OPHTHA Case Report Diabetic Retinopathy
OPHTHA Case Report Diabetic Retinopathy
Download as pptx, pdf, or txt
You might also like
- Lesson 1Document8 pagesLesson 1Random RandomNo ratings yet
- Measuring Disease: Ann BowlingDocument35 pagesMeasuring Disease: Ann BowlingAshraf Uddin Ahmed100% (1)
- Diabetic Emergencies: Click To Edit Master Subtitle StyleDocument22 pagesDiabetic Emergencies: Click To Edit Master Subtitle Stylenaven100% (1)
- NutritionDocument31 pagesNutritionzoltan2014No ratings yet
- Reading Review TOEFL Exercise (Skill 1 - 7)Document2 pagesReading Review TOEFL Exercise (Skill 1 - 7)LussyAlbayinnah100% (1)
- Gestational DiabetesDocument14 pagesGestational Diabetesamena mahmoudNo ratings yet
- AMBLYOPIADocument54 pagesAMBLYOPIAMolde DedekNo ratings yet
- IRIS Pocket Guide To CKD PDFDocument3 pagesIRIS Pocket Guide To CKD PDFJMilena2028No ratings yet
- Prepared By: Manisha Thapa Leeza ShresthaDocument12 pagesPrepared By: Manisha Thapa Leeza ShresthaManjesh Mishra XettriNo ratings yet
- Therapeutic Diet PDFDocument3 pagesTherapeutic Diet PDFJagveer ChauhanNo ratings yet
- BuscopanDocument3 pagesBuscopansukiyem89No ratings yet
- Advantages of Breast FeedingDocument6 pagesAdvantages of Breast Feedingmarck_cahiganNo ratings yet
- Retinoblastoma Case PresentationDocument40 pagesRetinoblastoma Case PresentationsjvikasNo ratings yet
- 128 Diabetic KetoacidosisDocument9 pages128 Diabetic KetoacidosisDite Bayu NugrohoNo ratings yet
- Comparison Between Maltofer-Iberet-Zincofer TAMBAHANDocument4 pagesComparison Between Maltofer-Iberet-Zincofer TAMBAHANhomesweethomestaytciNo ratings yet
- Nursing Care of A Family When A Child Has Gastrointestinal DisorderDocument3 pagesNursing Care of A Family When A Child Has Gastrointestinal DisorderIan BathanNo ratings yet
- Treatment in Childhood DiarrhoeaDocument17 pagesTreatment in Childhood DiarrhoeaPrabir Kumar ChatterjeeNo ratings yet
- Guideline For Empanelment of Hospital Under MA Yojana PDFDocument43 pagesGuideline For Empanelment of Hospital Under MA Yojana PDFVijay BaldaniyaNo ratings yet
- Duphaston PDFDocument4 pagesDuphaston PDFmarcusjanaNo ratings yet
- PROMDocument21 pagesPROMJanelle Lois EscolanoNo ratings yet
- Anemia During PregnancyDocument15 pagesAnemia During PregnancyKuleshwar SahuNo ratings yet
- Diabetes Mellitus: Dr. Madhusudan SwarnkarDocument45 pagesDiabetes Mellitus: Dr. Madhusudan Swarnkarmadhusudan swarnkarNo ratings yet
- DIabetic REtinopathyDocument34 pagesDIabetic REtinopathyLuqman Khan YousafXaiNo ratings yet
- MarasmusDocument1 pageMarasmusNovilee MartinezNo ratings yet
- Endometrial Polyps: Irregular Menstrual BleedingDocument4 pagesEndometrial Polyps: Irregular Menstrual BleedingLuke ObusanNo ratings yet
- Anaemia in Pregnancy md3 MhsDocument26 pagesAnaemia in Pregnancy md3 MhsjerrydanfordfxNo ratings yet
- Diabetic EmergenciesDocument35 pagesDiabetic EmergenciesotiafrancissavioNo ratings yet
- By B. Shalini Under The Guidance of Neelakant Reddy Patil M.PharmDocument25 pagesBy B. Shalini Under The Guidance of Neelakant Reddy Patil M.PharmShalini Reddy100% (1)
- Nursing College Address Etc.Document4 pagesNursing College Address Etc.ParvezNo ratings yet
- LeukorrheaDocument29 pagesLeukorrheaThorsang Chayovan100% (1)
- Intra OcularTumoursDocument35 pagesIntra OcularTumoursdrvishalkulkarni2007100% (1)
- TizanidineDocument2 pagesTizanidinebhawanisrNo ratings yet
- Idiopathic Thrombocytopenic Purpura: Overview With Report of A CaseDocument4 pagesIdiopathic Thrombocytopenic Purpura: Overview With Report of A CaseHernan GonzalezNo ratings yet
- 2 Management of Menorrhagia (Heavy Menstrual Bleeding)Document36 pages2 Management of Menorrhagia (Heavy Menstrual Bleeding)Malak Ahmed 2295No ratings yet
- CaffeineDocument2 pagesCaffeineSaini Malkeet100% (1)
- Esophageal VaricesDocument4 pagesEsophageal VaricesSnapeSnapeNo ratings yet
- Consensus Statement: Management of Idiopathic Nephrotic Syndrome in ChildhoodDocument14 pagesConsensus Statement: Management of Idiopathic Nephrotic Syndrome in Childhoodbendot29No ratings yet
- Imperforate AnusDocument2 pagesImperforate AnusTeofista Bartolome100% (1)
- Diabetic Retinopathy - Aetiopathogenesis, Clinical Presentation andDocument83 pagesDiabetic Retinopathy - Aetiopathogenesis, Clinical Presentation andOlayemi Olorundare0% (1)
- Anemia in ChildrenDocument4 pagesAnemia in ChildrenTeslim Raji100% (2)
- Complete Cholelithiasis Case AnalysisDocument18 pagesComplete Cholelithiasis Case AnalysisAllyssa AnastacioNo ratings yet
- Definition of Placenta PreviaDocument3 pagesDefinition of Placenta Previashan6ersNo ratings yet
- Meconium Plug and NECDocument28 pagesMeconium Plug and NECRon Christian Neil RodriguezNo ratings yet
- Urinary Incontinence in Elderly: DefinitionDocument13 pagesUrinary Incontinence in Elderly: DefinitionTarek AhmedNo ratings yet
- Prune Belly SyndromeDocument25 pagesPrune Belly SyndromeBrian ElinardsNo ratings yet
- Essentials of ObstetricsDocument2 pagesEssentials of Obstetricsmkm050923No ratings yet
- TB TreatmentDocument58 pagesTB TreatmentNdayisaba CorneilleNo ratings yet
- Vitamin A DeficiencyDocument16 pagesVitamin A DeficiencyNikhil ShresthaNo ratings yet
- Prevention of Dental Caries: Name:Huda Khan ROLL #: 753Document33 pagesPrevention of Dental Caries: Name:Huda Khan ROLL #: 753Hudh HudNo ratings yet
- Toxic Multinodular Goiter Physical ExaminationDocument2 pagesToxic Multinodular Goiter Physical ExaminationAngie MandeoyaNo ratings yet
- Budd Chiari SyndromeDocument37 pagesBudd Chiari SyndromeNader SaadNo ratings yet
- Lorazepam - Wikipedia, The Free EncyclopediaDocument15 pagesLorazepam - Wikipedia, The Free Encyclopediaapi-18997839No ratings yet
- Chronic Kidney Disease Sec. Type 2 DiabetesDocument38 pagesChronic Kidney Disease Sec. Type 2 DiabetesRenzel MurrayNo ratings yet
- Failure To ThriveDocument2 pagesFailure To Thrivekafosid100% (1)
- TBL (Miscarrriage)Document36 pagesTBL (Miscarrriage)hitsugayat_7100% (1)
- Case Presentation CKDDocument35 pagesCase Presentation CKDKojo EgyirNo ratings yet
- Diabetic EmergencyDocument28 pagesDiabetic Emergencychandrima pattadarNo ratings yet
- Gestational Diabetes Mellitus (GDM)Document24 pagesGestational Diabetes Mellitus (GDM)asyrafali93No ratings yet
- PI DuphalacDocument2 pagesPI Duphalacabin prakashNo ratings yet
- Antara Provider LeafletDocument2 pagesAntara Provider Leafletganapa247No ratings yet
- Alagille Syndrome FinalDocument54 pagesAlagille Syndrome FinalAlabi Victor Olukayode100% (1)
- Acute GlomerulonephritisDocument9 pagesAcute GlomerulonephritisAESTHETIC PHOTONo ratings yet
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- Optic Neuritis Clinical Practice GuidelineDocument6 pagesOptic Neuritis Clinical Practice GuidelineGufront MustofaNo ratings yet
- Grand Conference: Clinical Clerks Openiano, Oquendo, Pasaporte, PangandianDocument65 pagesGrand Conference: Clinical Clerks Openiano, Oquendo, Pasaporte, PangandianJessa MeaNo ratings yet
- Nephrotic and Nephritic SyndromeDocument52 pagesNephrotic and Nephritic SyndromeJessa MeaNo ratings yet
- Gunshot WoundsDocument22 pagesGunshot WoundsJessa Mea100% (1)
- PhilHealth For Kidney Stone RemovalDocument1 pagePhilHealth For Kidney Stone RemovalJessa MeaNo ratings yet
- The Meeting of Two Diving TraditionsDocument7 pagesThe Meeting of Two Diving TraditionsJessa MeaNo ratings yet
- Environment: Aparta, Auman, Del Castillo, Reas, SisoDocument18 pagesEnvironment: Aparta, Auman, Del Castillo, Reas, SisoJessa MeaNo ratings yet
- Flirting The IssueDocument3 pagesFlirting The IssueDecksGirlNo ratings yet
- Typhoid Fever: By, Arathy DarvinDocument35 pagesTyphoid Fever: By, Arathy DarvinJaina JoseNo ratings yet
- Matsyasana (Fish Pose) : TechniqueDocument1 pageMatsyasana (Fish Pose) : TechniqueKarisma SenapatiNo ratings yet
- Master of Pharmacy in Pharmacy PracticeDocument24 pagesMaster of Pharmacy in Pharmacy Practicecity cyberNo ratings yet
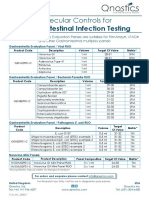
- Molecular Controls For Gastro-Intestinal Infection Testing - v2Document1 pageMolecular Controls For Gastro-Intestinal Infection Testing - v2moutasim mohammadNo ratings yet
- Hook For A Persuasive EssayDocument4 pagesHook For A Persuasive Essayb71g37ac100% (2)
- 3 Case Study On DM p.35 1Document44 pages3 Case Study On DM p.35 1Nina Fatima AllamNo ratings yet
- Jurnal Saraf 5Document5 pagesJurnal Saraf 5Suci MayveraNo ratings yet
- Xero PH Thal MiaDocument1 pageXero PH Thal MiaRavan WidiNo ratings yet
- 128 Research Papers Supporting The Vaccine Autism LinkDocument96 pages128 Research Papers Supporting The Vaccine Autism LinkEllaNo ratings yet
- Diagnotic Test MAPEHDocument5 pagesDiagnotic Test MAPEHAlma C Walsh0% (1)
- HEALTH COT DLP 3rdDocument3 pagesHEALTH COT DLP 3rdJK De GuzmanNo ratings yet
- Group 7 - Subgroup 2 Chief ComplaintDocument5 pagesGroup 7 - Subgroup 2 Chief ComplaintKAYLLIEN DURANNo ratings yet
- Overview of DiplopiaDocument21 pagesOverview of DiplopiadanielseanminneyNo ratings yet
- EMP3 Rosyidini Hazmi Nabila 30102000160Document14 pagesEMP3 Rosyidini Hazmi Nabila 30102000160rosydinihazmiNo ratings yet
- Inglês Médico - Aula 01Document26 pagesInglês Médico - Aula 01Leandro Teixeira dos SantosNo ratings yet
- Ebers Bryan-CP-The-Papyrus-Ebers-searchable-1930Document112 pagesEbers Bryan-CP-The-Papyrus-Ebers-searchable-1930Guillermo Benitez100% (1)
- Adventist GlenOaks Hospital 8110116874Document4 pagesAdventist GlenOaks Hospital 8110116874Mark Richard Hilbert (Rossetti)No ratings yet
- Common Pests and Breeding SitesDocument2 pagesCommon Pests and Breeding SitesJan Lianne BernalesNo ratings yet
- Pharmacology ReviewerDocument29 pagesPharmacology ReviewerIsabel Bibat DavidNo ratings yet
- Diphtheria The Strangling AngelDocument4 pagesDiphtheria The Strangling AngelDatu Nur-Jhun Salik, MDNo ratings yet
- Food Safety ManualDocument134 pagesFood Safety ManualKaran Singh RaiNo ratings yet
- PemphigusDocument1 pagePemphigusiSmayli (smyle-smayl)No ratings yet
- Board Recall Must ReadDocument8 pagesBoard Recall Must ReadSarahSalvanNo ratings yet
- Practical Research 2Document66 pagesPractical Research 2Cris Antonette AbataNo ratings yet
- 600 Item QBank For The PLEDocument203 pages600 Item QBank For The PLEVA SGNo ratings yet
- DLP Projector: User ManualDocument73 pagesDLP Projector: User ManualoddparentscribdNo ratings yet