Intussuscept ION: in The Paediatric Patient
Intussuscept ION: in The Paediatric Patient
Download as pptx, pdf, or txt
You might also like
- Esophageal and Gastric VaricesDocument15 pagesEsophageal and Gastric VaricesDumbo D' CatNo ratings yet
- Large Bowel Obstruction by Nic MDocument42 pagesLarge Bowel Obstruction by Nic MRisky OpponentNo ratings yet
- IntussusceptionDocument33 pagesIntussusceptionNovendi RizkaNo ratings yet
- K-25 Acute AppendicitisDocument23 pagesK-25 Acute AppendicitiscarinasheliapNo ratings yet
- Bladder Outlet Obstruction in Children PDFDocument64 pagesBladder Outlet Obstruction in Children PDFalaaNo ratings yet
- Acute Abdomen &peritonitisDocument63 pagesAcute Abdomen &peritonitisSamar Ahmad100% (1)
- Ectopic PregnancyDocument14 pagesEctopic PregnancytaufiqNo ratings yet
- Carcinomagallbladder PDFDocument61 pagesCarcinomagallbladder PDFZaki DhiifNo ratings yet
- By Col - Abrar Hussain ZaidiDocument47 pagesBy Col - Abrar Hussain ZaidiSilvanaPutriNo ratings yet
- Benign Disease of The Genital Tract by Hossam El SokkaryDocument92 pagesBenign Disease of The Genital Tract by Hossam El Sokkarysalah subbahNo ratings yet
- VolvulusDocument38 pagesVolvulusHector RaulNo ratings yet
- Choledochal CystDocument68 pagesCholedochal CystSyed Waqas HasanNo ratings yet
- Placenta Accreta (Or Worse!) : Deward Voss, MD James Pavelka, MDDocument75 pagesPlacenta Accreta (Or Worse!) : Deward Voss, MD James Pavelka, MDYessamin Paith RoderosNo ratings yet
- Burst Abdomen: by DR - SuhaibDocument15 pagesBurst Abdomen: by DR - Suhaibsuhaibrehaman100% (1)
- Intussusception 161007042729 PDFDocument44 pagesIntussusception 161007042729 PDFDina Marselina100% (1)
- Deep Venous ThrombosisDocument56 pagesDeep Venous ThrombosisSrikant Konchada100% (2)
- Benign Gynecological LesionsDocument9 pagesBenign Gynecological LesionsLanceNo ratings yet
- Jaundice in Infants and Children: Ultrasound ClinicsDocument11 pagesJaundice in Infants and Children: Ultrasound Clinics5206329No ratings yet
- Ultrasound Breast ScanningDocument36 pagesUltrasound Breast ScanningPhuntsho Ongmo100% (1)
- Pyloric StenosisDocument14 pagesPyloric Stenosisgangguan hepatobilierNo ratings yet
- Extrahepatic Biliary ObstructionDocument44 pagesExtrahepatic Biliary ObstructionOssama Abd Al-amierNo ratings yet
- Acute PancreatitisDocument46 pagesAcute PancreatitisLew NianNo ratings yet
- Renal Artery StenosisDocument80 pagesRenal Artery StenosisAnn FloydNo ratings yet
- Gastrointestinal ImagingDocument134 pagesGastrointestinal ImagingAnonymous RTSL19BmiNo ratings yet
- Breast Diseases BenignDocument34 pagesBreast Diseases BenignAhmad Uzair Qureshi100% (1)
- Anatomy of The Female Reproductive SystemDocument9 pagesAnatomy of The Female Reproductive SystemPinkeyinthecityNo ratings yet
- 2019 Hernia Kuliah FKDocument50 pages2019 Hernia Kuliah FKKhairani NurhamidahNo ratings yet
- BiliaryDocument23 pagesBiliarytikaauliaNo ratings yet
- Differential Diagnosis of A Renal MassDocument23 pagesDifferential Diagnosis of A Renal Massmdjohari100% (1)
- Hirschsprung's Disease - AthigamanDocument128 pagesHirschsprung's Disease - Athigamanprived100% (4)
- Coursebook-Livertransplant ch27Document53 pagesCoursebook-Livertransplant ch27Сергей СадовниковNo ratings yet
- VASCULAR - Abdominal Aorta Duplex ScanDocument24 pagesVASCULAR - Abdominal Aorta Duplex ScanSophia Elinor MenesesNo ratings yet
- Curs Fetal Abdominal AnomaliesDocument137 pagesCurs Fetal Abdominal AnomaliesCristi SoareceNo ratings yet
- Inguinal Scrotal SwellingsDocument23 pagesInguinal Scrotal SwellingsAzmyza Azmy100% (1)
- 03-First Trimester UsgDocument103 pages03-First Trimester UsgBharti Pant GahtoriNo ratings yet
- Abdominal Pain in ChildrenDocument48 pagesAbdominal Pain in ChildrenSurin Jayawardene100% (1)
- Gynecoloical Ultrasound Doppler AssessmentDocument17 pagesGynecoloical Ultrasound Doppler AssessmentKinzaNo ratings yet
- Thyroid GlandDocument81 pagesThyroid Glanddr_shamimrNo ratings yet
- Multifetalpregnancy 121008074609 Phpapp02Document38 pagesMultifetalpregnancy 121008074609 Phpapp02Jagannath MaaleNo ratings yet
- Omphalocele Omphalocele: Perceptor: DR. AMRAN SINAGA, SP.B AUTHOR: Ida Ayu Ratna W, S.Ked (G1A214018)Document17 pagesOmphalocele Omphalocele: Perceptor: DR. AMRAN SINAGA, SP.B AUTHOR: Ida Ayu Ratna W, S.Ked (G1A214018)Rully Riyan DikaNo ratings yet
- Testicular Tumours 2020Document55 pagesTesticular Tumours 2020Ramesh ReddyNo ratings yet
- Ultrasonography AssignmentDocument5 pagesUltrasonography AssignmentAkshay VasishtaNo ratings yet
- Pyloric StenosisDocument23 pagesPyloric StenosisRama ItachiNo ratings yet
- Vaginal Bleeding in Late PregnancyDocument139 pagesVaginal Bleeding in Late PregnancygibreilNo ratings yet
- Hernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsDocument43 pagesHernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsFobin VargheseNo ratings yet
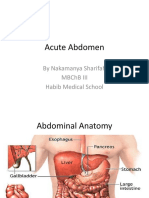
- Acute Abdomen: by Nakamanya Sharifah MBCHB Iii Habib Medical SchoolDocument48 pagesAcute Abdomen: by Nakamanya Sharifah MBCHB Iii Habib Medical SchoolNina100% (1)
- Cystic LesionsDocument101 pagesCystic LesionsKartik GuptaNo ratings yet
- Colonoscopi IndicationDocument26 pagesColonoscopi IndicationTony HardianNo ratings yet
- Minimally Invasive AdrenalectomyDocument14 pagesMinimally Invasive AdrenalectomyTJ LapuzNo ratings yet
- Fetal Growth Restriction - ACOG 2019Document23 pagesFetal Growth Restriction - ACOG 2019Adhitya Yudha Maulana100% (1)
- Lecture 6 Breach Presentation Transversal Oblique LieDocument51 pagesLecture 6 Breach Presentation Transversal Oblique Lietanmai nooluNo ratings yet
- Abdomen ExaminationDocument37 pagesAbdomen ExaminationJaaydevNo ratings yet
- Portal Hypertension SurgeryDocument6 pagesPortal Hypertension SurgeryjackSNMMCNo ratings yet
- EdemaDocument27 pagesEdemarapadilNo ratings yet
- Intestinal Obstruction in Paediatrics - James GathogoDocument21 pagesIntestinal Obstruction in Paediatrics - James GathogoMalueth Angui100% (2)
- Nursing Process OsteosarcomaDocument34 pagesNursing Process OsteosarcomaDonJohnNo ratings yet
- Benign Gyne LesionsDocument133 pagesBenign Gyne LesionsJulie Ann ValenciaNo ratings yet
- The Ultimate Guide to Vascular Ultrasound: Diagnosing and Understanding Vascular ConditionsFrom EverandThe Ultimate Guide to Vascular Ultrasound: Diagnosing and Understanding Vascular ConditionsNo ratings yet
- 2-Acute Abdominal PainDocument24 pages2-Acute Abdominal Painabdalmajeed alshammaryNo ratings yet
- Intussuscept ION: in The Paediatric PatientDocument30 pagesIntussuscept ION: in The Paediatric PatientSuneil R AlsNo ratings yet
- A Case of Iron Deficiency Anemia - Draft 1Document2 pagesA Case of Iron Deficiency Anemia - Draft 1Suneil R AlsNo ratings yet
- Viral Hepatitis: Juliana Chan, Pharm.DDocument26 pagesViral Hepatitis: Juliana Chan, Pharm.DSuneil R AlsNo ratings yet
- Serious Hazards of Transfusion: DR Kenneth S Charles MB - Bs (Uwi), FRCP (Uk), Frcpath (Uk) Senior Lecturer in HaematologyDocument65 pagesSerious Hazards of Transfusion: DR Kenneth S Charles MB - Bs (Uwi), FRCP (Uk), Frcpath (Uk) Senior Lecturer in HaematologySuneil R AlsNo ratings yet
- May-June 2003 P2 Q2Document2 pagesMay-June 2003 P2 Q2Suneil R Als47% (15)