Intrapartum Fetal Surveillance 1
Intrapartum Fetal Surveillance 1
Download as pptx, pdf, or txt
You might also like
- Examination of The Newborn An Evidence Based Guide PDFDocument2 pagesExamination of The Newborn An Evidence Based Guide PDFPhilNo ratings yet
- Newborn ExaminationDocument45 pagesNewborn ExaminationHamka Ham100% (1)
- Breast Examination - OSCE Guide - Geeky MedicsDocument6 pagesBreast Examination - OSCE Guide - Geeky MedicsJahangir AlamNo ratings yet
- 211 Manuel Cardiotocographe Bt330Document40 pages211 Manuel Cardiotocographe Bt330Mathurin Edmond WolaeNo ratings yet
- 9fetal Well Being in PregnancyDocument10 pages9fetal Well Being in PregnancyuouoNo ratings yet
- Antepartum Fetal MonitoringDocument4 pagesAntepartum Fetal MonitoringChristoperJ.ErecreNo ratings yet
- Antenatal Assessment of Fetal WellbeingDocument67 pagesAntenatal Assessment of Fetal WellbeingPaunami Dey50% (2)
- Medical School Companion Obstetrics and Gynecology Practice Question BookFrom EverandMedical School Companion Obstetrics and Gynecology Practice Question BookRating: 1 out of 5 stars1/5 (1)
- Partograph-Presentation-SBA TrainingDocument11 pagesPartograph-Presentation-SBA TrainingPradeep Verma0% (1)
- How To Read A CTGDocument11 pagesHow To Read A CTGiwennieNo ratings yet
- Management of PPH by DR - Manuel Hutapea, SP - Og (K) OnkDocument17 pagesManagement of PPH by DR - Manuel Hutapea, SP - Og (K) Onkvicky v. p. wardenaarNo ratings yet
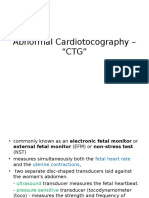
- Abnormal Cardiotocography - "CTG"Document47 pagesAbnormal Cardiotocography - "CTG"Ahmad Mustaqim SulaimanNo ratings yet
- 63 Shock in Obstetrics & GynecologyDocument29 pages63 Shock in Obstetrics & GynecologyGodsonYeboah-AwudziNo ratings yet
- Hypertensive Disorders of Pregnancy: Priyanka GehlotDocument50 pagesHypertensive Disorders of Pregnancy: Priyanka GehlotpriyankaNo ratings yet
- Normal LabourDocument10 pagesNormal LabourikeyoganitabangunNo ratings yet
- Normal LaborDocument70 pagesNormal LaborAmlodipine BesylateNo ratings yet
- Stillbirth C1 PPT - LectureDocument35 pagesStillbirth C1 PPT - LectureHenok Y KebedeNo ratings yet
- Case Study CPLDocument7 pagesCase Study CPLSkyllen FhayeNo ratings yet
- 4-Gynae Obs PT 24-04-2020Document35 pages4-Gynae Obs PT 24-04-2020DaniJaralNo ratings yet
- Obstetric Summm 1Document46 pagesObstetric Summm 1ملك عيسىNo ratings yet
- CardiotocographyDocument51 pagesCardiotocographyticticNo ratings yet
- Anorectal Malformations: Presented by Khushveer KaurDocument91 pagesAnorectal Malformations: Presented by Khushveer KaurKataria DavinNo ratings yet
- Obstetric ExaminationDocument26 pagesObstetric Examinationshofa nur rahmannisaNo ratings yet
- HELLP SyndromeDocument3 pagesHELLP SyndromeWidyawati TjahjadiNo ratings yet
- Psychological Perspective of Abnormal LaborDocument25 pagesPsychological Perspective of Abnormal LaborPriscilla Sarah PayneNo ratings yet
- SDMS ID: P2010/0496-001 2.9/09WACS Title: Management of Postpartum HaemorrhageDocument11 pagesSDMS ID: P2010/0496-001 2.9/09WACS Title: Management of Postpartum HaemorrhageYwagar YwagarNo ratings yet
- Assessment of The Fetal Well-BeingDocument85 pagesAssessment of The Fetal Well-BeingAlphine DalgoNo ratings yet
- Abortion 1Document46 pagesAbortion 1Nikhil TyagiNo ratings yet
- 2 Abnormal LaborDocument88 pages2 Abnormal LaborThya Hakim100% (1)
- 3rd and 4th Stage of LaborDocument8 pages3rd and 4th Stage of LaborMarco Paulo Reyes NaoeNo ratings yet
- Presentation 2Document49 pagesPresentation 2Wahyu Adhitya Prawirasatra100% (2)
- Postnatal AssessmentDocument9 pagesPostnatal Assessmentsaleha sultana100% (1)
- Prolonged LabourDocument3 pagesProlonged Labourgeorgeloto12No ratings yet
- Gynecological Operation and Nursing ManagementDocument29 pagesGynecological Operation and Nursing Managementhawra alsaad100% (1)
- Hypertensive Disorders of PregnancyDocument9 pagesHypertensive Disorders of PregnancyFcm-srAaf100% (1)
- Developed by D. Ann Currie, RN, MSNDocument40 pagesDeveloped by D. Ann Currie, RN, MSNtri utamiNo ratings yet
- Exercises To Facilitate Change of Baby's Position From Breech To CephalicDocument3 pagesExercises To Facilitate Change of Baby's Position From Breech To CephalicaziskarnNo ratings yet
- Obstructed Labor AND ITS CAUSE, CORD PROLAPS AND PRESENTATIONDocument59 pagesObstructed Labor AND ITS CAUSE, CORD PROLAPS AND PRESENTATIONmaezu100% (2)
- Pregnancy Induced Hypertension: DefinitionDocument7 pagesPregnancy Induced Hypertension: Definitionkristine hinaresNo ratings yet
- WHO Labour Care GuideDocument34 pagesWHO Labour Care GuideAnkita Singh100% (1)
- Ultrasound in ObstetricsDocument3 pagesUltrasound in ObstetricsSarita DubeyNo ratings yet
- Cervical CerclageDocument19 pagesCervical CerclageKarleneNo ratings yet
- Vaginal Birth After Previous Caesarean SectionDocument26 pagesVaginal Birth After Previous Caesarean SectionWonyenghitari George100% (1)
- 26a. Post Partum HemorrhageDocument35 pages26a. Post Partum HemorrhageAubrey100% (1)
- Instrumental DeliveryDocument25 pagesInstrumental DeliveryAhmed ElmohandesNo ratings yet
- Antenatal VisitsDocument8 pagesAntenatal VisitsKumarNo ratings yet
- VersionDocument15 pagesVersionAnees Siddiqui100% (2)
- Abdominal Examination ChecklistDocument3 pagesAbdominal Examination ChecklistYara Wael100% (1)
- Malposition and MalpresentationDocument60 pagesMalposition and MalpresentationDrPreeti Thakur Chouhan100% (1)
- Prenatal Care by Connie Sussan AustenDocument31 pagesPrenatal Care by Connie Sussan AustenNoraNo ratings yet
- Normal Conduct of LaborDocument62 pagesNormal Conduct of LaborFaye Cabotaje LinganNo ratings yet
- Abnormal Uterine ActionDocument110 pagesAbnormal Uterine ActionAnnapurna DangetiNo ratings yet
- CORDOCENTESISDocument6 pagesCORDOCENTESISSagar HanamasagarNo ratings yet
- Pre EclampsiaDocument8 pagesPre EclampsiaJamie Agbannawag100% (1)
- Occipito-Posterior Position of The Fetal HeadDocument8 pagesOccipito-Posterior Position of The Fetal HeaduouoNo ratings yet
- Fetal Growth Restriction - ACOG 2019Document23 pagesFetal Growth Restriction - ACOG 2019Adhitya Yudha Maulana100% (1)
- Antepartum HemorrhageDocument18 pagesAntepartum HemorrhageSanaNo ratings yet
- Antenatal Assessment of Fetal Well-BeingDocument18 pagesAntenatal Assessment of Fetal Well-BeingAmritaNo ratings yet
- Post Partum HemorrhageDocument12 pagesPost Partum HemorrhageMd. Lutfor Rahman KhanNo ratings yet
- Partograph Literature ReviewDocument36 pagesPartograph Literature ReviewIrma Fatimah100% (2)
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- RSDocument682 pagesRSDeni ArdiansyahNo ratings yet
- Sinusoidal and Saltatory Patterns: Unusual Fetal Heart Rate PatternsDocument5 pagesSinusoidal and Saltatory Patterns: Unusual Fetal Heart Rate PatternsMaria MogosNo ratings yet
- Fetal SurvillanceDocument26 pagesFetal SurvillanceBetelhem EjiguNo ratings yet
- Test Drill OBDocument8 pagesTest Drill OBViviane Ńíáshéè Basod100% (1)
- Final Obgn HandoutDocument36 pagesFinal Obgn HandoutAhmad Faizul AbdrahmansazliNo ratings yet
- Silliman University: Nursing Care Plan On Preeclampsia With Severe FeaturesDocument8 pagesSilliman University: Nursing Care Plan On Preeclampsia With Severe FeaturesRyan Robert V. VentoleroNo ratings yet
- Abnormal Uterine ContractionDocument34 pagesAbnormal Uterine Contractionsapana shahNo ratings yet
- Cesarean Birth - Surgical TechniquesDocument21 pagesCesarean Birth - Surgical TechniquesInatrinNo ratings yet
- Contraction Stress Test: The Underline Physiological and Technological Basis For The CST Are As FollowsDocument3 pagesContraction Stress Test: The Underline Physiological and Technological Basis For The CST Are As FollowsSagar HanamasagarNo ratings yet
- NURS 3337 Day1 WorkbookDocument18 pagesNURS 3337 Day1 WorkbookEmerald Holly TagoNo ratings yet
- Extension of Review Date: Translating Evidence Into Best Clinical PracticeDocument39 pagesExtension of Review Date: Translating Evidence Into Best Clinical PracticeEvan SaapNo ratings yet
- Management of Meconium Stained Liquor 6.0Document12 pagesManagement of Meconium Stained Liquor 6.0andi hamatajNo ratings yet
- CPG Abnormal Labor and Delivery PDFDocument29 pagesCPG Abnormal Labor and Delivery PDFKarl Jimenez Separa100% (2)
- Partograph and CTG Intrapartum Fetal MonitoringDocument56 pagesPartograph and CTG Intrapartum Fetal MonitoringPEÑAFLOR, Shealtiel Joy G.No ratings yet
- Labour+and+Birth.+Routine+care+in+normal+labour+ Birth PPG V1 1Document22 pagesLabour+and+Birth.+Routine+care+in+normal+labour+ Birth PPG V1 1Arti NegiNo ratings yet
- Radha Antenatal Fetal Well Being1Document32 pagesRadha Antenatal Fetal Well Being1Shaells JoshiNo ratings yet
- WHO Labour Care GuideDocument34 pagesWHO Labour Care GuideAnkita Singh100% (1)
- Antenatal Foetal MonitoringDocument65 pagesAntenatal Foetal Monitoringsyirah99No ratings yet
- Antenatal AssessmentDocument84 pagesAntenatal AssessmentRitbano AhmedNo ratings yet
- 13.Labour-Partograph-Plotting and InterpretationDocument9 pages13.Labour-Partograph-Plotting and InterpretationHem KumariNo ratings yet
- Prolonged Pregnancy: Table 1Document5 pagesProlonged Pregnancy: Table 1Yo MeNo ratings yet
- Antenatal Cardiotocography For Fetal Assessment (Review) : Grivell RM, Alfirevic Z, Gyte GML, Devane DDocument50 pagesAntenatal Cardiotocography For Fetal Assessment (Review) : Grivell RM, Alfirevic Z, Gyte GML, Devane DDara Loor GonzálesNo ratings yet
- Optimal Obstetric Management For Women With Diabetes - The Benefits and Costs of Fetal SurveillanceDocument9 pagesOptimal Obstetric Management For Women With Diabetes - The Benefits and Costs of Fetal SurveillanceWillians ReyesNo ratings yet
- Ncma219 Course Task 3Document18 pagesNcma219 Course Task 3NikoruNo ratings yet
- Labor Delivery 1Document29 pagesLabor Delivery 1Elmer DaquilañeaNo ratings yet
- Fetal Assessment and Wellbeing in Pregnancy (FetalDocument23 pagesFetal Assessment and Wellbeing in Pregnancy (Fetalapi-3705046100% (1)
- Student Copy Conti - Intrapartal Week8Document25 pagesStudent Copy Conti - Intrapartal Week8Toyour EternityNo ratings yet
- How To Read A CTGDocument16 pagesHow To Read A CTGHussain H. HussainNo ratings yet