The document provides information on three mosquito-borne diseases: Zika virus, dengue fever, and malaria. It describes the signs and symptoms of each disease, how they are transmitted, their incubation periods, diagnostic testing and treatment approaches. For nursing management, it emphasizes monitoring patients, providing comfort measures, educating on prevention of transmission and watching for complications. The primary focus is on assessment and care of patients experiencing these tropical diseases.
The document provides information on three mosquito-borne diseases: Zika virus, dengue fever, and malaria. It describes the signs and symptoms of each disease, how they are transmitted, their incubation periods, diagnostic testing and treatment approaches. For nursing management, it emphasizes monitoring patients, providing comfort measures, educating on prevention of transmission and watching for complications. The primary focus is on assessment and care of patients experiencing these tropical diseases.
The document provides information on three mosquito-borne diseases: Zika virus, dengue fever, and malaria. It describes the signs and symptoms of each disease, how they are transmitted, their incubation periods, diagnostic testing and treatment approaches. For nursing management, it emphasizes monitoring patients, providing comfort measures, educating on prevention of transmission and watching for complications. The primary focus is on assessment and care of patients experiencing these tropical diseases.
The document provides information on three mosquito-borne diseases: Zika virus, dengue fever, and malaria. It describes the signs and symptoms of each disease, how they are transmitted, their incubation periods, diagnostic testing and treatment approaches. For nursing management, it emphasizes monitoring patients, providing comfort measures, educating on prevention of transmission and watching for complications. The primary focus is on assessment and care of patients experiencing these tropical diseases.
Download as PPTX, PDF, TXT or read online from Scribd
Download as pptx, pdf, or txt
You are on page 1/ 24
Gil P.
Soriano, RN, MHPEd
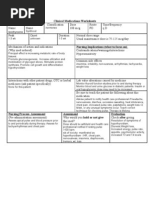
Zika Virus Dengue Fever Malaria is spread mostly by the bite of an infected Aedes species mosquito (Aedes aegypti and Aedes albopticus) that bites during the day and night. It can be passed from a pregnant woman to her fetus. Infection during pregnancy can cause certain birth defects. There is no vaccine or medicine for Zika.
Incubation Period 3 to 12 days Mode of Transmission Bite of an infected mosquito Sexual contact Vertical transmission Blood transfusion
Diagnosis Presence of Zika virus in the blood, urine and saliva of infected person Serologic testing PCR Treatment Symptomatic
Nursing Management Provide comfort measure to patient Instruct to increase oral fluid intake of patients Give analgesics to reduce fever and pain except aspirin and other non-steroidal anti-inflammatory drugs (NSAIDS) until dengue can be ruled out to reduce the risk of bleeding. Complication Guillain-Barre syndrome aka Breakbone fever, Hemorrhagic fever, Dandy fever, Infectious Thrombocytopenic Purpura
Acute febrile disease caused by infection with one of the serotypes
of dengue virus, Etiologic Agent/Vector Flaviviruses 1, 2, 3, 4, a family of togaviridae
Incubation Period 3 to 14 days Bite of an infected mosquito, principally Aedes aegypti Aedes aegypti is a day-biting mosquito (they appear two hours after sunrise and two hours before sunset) It breeds in areas of stagnant water It has limited, low-flying movement It has fine white dots at the base of the wings and white bands on the legs
Aedes albopticus may contribute to the transmission of the dengue virus in rural areas Other contributory mosquitoes: Aedes polynensis Aedes scutellaris simplex Period of Communicability Patients are usually infective to the mosquito from a day before the febrile period to the end of it. The mosquito becomes infected from day 8 to 12 after the blood meal and remains infective throughout its life
Sources of Infection Infected Persons-the virus is present in the blood of patients during the acute phase of the disease and will become a reservoir of the virus, sucked by mosquitoes, which may then transmit the disease Standing Water-any stagnant water in the household and its premises are usual breeding places of these mosquitoes
Incidence Age-occur at any stage, but common among children and peaks between four to nine years old Sex-Both sexes can be affected Season-It is more frequent during the rainy season Location-Dengue fever is more prevalent in urban communities DENGUE IS AN ALL YEAR ROUND DISEASE IN THE PHILIPPINES.
MARCH OF 2012, DOH RELEASED
ADMINISTRATIVE ORDER NO. 2012-0006 OR THE REVISED DENGUE CLINICAL CASE MANAGEMENT GUIDELINES 2011. DENGUE WITHOUT WARNING SIGNS Probable Dengue: Confirmed Dengue Lives in or travels to dengue-endemic Viral culture isolation Polymerase Chain area, with fever, plus any two of the Reaction following: a) Headache b) Body malaise c) Myalgia d) Arthralgia e) Retro-orbital pain f) Anorexia g) Nausea h) Vomiting i) Diarrhea j) Flushed skin k) Rash AND Laboratory test, at least CBC (leukopenia with or without thrombocytopenia) and/or dengue NS1 Antigen test or dengue 1gM anti-body test (optional) DENGUE WITH WARNING SIGNS SEVERE DENGUE
Lives in or travel to dengue Lives in or travel to dengue
endemic area, with fever lasting endemic area, with fever lasting 2-7 days, plus any of the 2-7 days, plus any of the above following: clinical manifestations for Abdominal pain dengue with or without warning Tenderness signs plus any of the following: Persistent vomiting Severe plasma leakage leading to Clinical signs of fluid accumulation shock or fluid accumulation with Mucosal bleeding respiratory distress, severe Lethargy bleeding severe organ impairment: Restlessness Liver AST or ALT> or equal to Liver enlargement 1000, CNS- seizures, impaired Laboratory: increase in Hematocrit consciousness. decreasing platelet count. Heart-myocarditis, kidneys-renal failure. Diagnostic Test Torniquet test Platelet count Hemoconcentration Occult Blood Hgd determination
Treatment Symptomatic Analgesic except aspirin IV therapy Blood transfusion Oxygen therapy Sedatives Take the patient's blood pressure and record it, for example, 100/70. Inflate the cuff to a point midway between SBP and DBP, and maintain for 5 minutes, (100 + 70) 2 = 85 mm Hg Reduce and wait 2 minutes. Count petechiae below antecubital fossa. - A positive test is 10 or more petechiae per 1 square inch. Patient should be kept in a mosquito-free environment to avoid further transmission of infection Keep patient at rest during bleeding episodes Monitoring of vital signs Observe for signs of shock, such as slow pulse, cold, clammy skin, prostration and fall of blood pressure Trendelenburg position to provide greater blood volume to the head part Isolation is not required Nursing Diagnosis Altered body temperature Fear Anxiety Knowledge deficit Activity intolerance
Prevention Health education Early detection and treatment Treat mosquito nets with insecticides House spraying is advised Eliminate vector by: Changing water and scrubbing sides of flower vases once a week Destroy breeding places of mosquitoes by cleaning surroundings Keeping the water container covered Avoid hanging too many clothes inside the house Case finding Dengue hemorrhagic fever Metabolic acidosis Hyperkalemia Tissue anoxia Hemorrhage into the CNS or adrenal glands Uterine bleeding may occur Myocarditis
Dengue encephalopathy Increase restlessness Apprehension Disturbed sensorium Convulsions Hyporeflexia Is an acute and chronic parasitic disease transmitted by the bite of mosquitoes and in confined mainly to tropical and subtropical areas
Etiologic Agent Protozoa of genus plasmodia Plasmodium falciparum (malignant tertian)- most serious malarial infection and most common in the Philippines Plasmodium vivax (benign tertian)- non-life threatening except for the very young and very old, manifested by chills every 48 hours on the 3rd day and onward especially if untreated Plasmodium malariae (quartan)- less frequently seen, non-life threatening, fever and chills occur every 72 hours usually on the 4th day after onset Plasmodium ovale-rare type of specie Plasmodium knowlesi- Found in South-East Asia and causes malaria in lon- tailed macaques (Macaca fascicularis), but it may also infect humans, either naturally or artificially. Vector is female Anopheles mosquito Breeds in clear, flowing and shaded streams, usually in the mountains Bigger in size than ordinary mosquitoes Brown in color, night-biting mosquito Does not bite a person in motion Assumes a 36 degree position on walls, trees, curtains and the like
Incubation Period 12 days for P. falciparum and P. knowlesi 14 days for P. vivax and ovale 30 days for P. malariae
Period of Communicability An untreated or insufficiently treated may be the source of mosquito infection for more than 3 years in P. malariae, 1 to 2 years in P. vivax and not more than 1 year in P. falciparum Mode of Transmission Bite of infected female Anopheles mosquito It can be transmitted parenterally through blood transfusion On rare occasions, it is transmitted from share contaminated needles Vertical transmission is a rare case
Clinical Manifestation Paroxysms with shaking chills Rapidly rising fever with severe headache Profuse sweating Myalgia, with feelings of well-being in between Splenomegaly, hepatomegaly Orthostatic hypotension Paroxysms may last for 12 hours and may attack daily or every 2 days In children Fever may be continuous, convulsions and GIT symptoms are prominent and splenomegaly is present In cerebral malaria Severe headache, vomiting and changes in sensorium and Jacksonian or grand mal seizure may occur Diagnosis Malarial smear Rapid Diagnostic Test Treatment Anti-malarial drugs Chloroquine Quinine Sulfadoxine for the resistant P. falciparum Primaquine for relapses of P. vivax and ovale Erythrocyte exchange transfusion for rapid production of high levels or parasites in the blood Nursing Management Close monitoring, take note of I and O to prevent pulmonary edema Daily monitoring of patients serum albumin, BUN, creatinine and parasitic count Determine ABG and plasma electrolyte TSB, alcohol rubs and ice cap on the head help bring temperature down Application of external heat and hot drinks during the chilling stage are helpful Provide comfort and psychological support Encourage the patient to take plenty of fluids Watch for neurologic toxicity like muscular twitching, delirium, confusion, convulsion and coma Evaluate the degree of anemia Wof signs of bleeding Nursing Diagnosis Altered body temperature Activity intolerance Knowledge deficit Altered nutrition: less than body requirement Prevention and Control Case reporting and case finding Destruction of breeding sites Spraying of insecticides at home Mosquito nets should be used Insect repellents People living in malaria infested areas should not donate blood for at least 3 years Blood screening Mondejar-Navales, D. (2014). Handbook of Common Communicable and Infectious Diseases. South Triangle, Quezon City: C & E Publishing, Inc. Smeltzer, S., Bare, B., Hinkle, J. & Cheever. (2008). Brunner & Suddarths Textbook of Medical-Surgical Nursing. Lippincott William & Wilkins Kwann-Gett, T., Kemp, C. & Kovarik, C. (2009). Infectious and Tropical Diseases: A Handbook for Primary Care. Singapore: Mosby Elsevier