Impulse Disorders
Impulse Disorders
Download as ppt, pdf, or txt
You might also like
- Getting Ready To Test SupplementDocument138 pagesGetting Ready To Test SupplementIan Cloudy60% (5)
- Book Identifying Negative Core Beilefs For Clearing1Document3 pagesBook Identifying Negative Core Beilefs For Clearing1Brooke Pena75% (4)
- CAARS ManualDocument39 pagesCAARS Manualkay jonesNo ratings yet
- Conduct DisorderDocument14 pagesConduct Disorderima100% (2)
- Child Welfare Trauma Referral ToolDocument10 pagesChild Welfare Trauma Referral ToolErin CooperNo ratings yet
- Case StudyDocument14 pagesCase Studyaaliyah100% (1)
- PTSD Research PaperDocument4 pagesPTSD Research PapergraceNo ratings yet
- Social Anxiety Disorder (Social Phobia) PDFDocument29 pagesSocial Anxiety Disorder (Social Phobia) PDFMuhammad NabeelNo ratings yet
- Suggestive TherapeuticsDocument3 pagesSuggestive TherapeuticsHelena Espirito SantoNo ratings yet
- Posttraumatic Stress DisorderDocument11 pagesPosttraumatic Stress DisorderJolson123No ratings yet
- Mpce-11 2023Document16 pagesMpce-11 2023xicacol947No ratings yet
- P T S DisorderDocument10 pagesP T S Disordersp2056251No ratings yet
- PTSDDocument3 pagesPTSDswastikakar28No ratings yet
- PTSDsDocument41 pagesPTSDsBabul BanerjeeNo ratings yet
- Panic Attacks and Panic DisorderDocument3 pagesPanic Attacks and Panic DisorderRoci ArceNo ratings yet
- Trauma Concept PaperDocument7 pagesTrauma Concept Paperapi-226804663No ratings yet
- NIMH Post-Traumatic Stress DisorderDocument8 pagesNIMH Post-Traumatic Stress DisorderBuon GiornoNo ratings yet
- E Disorder: Posttraumatic Stress Umatic Stress DisorderDocument7 pagesE Disorder: Posttraumatic Stress Umatic Stress DisorderMelly T CiakraNo ratings yet
- PTSDDocument4 pagesPTSDAzim Arif HashmiNo ratings yet
- PMH Panic DisorderDocument19 pagesPMH Panic Disorderycq5s9jdgnNo ratings yet
- CHP 3Document9 pagesCHP 3MR ZalimNo ratings yet
- Post Traumatic Stress Disorder (PTSD)Document4 pagesPost Traumatic Stress Disorder (PTSD)Samreen Jawaid100% (1)
- World Psychiatry - 2019 - Bryant - Post Traumatic Stress Disorder A State of The Art Review of Evidence and ChallengesDocument11 pagesWorld Psychiatry - 2019 - Bryant - Post Traumatic Stress Disorder A State of The Art Review of Evidence and ChallengesHesti Juwita P.No ratings yet
- Practice Essentials: Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)Document20 pagesPractice Essentials: Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)Anonymous 2ernTkNo ratings yet
- PTSDDocument21 pagesPTSDsachinkumarmalra792000No ratings yet
- PTSD and Crime Victimization - PPTDocument42 pagesPTSD and Crime Victimization - PPTVictoria HarganNo ratings yet
- Materi Penkes JiwaDocument15 pagesMateri Penkes JiwaNursezya W. DaudNo ratings yet
- PTSD EssayDocument10 pagesPTSD Essayapi-549243920No ratings yet
- What Is Post Traumatic Stress DiorderDocument3 pagesWhat Is Post Traumatic Stress DiorderperezNo ratings yet
- PTSDDocument7 pagesPTSDadeNo ratings yet
- Brief Psychotic DisorderDocument3 pagesBrief Psychotic DisorderEugenio CainghugNo ratings yet
- Difference Between PTSD and Developmental/Complex TraumaDocument10 pagesDifference Between PTSD and Developmental/Complex Traumaaqib aliNo ratings yet
- NeedtoknowDocument2 pagesNeedtoknowapi-306018641No ratings yet
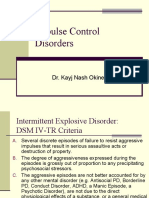
- Impulse Control Disorders: Dr. Kayj Nash OkineDocument18 pagesImpulse Control Disorders: Dr. Kayj Nash OkineDivya ThomasNo ratings yet
- Post-Traumatic Stress Disorder (PTSD) - Symptoms and Causes - Mayo ClinicDocument1 pagePost-Traumatic Stress Disorder (PTSD) - Symptoms and Causes - Mayo ClinicJoyce GarciaNo ratings yet
- Panic Disorder Research PaperDocument6 pagesPanic Disorder Research PaperDisha AgarwalNo ratings yet
- Pyromania Disorder Symptoms, Causes, Diagnosis, and TreatmentDocument1 pagePyromania Disorder Symptoms, Causes, Diagnosis, and TreatmentO MiranhaNo ratings yet
- Conversion Disorder Hysterical NeurosisDocument4 pagesConversion Disorder Hysterical NeurosisrianachuNo ratings yet
- What Is Post-Traumatic Stress Disorder, or PTSD?Document8 pagesWhat Is Post-Traumatic Stress Disorder, or PTSD?Hakim HashimNo ratings yet
- Post-Traumatic Stress Disorder (PTSD)Document2 pagesPost-Traumatic Stress Disorder (PTSD)Kwaku OhemengNo ratings yet
- PTSDDocument8 pagesPTSDasma khalidNo ratings yet
- Leerdocument DMHDocument42 pagesLeerdocument DMHFlorien BuitendijkNo ratings yet
- USMLE Step 2 CK: CMS: Psychiatry Form 3Document17 pagesUSMLE Step 2 CK: CMS: Psychiatry Form 3usmleaddict pro63% (8)
- Post-Traumatic Stress Disorder: ... Once Called Shell Shock or Battle Fatigue SyndromeDocument7 pagesPost-Traumatic Stress Disorder: ... Once Called Shell Shock or Battle Fatigue SyndromeJake CastañedaNo ratings yet
- PTSD PresentationDocument21 pagesPTSD Presentationmiyahb2007No ratings yet
- Apa - DSM 5 PTSD PDFDocument2 pagesApa - DSM 5 PTSD PDFoktaviana54100% (1)
- Trauma Survivor's Guide to Coping with Panic Attacks: Focusing on Panic Associated with PTSD and cPTSDFrom EverandTrauma Survivor's Guide to Coping with Panic Attacks: Focusing on Panic Associated with PTSD and cPTSDNo ratings yet
- Post Traumatic Stress DisorderDocument4 pagesPost Traumatic Stress DisorderaploureyNo ratings yet
- PsychopathologyDocument24 pagesPsychopathologyamulya anandNo ratings yet
- Depression and Bipolar DisordersDocument20 pagesDepression and Bipolar DisordersRavi Paul100% (1)
- Post Traumatic Stress DisorderDocument7 pagesPost Traumatic Stress Disordersomebody_maNo ratings yet
- Posttraumatic Stress Disorder and Acute Stress DisorderDocument42 pagesPosttraumatic Stress Disorder and Acute Stress DisorderPIH SHTNo ratings yet
- Pshcology AssignmentDocument5 pagesPshcology AssignmentAbdul MoizNo ratings yet
- Guaranteed Cognitive Behavioral Treatment (CBT) Simple Steps to Overcome Anxiety, Depression, Fear and Anger in WomenFrom EverandGuaranteed Cognitive Behavioral Treatment (CBT) Simple Steps to Overcome Anxiety, Depression, Fear and Anger in WomenNo ratings yet
- What Are The Signs and Symptoms of PTSDDocument3 pagesWhat Are The Signs and Symptoms of PTSDzlibrary302No ratings yet
- Post-Traumatic Stress DisorderDocument18 pagesPost-Traumatic Stress DisorderRenee FryeNo ratings yet
- Happiness, Depression and Self-Concept - PsychologyDocument179 pagesHappiness, Depression and Self-Concept - PsychologyHiba Al-Swaid100% (1)
- Post-Traumatic Stress Disorder: National Institute of Mental HealthDocument8 pagesPost-Traumatic Stress Disorder: National Institute of Mental HealthAndra AndruNo ratings yet
- Impulse ControlDocument16 pagesImpulse ControlimaNo ratings yet
- Kleptomania: By: Jasmin LeonDocument10 pagesKleptomania: By: Jasmin Leonkareem92No ratings yet
- Wa0030.Document3 pagesWa0030.Marianela PatillaNo ratings yet
- CRIS 304 Module 1 NotesDocument10 pagesCRIS 304 Module 1 NotesDee Heun GlaunerNo ratings yet
- Post Traumatic Stress DisorderDocument23 pagesPost Traumatic Stress DisorderMuhammad Taufiqul HadiNo ratings yet
- Anxiety Disorders: Nagy Ghattas Henein Ass. Lecturer, NeuropsychiatryDocument39 pagesAnxiety Disorders: Nagy Ghattas Henein Ass. Lecturer, NeuropsychiatryNagy ShenodaNo ratings yet
- Overcoming PTSD: The workbook designed to help you understand and overcome post-traumatic stress disorderFrom EverandOvercoming PTSD: The workbook designed to help you understand and overcome post-traumatic stress disorderNo ratings yet
- 78 Rotavirus PDFDocument4 pages78 Rotavirus PDFimaNo ratings yet
- YMRSDocument2 pagesYMRSimaNo ratings yet
- Impulse ControlDocument16 pagesImpulse ControlimaNo ratings yet
- Eating Disorder Among TeenagersDocument14 pagesEating Disorder Among TeenagersReese CorpuzNo ratings yet
- Back From The Bluez - 09 - Self ManagementDocument5 pagesBack From The Bluez - 09 - Self ManagementMelanie DovaleNo ratings yet
- Psychology Individual AssignmentDocument3 pagesPsychology Individual AssignmentKale'ab LemmaNo ratings yet
- Healing TR Auma: A Brief Intervention For WomenDocument8 pagesHealing TR Auma: A Brief Intervention For WomenAsmaa El-emairyNo ratings yet
- Rollo May - Freedom and DestinyDocument231 pagesRollo May - Freedom and DestinyRaluca Elena100% (1)
- Medical Management SchizoDocument3 pagesMedical Management SchizoPatricia Vergara AlbiolaNo ratings yet
- A List of Psychological DisordersDocument12 pagesA List of Psychological DisordersGaurav LahotiNo ratings yet
- ن مقرر علم النفس التأهيليDocument38 pagesن مقرر علم النفس التأهيليZEINABNo ratings yet
- Aluma Center:: 1. Providing Therapy and Consultation On All Levels: Individual, Couple, Family and GroupDocument4 pagesAluma Center:: 1. Providing Therapy and Consultation On All Levels: Individual, Couple, Family and Groupאורלי רוביןNo ratings yet
- Hare Psychopathy Checklist ReviewedDocument7 pagesHare Psychopathy Checklist Reviewedraluca_ghigaNo ratings yet
- Family-Alcohol ReviewDocument19 pagesFamily-Alcohol ReviewErma89No ratings yet
- Outcome and Outcome Indicator BanksDocument29 pagesOutcome and Outcome Indicator BanksImprovingSupportNo ratings yet
- 3 Faces of Eve Results TableDocument2 pages3 Faces of Eve Results Tableapi-247243068No ratings yet
- CAMH-Course-Brochure-2024 1Document2 pagesCAMH-Course-Brochure-2024 1suvaran sagar bajpaiNo ratings yet
- Case PresentationDocument9 pagesCase Presentationapi-637050088No ratings yet
- J 1545-5300 1962 00015 XDocument7 pagesJ 1545-5300 1962 00015 XFausto Adrián Rodríguez LópezNo ratings yet
- Psyc 331 Exam 2 Study GuideDocument2 pagesPsyc 331 Exam 2 Study GuidedivssssssNo ratings yet
- Group TherapyDocument27 pagesGroup TherapyDr. Jayesh Patidar100% (5)
- The Effectiveness of Psychodynamic Psychotherapies - An Update (2015) PDFDocument14 pagesThe Effectiveness of Psychodynamic Psychotherapies - An Update (2015) PDFmysticmdNo ratings yet
- Mental Illnes in MalaysiaDocument4 pagesMental Illnes in MalaysiaZikkru ThaqibNo ratings yet
- Introduction To Family Mental Health: MK Kesehatan Mental KeluargaDocument14 pagesIntroduction To Family Mental Health: MK Kesehatan Mental KeluargaDamar Adhi PrakosoNo ratings yet
- Mental Health, Psychosocial Support Services and Psychological First AidDocument102 pagesMental Health, Psychosocial Support Services and Psychological First AidDonna Flor Nabua50% (2)
- Rwilliams Personal Position PaperDocument29 pagesRwilliams Personal Position Paperapi-231978749No ratings yet
- Stress-Test - 3Document2 pagesStress-Test - 3api-491070484No ratings yet