApplication CoopMED Health Insurance Plan BarbadosKammieNo ratings yet
- Task 2 Case Notes: Brendan CrossDocument4 pagesTask 2 Case Notes: Brendan Crossprakash poudelNo ratings yet
- ThyrotoxicosisDocument42 pagesThyrotoxicosisShaw Khan100% (7)
- Portfolio2nd Revised Argument Essay Miranda SuggsDocument5 pagesPortfolio2nd Revised Argument Essay Miranda Suggsapi-252312620No ratings yet
- Chapter 9-10Document4 pagesChapter 9-10valeria camila leon 7bNo ratings yet
- Kode Diagnosa-1 TambahanDocument8 pagesKode Diagnosa-1 TambahanbundamegaNo ratings yet
- Kisi Kisi Ujian Genap B Ing XiDocument4 pagesKisi Kisi Ujian Genap B Ing Xibalqisaasahr29No ratings yet
- Constipation Guideline PDFDocument13 pagesConstipation Guideline PDFCarimaGhalieNo ratings yet
- Gastrointestinal Disorders: Care of The Patients With Altered MetabolismDocument6 pagesGastrointestinal Disorders: Care of The Patients With Altered MetabolismHazel BandayNo ratings yet
- Pascual, Jayvin - CHAPTER 1Document18 pagesPascual, Jayvin - CHAPTER 1Marlon CalbangNo ratings yet
- Quiz 2 ReviewDocument19 pagesQuiz 2 ReviewKelsey Bissell100% (1)
- Transient Tachypnea of The Newborn: Fetal LungDocument5 pagesTransient Tachypnea of The Newborn: Fetal LungNurul HafizahNo ratings yet
- Common Signs and SymptomsDocument5 pagesCommon Signs and SymptomsPeopleNo ratings yet
- Diarrhea NCPDocument34 pagesDiarrhea NCPchezian smartNo ratings yet
- Exam of The AbdomenDocument11 pagesExam of The AbdomenjohnNo ratings yet
- FT 112 General MicrobiologyDocument9 pagesFT 112 General MicrobiologyPrincess Lia SarnoNo ratings yet
- Alzheimer's disease: early diagnosis and treatment: LW Chu 朱亮榮Document10 pagesAlzheimer's disease: early diagnosis and treatment: LW Chu 朱亮榮Dana LebadaNo ratings yet
- 190 EutecRodDocument4 pages190 EutecRodMohamed AdelNo ratings yet