Anemia
Anemia
Download as pptx, pdf, or txt
You might also like
- Emergency Care (Hemophilia)Document30 pagesEmergency Care (Hemophilia)Nica Georgelle Maniego SamonteNo ratings yet
- An Overview Of: Acute Kidney Injury (Aki: Hasan BasriDocument22 pagesAn Overview Of: Acute Kidney Injury (Aki: Hasan BasriDz PutraNo ratings yet
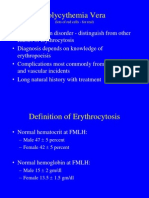
- PolycythemiaDocument22 pagesPolycythemiaIrman DinejadNo ratings yet
- Assessing Chronic Illness Representations - The Implicit Models of Illness QuestionnaiDocument18 pagesAssessing Chronic Illness Representations - The Implicit Models of Illness QuestionnaiiulianaNo ratings yet
- An Approach To Common Urological Disorders PDFDocument45 pagesAn Approach To Common Urological Disorders PDFCrystel Tze JingNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 16: HematologyFrom EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyNo ratings yet
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hypophosphatemia, (Low Phosphate) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypophosphatemia, (Low Phosphate) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Complications Blood TransfusionDocument7 pagesComplications Blood TransfusionWajeehaWasimNo ratings yet
- Anemia and Critical CareDocument77 pagesAnemia and Critical Carehunter_axl010% (1)
- ZENICADocument72 pagesZENICAVedadNo ratings yet
- Blood ManagmentDocument22 pagesBlood ManagmentNana Yaw OwusuNo ratings yet
- What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Document60 pagesWhat Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Priyanka MhNo ratings yet
- Case 1 - Sickle Cell Disease - PPSXDocument44 pagesCase 1 - Sickle Cell Disease - PPSXNICHOLAS KAUMBA100% (1)
- Chronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDocument42 pagesChronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDon RaulNo ratings yet
- Geriatrics Trauma Power Point Presentation Dr. BarbaDocument23 pagesGeriatrics Trauma Power Point Presentation Dr. Barbagiscaamilia100% (1)
- Geriatric Trauma - WaniDocument60 pagesGeriatric Trauma - WaniNurul Syazwani Ramli100% (1)
- KMU Blood DisorderDocument43 pagesKMU Blood DisorderSHAFIQNo ratings yet
- Clotting MechanismDocument3 pagesClotting MechanismLindsey SimmonsNo ratings yet
- HypercalcemiaDocument50 pagesHypercalcemiaEvelyn EdgarNo ratings yet
- Infection Control Standards in Blood TransfusionDocument44 pagesInfection Control Standards in Blood Transfusionyang_torn100% (2)
- An Introduction To AnaemiaDocument27 pagesAn Introduction To Anaemiaمجاهد إسماعيل حسن حسينNo ratings yet
- Haemolytic AnaemiaDocument11 pagesHaemolytic AnaemiaSonam JoshiNo ratings yet
- Mitochondrial DisorderDocument3 pagesMitochondrial DisorderRoxie May Theresse AbagatnanNo ratings yet
- Acute Liver FailureDocument69 pagesAcute Liver FailureAsif.N.IqbalNo ratings yet
- Bleeding Disorders: LCDR Art GeorgeDocument54 pagesBleeding Disorders: LCDR Art Georgesatya_mdsNo ratings yet
- Transfusion Reactions CHDocument22 pagesTransfusion Reactions CHHenni Wahyu Triyuniati100% (1)
- Chronic Obstructive Pulmonary DiseaseDocument161 pagesChronic Obstructive Pulmonary DiseaseClarisse Nicole TanNo ratings yet
- Cvs PracticalDocument63 pagesCvs PracticalSreedeep TejaNo ratings yet
- Thrombocytopenia Sarah WalterDocument49 pagesThrombocytopenia Sarah WalterSupicha VichaiditNo ratings yet
- Practice Essentials: Signs and SymptomsDocument4 pagesPractice Essentials: Signs and Symptomschalya pratistha100% (1)
- The Bleeding Child OSCE HaemophiliaDocument3 pagesThe Bleeding Child OSCE HaemophiliaJJ LimNo ratings yet
- Approach To Abdominal Masses in ChildrenDocument36 pagesApproach To Abdominal Masses in ChildrenMia Lesaca-Medina100% (3)
- Chronic Obstructive Pulmonary DiseaseDocument33 pagesChronic Obstructive Pulmonary DiseasealexpharmNo ratings yet
- Primary Immunodeficiency Disease FinalDocument35 pagesPrimary Immunodeficiency Disease FinalDixie DumagpiNo ratings yet
- 1 ParkinsonsDocument58 pages1 ParkinsonsgautambobNo ratings yet
- AnemiaDocument116 pagesAnemiaStanly stephenNo ratings yet
- Blood Component TherapyDocument73 pagesBlood Component TherapySaikat Prasad DattaNo ratings yet
- Polycythemia Vera: DR - Karthik.S Moderator:Dr - Sumedh ShettyDocument51 pagesPolycythemia Vera: DR - Karthik.S Moderator:Dr - Sumedh ShettyDr. Apoorva KottaryNo ratings yet
- Onconephrology Core Curriculum 2023Document19 pagesOnconephrology Core Curriculum 2023jogutiro01100% (1)
- Chronic Congestive Heart Failure: American Heart Association Sociedad Española de CardiologíaDocument94 pagesChronic Congestive Heart Failure: American Heart Association Sociedad Española de Cardiologíaladyminervs08100% (2)
- VasculitidesDocument13 pagesVasculitidesIrene Zae MwandotoNo ratings yet
- Normocytic Anemia'sDocument14 pagesNormocytic Anemia'sbrown_chocolate87643No ratings yet
- Classification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Document78 pagesClassification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Kaushik Bhuva100% (1)
- Jaundice MasterDocument76 pagesJaundice MasterVinoth KumarNo ratings yet
- By: DR Eyad Talal: Moderator: DR I - QudaisatDocument55 pagesBy: DR Eyad Talal: Moderator: DR I - QudaisatEyad AbdeljawadNo ratings yet
- Leucodepletion Filter PDFDocument29 pagesLeucodepletion Filter PDFmukeshNo ratings yet
- AKIDocument23 pagesAKInadddNo ratings yet
- Classification of Anemia OkDocument60 pagesClassification of Anemia OkAnonymous 7CnBF0cjNo ratings yet
- AlcoholDocument20 pagesAlcoholrecklesspeshal2058100% (1)
- Presentation 1Document44 pagesPresentation 1HeforSheNo ratings yet
- Abnormal CBC - PresentationDocument23 pagesAbnormal CBC - PresentationMateen ShukriNo ratings yet
- Megaloblastic AnaemiaDocument11 pagesMegaloblastic AnaemiaJesmin_36No ratings yet
- DR Aida Lombok 3 Mei 2017 - HisfarsiDocument39 pagesDR Aida Lombok 3 Mei 2017 - HisfarsiBasri BaslamNo ratings yet
- A. Inflammation and Repair: I. Disease Process (6 Questions)Document17 pagesA. Inflammation and Repair: I. Disease Process (6 Questions)Anonymous Sw4Pk9fNo ratings yet
- Introduction To HaemostasisDocument18 pagesIntroduction To Haemostasiswatchme3No ratings yet
- HRSDocument63 pagesHRSPriya KalariaNo ratings yet
- Cerebrovascular AccidentDocument31 pagesCerebrovascular AccidentRam ReddyNo ratings yet
- Peripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Document46 pagesPeripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Dzariyat_Azhar_9277100% (1)
- Anaemia in PregnancyDocument15 pagesAnaemia in PregnancyNorshahidah Ieda100% (1)
- Assessment of Metabolic AcidosisDocument34 pagesAssessment of Metabolic Acidosisfatha100% (1)
- 4 Blood ProductsDocument11 pages4 Blood ProductsGampa VijaykumarNo ratings yet
- 1533293623Q IDocument10 pages1533293623Q IthilagavathyNo ratings yet
- Renal - MedbulletsDocument74 pagesRenal - Medbulletssmian08No ratings yet
- Bio Ia PDFDocument13 pagesBio Ia PDFLia Marie BeloyNo ratings yet
- 14 - STUDY INTO KID'S INHALER USE OetDocument20 pages14 - STUDY INTO KID'S INHALER USE OetRithu SanthoshNo ratings yet
- Jooo 1 3 126-128 1Document4 pagesJooo 1 3 126-128 1Indah IndrianiNo ratings yet
- 144 272 1 SMDocument50 pages144 272 1 SMdyasNo ratings yet
- Lmr-Hematology: Bad Prognostic Factors For ALLDocument3 pagesLmr-Hematology: Bad Prognostic Factors For ALLYuku BabyNo ratings yet
- Hare Krsna Book ofDocument213 pagesHare Krsna Book ofDilip YadavNo ratings yet
- Radiology Report 2300985Document4 pagesRadiology Report 2300985JyotiNo ratings yet
- Indian Council of Medical ResearchDocument43 pagesIndian Council of Medical ResearchVivek YadavNo ratings yet
- Blood Donation DissertationDocument8 pagesBlood Donation DissertationFinishedCustomWritingPaperSingapore100% (1)
- Medtronic Gi Portfolio BrochureDocument10 pagesMedtronic Gi Portfolio BrochuremubaraknlhddNo ratings yet
- SW Provider Directory 2018 1ST QTR - CompressedDocument20 pagesSW Provider Directory 2018 1ST QTR - CompressedStayWell InsuranceNo ratings yet
- Bài Tập Cấu Trúc Câu So SánhDocument92 pagesBài Tập Cấu Trúc Câu So SánhVũ Hoàng Hải MyNo ratings yet
- Autoimmune Bullous Dermatoses - Overview of Serological Diagnostics in Blister Forming Diseases of The SkinDocument8 pagesAutoimmune Bullous Dermatoses - Overview of Serological Diagnostics in Blister Forming Diseases of The SkinFedoxyzNo ratings yet
- Who Inquiry PDFDocument260 pagesWho Inquiry PDFAnjali TajayanNo ratings yet
- Circular Cghs 2010 Cghs Rates DelhiDocument24 pagesCircular Cghs 2010 Cghs Rates Delhipradeep2002002No ratings yet
- Second Paper Assignment: It's Over, DebbieDocument2 pagesSecond Paper Assignment: It's Over, DebbieCristina Mihaela FNo ratings yet
- MAPEH 9 Second GradingDocument9 pagesMAPEH 9 Second GradingSittie Rahma AlawiNo ratings yet
- CASE STUDY Acute PancreatitisDocument12 pagesCASE STUDY Acute PancreatitisChristine Evan HoNo ratings yet
- Review On The Aflatoxins' Contamination of Foods and Public Health Effects Among Nigerian PopulationDocument17 pagesReview On The Aflatoxins' Contamination of Foods and Public Health Effects Among Nigerian PopulationUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Ovarian TumorsDocument73 pagesOvarian Tumorsabhishekrajpurohit275No ratings yet
- Protozoa ReferenceDocument112 pagesProtozoa ReferenceMiaQuiambaoNo ratings yet
- The Evaluation and Management of Neck Masses of Unknown EtiologyDocument38 pagesThe Evaluation and Management of Neck Masses of Unknown EtiologyShaxawan Mahmood AliNo ratings yet
- HoxseyDocument7 pagesHoxseyuncoveringconsciousNo ratings yet
- NCM 118 RleDocument10 pagesNCM 118 RleJamaica Leslie NovenoNo ratings yet
- Lymph Node PathologyDocument4 pagesLymph Node PathologyGerardLum0% (1)
- The International Academy of Cytology Yokohama System For Reporting Breast Fine-Needle Aspiration Biopsy CytopathologyDocument17 pagesThe International Academy of Cytology Yokohama System For Reporting Breast Fine-Needle Aspiration Biopsy Cytopathologyunimo.prgNo ratings yet