Problem 2A (Adult) : Frudensia Kristiana
Problem 2A (Adult) : Frudensia Kristiana
Download as ppt, pdf, or txt
You might also like
- Dead Inside - Do Not Enter - Notes From The Zombie Apocalypse (Lost Zombies)Document169 pagesDead Inside - Do Not Enter - Notes From The Zombie Apocalypse (Lost Zombies)KIM KYRISH DELA CRUZNo ratings yet
- Peritoneum and Peritoneal CavityDocument26 pagesPeritoneum and Peritoneal CavitytuhinsinghNo ratings yet
- Hospital Linen ManagementDocument2 pagesHospital Linen Managementsrngm67% (3)
- Learning ObjectivesDocument162 pagesLearning ObjectivesNovita IskandarNo ratings yet
- Pemicu 2 GIDocument123 pagesPemicu 2 GIDessy DsyNo ratings yet
- Pemicu 2 Git StephenDocument169 pagesPemicu 2 Git StephenRana RickNo ratings yet
- Anatomy of StomachDocument4 pagesAnatomy of StomachIntan Putri Maisarah100% (1)
- Structures of The ForegutDocument13 pagesStructures of The ForegutJatan KothariNo ratings yet
- Stomach and Small IntestineDocument12 pagesStomach and Small IntestineOnwumerechimdikepreciousNo ratings yet
- Anatomy and Histology Gaster - DuodenumDocument149 pagesAnatomy and Histology Gaster - DuodenumRevila AuliaNo ratings yet
- Nahrain University - Abdomen - UPPER GIT ANATOMYDocument42 pagesNahrain University - Abdomen - UPPER GIT ANATOMYSalman KhanNo ratings yet
- My StomachDocument24 pagesMy StomachPriya GKNo ratings yet
- Anatomy of Abdominal VisceralsDocument189 pagesAnatomy of Abdominal VisceralsademabdellaaleNo ratings yet
- StomachDocument18 pagesStomachShimmering MoonNo ratings yet
- Abdominal Cavity: Prep by Lect: S Hassan AskariDocument38 pagesAbdominal Cavity: Prep by Lect: S Hassan AskariNaveed AfridiNo ratings yet
- Ac 2Document104 pagesAc 2saide limNo ratings yet
- Anatomi EsofagusDocument14 pagesAnatomi EsofagusSandy PranadaNo ratings yet
- Stomach: Arterial and Venous Blood SupplyDocument10 pagesStomach: Arterial and Venous Blood SupplyBereket temesgenNo ratings yet
- Git AnatomyDocument62 pagesGit AnatomyBimo HarmajiNo ratings yet
- Esophagus & Stomach, Its Blood Supply& Development:: OesophagusDocument8 pagesEsophagus & Stomach, Its Blood Supply& Development:: OesophagusBoody KhalilNo ratings yet
- StomachDocument13 pagesStomachSemNo ratings yet
- 14 StomachDocument24 pages14 Stomachafzal sulemaniNo ratings yet
- 0ac8 PDFDocument17 pages0ac8 PDFRamona MükNo ratings yet
- Small Intestine AnatomyDocument4 pagesSmall Intestine AnatomyMaria Natalie IrwandaNo ratings yet
- Anatomi & Histologi GasterDocument24 pagesAnatomi & Histologi Gastersalvaryn neNo ratings yet
- The Stomach - Structure - Neurovasculature - TeachMeAnatomyDocument4 pagesThe Stomach - Structure - Neurovasculature - TeachMeAnatomyyamanuel25No ratings yet
- 1-Gastric and Duodenal UlcerDocument21 pages1-Gastric and Duodenal UlcerSeceleanu MarianNo ratings yet
- Factors Affecting Clinical Outcomes Among Patients With Esophageal Varices BleedingDocument16 pagesFactors Affecting Clinical Outcomes Among Patients With Esophageal Varices BleedingMohamed ZezoNo ratings yet
- Abdomen Kub Presentation (Autosaved)Document81 pagesAbdomen Kub Presentation (Autosaved)adhikariaashi2004No ratings yet
- Peritoneum and Gastro-Intestinal TractDocument108 pagesPeritoneum and Gastro-Intestinal TractKAYISIRE EMERYNo ratings yet
- 2 Anatomy of The Abdominal VisceraDocument9 pages2 Anatomy of The Abdominal VisceraLinh PhanNo ratings yet
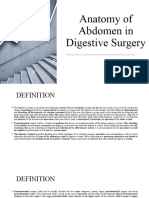
- Anatomy of Abdomen in Digestive SurgeryDocument25 pagesAnatomy of Abdomen in Digestive SurgerymachalliNo ratings yet
- Abdominal Organs Essay SolutionDocument77 pagesAbdominal Organs Essay SolutionEmmanuel IshiomaNo ratings yet
- Anatomy of StomachDocument15 pagesAnatomy of Stomachmedicaleducation2076No ratings yet
- Anatomia de Vesicula BiliarDocument5 pagesAnatomia de Vesicula BiliarHumberto CamposNo ratings yet
- Blok GastrointestinalDocument103 pagesBlok GastrointestinalArLyne MakinNo ratings yet
- STOMACHDocument18 pagesSTOMACHOlaifa victorNo ratings yet
- Lecture StomachDocument31 pagesLecture StomachAmaetenNo ratings yet
- Abdominal Cavity: Peritoneum & GITDocument32 pagesAbdominal Cavity: Peritoneum & GITAli Al-QudsiNo ratings yet
- Digestive SystemDocument106 pagesDigestive Systemshahzaibzafargondal11786No ratings yet
- Nakayama ProcedureDocument6 pagesNakayama ProcedureRosyiidta JanahNo ratings yet
- Anatomy, Lecture 10, Abdominal Cavity 1 (Slides)Document32 pagesAnatomy, Lecture 10, Abdominal Cavity 1 (Slides)Ali Al-Qudsi100% (1)
- Accessory GlandsDocument55 pagesAccessory GlandsMaxamed Faarax XaashiNo ratings yet
- Stomach Esophagus ChymeDocument2 pagesStomach Esophagus ChymeDeryantoNo ratings yet
- 2.3.1 Upper Gastro-Oesophageal SurgeryDocument14 pages2.3.1 Upper Gastro-Oesophageal SurgeryZayan SyedNo ratings yet
- Pa Tho PhysiologyDocument8 pagesPa Tho PhysiologyEitan LopezNo ratings yet
- StomachDocument24 pagesStomachesra1altahirNo ratings yet
- Class 2Document183 pagesClass 2Tanvir AhmedNo ratings yet
- Ana202 - Gross Anatomy of The Abdominal Esophagus Ans Stomach Gross 2021 (Autosaved) (Autosaved)Document45 pagesAna202 - Gross Anatomy of The Abdominal Esophagus Ans Stomach Gross 2021 (Autosaved) (Autosaved)ezekieldare91No ratings yet
- Anatomi Gasttrointestinal FIXDocument79 pagesAnatomi Gasttrointestinal FIXEka TariganNo ratings yet
- 18 IntestinesDocument28 pages18 Intestinesafzal sulemaniNo ratings yet
- 3.02.6.1 Gross Anatomical Relationships: Boron and Boulpaep, 2009Document2 pages3.02.6.1 Gross Anatomical Relationships: Boron and Boulpaep, 2009Oana GușetoaiaNo ratings yet
- Upper GITDocument33 pagesUpper GITWahida Amalin Ab RazakNo ratings yet
- Clinical Anatomy of Abdominal CavityDocument88 pagesClinical Anatomy of Abdominal CavityFahim NadvyNo ratings yet
- Anatomy and Physiology of Stomach.Document4 pagesAnatomy and Physiology of Stomach.Miza HayaniNo ratings yet
- Anatomy of StomachDocument18 pagesAnatomy of StomachAyu NiendarNo ratings yet
- Tizita's Rad Anat of Gu Updated TTDocument134 pagesTizita's Rad Anat of Gu Updated TTleul TizazuNo ratings yet
- Problem 2.03Document12 pagesProblem 2.03DeirdreNo ratings yet
- Radio Logical Anatomy of Esophagus, Stomach, Small by Talat 11-9Document153 pagesRadio Logical Anatomy of Esophagus, Stomach, Small by Talat 11-9dr1mazinNo ratings yet
- Large Intestine BontragerDocument3 pagesLarge Intestine BontragerShofian MadaniNo ratings yet
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Use of Statistics in EpidemiologyDocument30 pagesUse of Statistics in Epidemiologysmaran2meNo ratings yet
- Pocket PediaDocument76 pagesPocket PediaDonna Labaniego100% (1)
- Glossary of Small Ruminant Terminologies: Bulletin II, Vol. IIDocument21 pagesGlossary of Small Ruminant Terminologies: Bulletin II, Vol. IIPiyaNo ratings yet
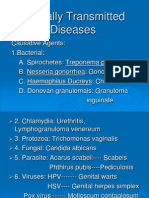
- Sexually Transmitted DiseasesDocument14 pagesSexually Transmitted DiseasesMartha P0% (1)
- My Experiences During The Pandemic TimeDocument2 pagesMy Experiences During The Pandemic TimeDaniel DeniegaNo ratings yet
- NCP 3Document3 pagesNCP 3Grae TaclobNo ratings yet
- Birdflu EbookDocument19 pagesBirdflu EbookandreassuwitoNo ratings yet
- 8a. Typology of Family NursingHealth Problems 2Document2 pages8a. Typology of Family NursingHealth Problems 2Celine PanahonNo ratings yet
- Ulcer Genitalis EllenoDocument2 pagesUlcer Genitalis EllenoGabriela Sabatini GunawanNo ratings yet
- Isolated Glomerular Disease With Recurrent Gross HematuriaDocument17 pagesIsolated Glomerular Disease With Recurrent Gross HematuriaArun GeorgeNo ratings yet
- Developmental Action Plan CHNDocument3 pagesDevelopmental Action Plan CHNRachel Ann BatayolaNo ratings yet
- Understanding The Mechanism of Chikungunya Virus Vector Competence in Three Species of MosquitoesDocument13 pagesUnderstanding The Mechanism of Chikungunya Virus Vector Competence in Three Species of MosquitoesRayssa OliveiraNo ratings yet
- Fordyce SpotsDocument4 pagesFordyce SpotsAnitaPutri100% (2)
- Student's Book Form 4 PDFDocument94 pagesStudent's Book Form 4 PDFAnzimNo ratings yet
- People Before Profit Intermediate Business English Article LessonDocument8 pagesPeople Before Profit Intermediate Business English Article LessonBarbariskovna IriskaNo ratings yet
- Biostatistics and Role in DentistryDocument90 pagesBiostatistics and Role in DentistryJyoti Sharma100% (1)
- Promotive and Preventive Health Aspect in CHN & Facts On Healthcare in PHDocument2 pagesPromotive and Preventive Health Aspect in CHN & Facts On Healthcare in PH2A - Nicole Marrie HonradoNo ratings yet
- Evaluation of Functions of SubcentreDocument16 pagesEvaluation of Functions of SubcentreMohammed Shahnawaz HussainNo ratings yet
- Branches of MicrobiologyDocument2 pagesBranches of MicrobiologyMonika Sharma100% (2)
- 8th Grade Spelling WordsDocument3 pages8th Grade Spelling Wordsgj7g5cd8zjNo ratings yet
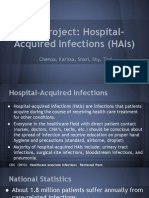
- Qi Project-1Document10 pagesQi Project-1api-245887979No ratings yet
- Examining The PrecordiumDocument83 pagesExamining The PrecordiumnicolNo ratings yet
- Health StudyDocument10 pagesHealth StudyRajeswara Rao NidasanametlaNo ratings yet
- Blood: Symptoms of Dengue FeverDocument7 pagesBlood: Symptoms of Dengue FeverPrincess Viluan PazNo ratings yet
- German Panic Paper 4 - Necessary Measures For Germany To Contain The COVID-19 Pandemic and To Avoid Social Collateral Damage (English)Document9 pagesGerman Panic Paper 4 - Necessary Measures For Germany To Contain The COVID-19 Pandemic and To Avoid Social Collateral Damage (English)MichaelNo ratings yet
- The Quality of Water in Fish Spa With Garra Rufa FishDocument7 pagesThe Quality of Water in Fish Spa With Garra Rufa Fishzagad04No ratings yet
- Understanding The WOB Bar PAVDocument2 pagesUnderstanding The WOB Bar PAVCarlos Julián Ortiz DallosNo ratings yet
- DengueDocument3 pagesDengueNeils MicNo ratings yet