Microbiology Laboratory Faculty of Medicine Brawijaya University
Microbiology Laboratory Faculty of Medicine Brawijaya University
Download as ppt, pdf, or txt
You might also like
- Mother Earth: The Sacred ProstituteDocument50 pagesMother Earth: The Sacred Prostitutelamacaroline67% (3)
- Corynebacterium DiphtheriaeDocument21 pagesCorynebacterium DiphtheriaehercolaniumNo ratings yet
- Bacterial Causes of URIDocument28 pagesBacterial Causes of URIOmar MohammedNo ratings yet
- Diphtheria Pertussis TetanusDocument43 pagesDiphtheria Pertussis Tetanuspnalinl108No ratings yet
- Diphtheria 25.5.2021Document46 pagesDiphtheria 25.5.2021Aarushi AgrawalNo ratings yet
- Diphtheria Pertussis TetanusDocument43 pagesDiphtheria Pertussis TetanusPURVI BARIANo ratings yet
- Diphtheria Pertussis TetanusDocument43 pagesDiphtheria Pertussis TetanusRomel Ciptoadi WijayaNo ratings yet
- Diphtheria Pertussis TetanusDocument44 pagesDiphtheria Pertussis TetanusayunusaNo ratings yet
- 2 Microbial Disease of The Respiratory SystemDocument63 pages2 Microbial Disease of The Respiratory Systemrandom stuffNo ratings yet
- 3-2 - Corynebacteria 2017Document2 pages3-2 - Corynebacteria 2017Dent.Ridha AlshairNo ratings yet
- Epidemiology and Control of Important Airborne Diseases IIDocument23 pagesEpidemiology and Control of Important Airborne Diseases IIanitaaniebo2017No ratings yet
- Case Study: Pathogenic Bacteriology 2009Document16 pagesCase Study: Pathogenic Bacteriology 2009Porombita PorumbelNo ratings yet
- Lesson 6Document3 pagesLesson 6droppersteinNo ratings yet
- Immunity To FungiDocument29 pagesImmunity To FungiNoor NawawraNo ratings yet
- Gram PositiveDocument83 pagesGram PositiveHunato KugerNo ratings yet
- Microbiology - Lecture (10) 2023 FallDocument42 pagesMicrobiology - Lecture (10) 2023 FallAbishek DhinakaranNo ratings yet
- Sterptococci Lecture NewDocument15 pagesSterptococci Lecture NewShreef SonsonNo ratings yet
- MycobacteriaDocument26 pagesMycobacteriacimdesadesuNo ratings yet
- StreptococciDocument39 pagesStreptococciالطاهر زروقNo ratings yet
- Airborne Transmission: Nurul Aqmar Mohd Nor Hazalin Phc454 - Pharmaceutical MicrobiologyDocument27 pagesAirborne Transmission: Nurul Aqmar Mohd Nor Hazalin Phc454 - Pharmaceutical MicrobiologySuhaila Abdul RahimNo ratings yet
- Communicable Diseasesp.170 199Document30 pagesCommunicable Diseasesp.170 199Gary Largosa GallardoNo ratings yet
- Mikrobiologi Parasitologi Respiration: AN IMO 2019Document64 pagesMikrobiologi Parasitologi Respiration: AN IMO 2019Sleeping BeautyNo ratings yet
- Pleuropulmonary InfectionsDocument40 pagesPleuropulmonary InfectionsRahmidatul AftikaNo ratings yet
- 2 Diphtheria 1Document30 pages2 Diphtheria 1Happy SinghNo ratings yet
- All 45 BugsDocument26 pagesAll 45 Bugsroboat96No ratings yet
- Haemophilus, Bordetella, Brucella,: and FrancisellaDocument29 pagesHaemophilus, Bordetella, Brucella,: and FrancisellaDaniel AtiehNo ratings yet
- Hidalgo, Rubenjie S. Dela Cruz, Anthony Jericho B. Abary, Claudine D. Tan Hoc, Anne Mei H. Oca, Renx MarkDocument52 pagesHidalgo, Rubenjie S. Dela Cruz, Anthony Jericho B. Abary, Claudine D. Tan Hoc, Anne Mei H. Oca, Renx MarkEira LopezNo ratings yet
- Microbial Diseases of Respiratory System AO Rev3Document40 pagesMicrobial Diseases of Respiratory System AO Rev3rahafahmed20043No ratings yet
- Infeksi Saluran Pernafasan BawahDocument36 pagesInfeksi Saluran Pernafasan BawahMhmd Rifki FaizNo ratings yet
- pertusisDocument31 pagespertusisDR MOHAMED HEALTH CHANNELNo ratings yet
- Infection of Nose, Sinus and EarDocument18 pagesInfection of Nose, Sinus and EarMuhammad FadlilahNo ratings yet
- Clinical Manifestations of DiphteriaDocument7 pagesClinical Manifestations of DiphteriaRuturaj JadejaNo ratings yet
- DiphtheriaDocument15 pagesDiphtheriaelka.kgmaNo ratings yet
- DiphtheriaDocument23 pagesDiphtheriaMohammed HamidNo ratings yet
- Microbial Diseases of The Respiratory SystemDocument30 pagesMicrobial Diseases of The Respiratory SystemChristopher Eria Santiañez0% (1)
- Anaerobic BacteriaDocument52 pagesAnaerobic BacteriazaheerbinzubairNo ratings yet
- Cory Ne BacteriumDocument25 pagesCory Ne BacteriumjmalavanuNo ratings yet
- 14-Diphtheria - Pertussis - and Brucellosis 44-45Document40 pages14-Diphtheria - Pertussis - and Brucellosis 44-45Manar AlhakamiNo ratings yet
- 13 - Gram Positive RodsDocument24 pages13 - Gram Positive Rodsabody abodyNo ratings yet
- بكتيريا اخر محاضراتDocument52 pagesبكتيريا اخر محاضراتIftikharNo ratings yet
- Microbiology Lecture 3: Respiratory Tract Infections Medicine Ii Dr. Anna Lynda Bellen ZjrnateDocument9 pagesMicrobiology Lecture 3: Respiratory Tract Infections Medicine Ii Dr. Anna Lynda Bellen Zjrnatezahj nateNo ratings yet
- Diphteria, ListeriaDocument20 pagesDiphteria, ListeriaLore LorenaNo ratings yet
- Corynebacterium Diphteriae: 3 Year Pharmacy, Semester 2, 2021Document20 pagesCorynebacterium Diphteriae: 3 Year Pharmacy, Semester 2, 2021Xing YuNo ratings yet
- DiphtheriaDocument10 pagesDiphtheriakudzaimuregidubeNo ratings yet
- Respiratory infection public healthDocument32 pagesRespiratory infection public health- fa44dak -No ratings yet
- Types of TuberculosisDocument7 pagesTypes of TuberculosisYashaswi ANo ratings yet
- CHN Midterm ReviewerDocument54 pagesCHN Midterm ReviewerJoi PreconesNo ratings yet
- Diptheria Nursing ManagementDocument14 pagesDiptheria Nursing ManagementMey MeyNo ratings yet
- Surgical InfectionsDocument24 pagesSurgical InfectionsBenja MutindaNo ratings yet
- Anaerobic Bacteria: Dept. of Microbiology Medical Faculty, Padjadjaran UniversityDocument52 pagesAnaerobic Bacteria: Dept. of Microbiology Medical Faculty, Padjadjaran UniversitySabrina Indri WardaniNo ratings yet
- PediatricsDocument31 pagesPediatricsLuai Tuma KhouryNo ratings yet
- Diphtheria HandoutsDocument8 pagesDiphtheria HandoutsRachelle Mae DimayugaNo ratings yet
- Etiology: M Tuberculosis Is A Slow-Growing, Obligate Aerobe and A Facultative, Intracellular Parasite. TheDocument5 pagesEtiology: M Tuberculosis Is A Slow-Growing, Obligate Aerobe and A Facultative, Intracellular Parasite. TheFerdi StefiyanNo ratings yet
- Infectious Diseases (1&2) : TuberculosisDocument67 pagesInfectious Diseases (1&2) : TuberculosisYesi SaputriNo ratings yet
- Lecture 22. Diphtheria. Dysentery. Scarlatina. DiphtheriaDocument4 pagesLecture 22. Diphtheria. Dysentery. Scarlatina. DiphtheriaIsak ShatikaNo ratings yet
- BINCY P B - Pneumococcal InfectionsDocument32 pagesBINCY P B - Pneumococcal InfectionsRaya ThesseahNo ratings yet
- 5 Mikrobiologi (Dr. Enny S, M.kes)Document115 pages5 Mikrobiologi (Dr. Enny S, M.kes)fitkaNo ratings yet
- Pathology WildlifeDocument21 pagesPathology WildlifenamratapanemNo ratings yet
- (SGD) PathologyDocument6 pages(SGD) PathologyPaulene RiveraNo ratings yet
- Communicable DiseasesDocument164 pagesCommunicable DiseasesJasmin Jacob33% (3)
- 911 Pigeon Disease & Treatment Protocols!From Everand911 Pigeon Disease & Treatment Protocols!Rating: 4 out of 5 stars4/5 (1)
- BONE (Histology)Document65 pagesBONE (Histology)fhfebriiNo ratings yet
- Anatomy & Histology Dept. Brawijaya Medical FacultyDocument78 pagesAnatomy & Histology Dept. Brawijaya Medical FacultyfhfebriiNo ratings yet
- MR Radio 19 Jan 2018Document12 pagesMR Radio 19 Jan 2018fhfebriiNo ratings yet
- Community Diagnosis 2018Document97 pagesCommunity Diagnosis 2018fhfebriiNo ratings yet
- Manajemen SDM (Teamwork) : Changing Organizational CultureDocument20 pagesManajemen SDM (Teamwork) : Changing Organizational CulturefhfebriiNo ratings yet
- Modern Perl A4Document186 pagesModern Perl A4Henrik NårstadNo ratings yet
- WRC Bulletin 275Document6 pagesWRC Bulletin 275Bhadresh PrajapatiNo ratings yet
- Scaffolding Material Calc. For Wall FaceDocument36 pagesScaffolding Material Calc. For Wall FaceShashank HegdeNo ratings yet
- Nama: Rahma Aini NIM: 21332052 Prodi: Pendidikan Bahasa InggrisDocument2 pagesNama: Rahma Aini NIM: 21332052 Prodi: Pendidikan Bahasa InggrisRahma ainiNo ratings yet
- African Grey ParrotsDocument1 pageAfrican Grey Parrotsclark kenNo ratings yet
- O9CTNDxISFSa9UVVI0rFyw Activity Template Data Leak WorksheetDocument3 pagesO9CTNDxISFSa9UVVI0rFyw Activity Template Data Leak Worksheetf.samui.almeidaNo ratings yet
- Philo Final SummativeDocument2 pagesPhilo Final SummativeFobe Lpt NudaloNo ratings yet
- 5 - Testing and SelectionDocument27 pages5 - Testing and SelectionNadeem AhmadNo ratings yet
- Ieeeansi 571290 PDFDocument93 pagesIeeeansi 571290 PDFdharm rajNo ratings yet
- Second Service: William ByrdDocument11 pagesSecond Service: William ByrdGameunrealNo ratings yet
- Investment Banking 2014Document336 pagesInvestment Banking 2014Thibault MHNo ratings yet
- First Known BlackoutDocument14 pagesFirst Known Blackoutp61466365No ratings yet
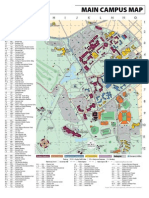
- Campus MapDocument1 pageCampus MapquanghiepftuNo ratings yet
- Enron Accounting ScandalDocument10 pagesEnron Accounting ScandalParvinder SinghNo ratings yet
- Hands On Exercise No. 2 Digiskills - PK Batch-01 Freelancing Total Marks: 10 Due Date: 17/03/2022Document3 pagesHands On Exercise No. 2 Digiskills - PK Batch-01 Freelancing Total Marks: 10 Due Date: 17/03/2022Izhar Ahmed NoohpotoNo ratings yet
- Add A SubheadingDocument13 pagesAdd A Subheadingamany hakeemNo ratings yet
- En Wikipedia Org Wiki Lifeforce FilmDocument11 pagesEn Wikipedia Org Wiki Lifeforce Filmvijaybabup9900% (1)
- Assignment 1Document3 pagesAssignment 1Hafez MohammedNo ratings yet
- 1.concept of LanguageDocument19 pages1.concept of LanguageIstiqomah BonNo ratings yet
- Course Outline - Updated To ArrestDocument6 pagesCourse Outline - Updated To ArrestDalgi MembrillosNo ratings yet
- Income Certificate Format - 2021Document1 pageIncome Certificate Format - 2021Faltu Ka jhamlqNo ratings yet
- Team Building Class For Elementary XL by SlidesgoDocument92 pagesTeam Building Class For Elementary XL by SlidesgoelianaNo ratings yet
- Mystic Test Book of The Hindu Occult ChambersDocument193 pagesMystic Test Book of The Hindu Occult Chamberssantsetesh100% (3)
- Rashtrasant Tukadoji Maharaj Nagpur University: NotificationDocument55 pagesRashtrasant Tukadoji Maharaj Nagpur University: NotificationDeepshikha MehtaNo ratings yet
- Section A: Sample/Pre-Board Paper 3 Class X Term 1 Exam Nov - Dec 2021 Mathematics (Standard) 041Document5 pagesSection A: Sample/Pre-Board Paper 3 Class X Term 1 Exam Nov - Dec 2021 Mathematics (Standard) 041C.Rithish 6No ratings yet
- Internship GuideDocument28 pagesInternship GuidesanswathiNo ratings yet
- RSE+Reyee+Hotel+Solution+2024 Q2 PDFDocument66 pagesRSE+Reyee+Hotel+Solution+2024 Q2 PDFEdmar AberinNo ratings yet
- SSC CGL and CHSL Practice Book For Competitive Exams LDocument6 pagesSSC CGL and CHSL Practice Book For Competitive Exams LNARAYAN NAHAKNo ratings yet
- Coporate LiquidationDocument5 pagesCoporate LiquidationMary Dale Joie BocalaNo ratings yet