Malpresentations: Liji Raichel Kurian Dept of OBG
Malpresentations: Liji Raichel Kurian Dept of OBG
Download as pptx, pdf, or txt
You might also like
- Placenta PreviaDocument33 pagesPlacenta PreviaKinjal Vasava100% (1)
- Oral Sex Mini BookDocument115 pagesOral Sex Mini Bookshuely akter100% (1)
- Top 25 Female Orgasm TipsDocument37 pagesTop 25 Female Orgasm Tipssexypuka49% (45)
- The Kegel Legacy-Print Version 1308Document100 pagesThe Kegel Legacy-Print Version 1308teju2812No ratings yet
- Rati SastrasDocument2 pagesRati SastrasRavi Soni100% (1)
- Malpresentations and MalpositionsDocument14 pagesMalpresentations and MalpositionsAsteway MesfinNo ratings yet
- Presentation 2Document49 pagesPresentation 2Wahyu Adhitya Prawirasatra100% (2)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Management of Breech PresentationDocument27 pagesManagement of Breech Presentationapi-370504683% (6)
- Breech PresentationDocument35 pagesBreech PresentationPrince Jhessie L. AbellaNo ratings yet
- CPDDocument45 pagesCPDVijith.V.kumar100% (1)
- Shoulder DystociaDocument9 pagesShoulder DystociaSoriao, Lovely Rose V.100% (1)
- Benefits of BreastfeedingDocument20 pagesBenefits of BreastfeedingIan FordeNo ratings yet
- Prolonged LaborDocument6 pagesProlonged LaborBqSafinatun NajaNo ratings yet
- CPD Book and Patient PictureDocument6 pagesCPD Book and Patient PicturePriyaNo ratings yet
- OB GDM CasepresDocument102 pagesOB GDM Casepreskitten garciaNo ratings yet
- NVD With EpisiotomyDocument4 pagesNVD With EpisiotomySimran SimzNo ratings yet
- Active Management of The Third Stage of LabourDocument15 pagesActive Management of The Third Stage of LabourtyasNo ratings yet
- Premature Rupture of Membranes (Prom)Document12 pagesPremature Rupture of Membranes (Prom)KABERA RENE50% (2)
- Compound PresentationDocument10 pagesCompound PresentationmaezuNo ratings yet
- A Nursing Care Plan On OligohydramniosDocument7 pagesA Nursing Care Plan On OligohydramniosTintin Honra100% (1)
- Obstetrics: The Fetus-in-Utero (Lie, Presentation & Position)Document28 pagesObstetrics: The Fetus-in-Utero (Lie, Presentation & Position)Sanjeet SahNo ratings yet
- Shoulder DystociaDocument22 pagesShoulder Dystociaamulan_aNo ratings yet
- Leopold's ManeuverDocument3 pagesLeopold's ManeuverKristine Marie de MesaNo ratings yet
- Breech PresentationDocument85 pagesBreech Presentationwidya vannesaNo ratings yet
- Mechanism of LabourDocument16 pagesMechanism of LabourRadha SriNo ratings yet
- HIV in Pregnancy TopicDocument50 pagesHIV in Pregnancy TopicstepnemoNo ratings yet
- Ectopic PregnancyDocument11 pagesEctopic PregnancyPrincess BalloNo ratings yet
- Antepartum Hemorrhage: Placental CausesDocument9 pagesAntepartum Hemorrhage: Placental CausesadiNo ratings yet
- Complications of PuerperiumDocument20 pagesComplications of Puerperiumrevathidadam55555No ratings yet
- Gestational Trophoblastic DiseaseDocument4 pagesGestational Trophoblastic DiseasePrincess PlateroNo ratings yet
- Cord Presentation ProlapseDocument10 pagesCord Presentation ProlapseJHONESSA LAYOSNo ratings yet
- EpisiotomyDocument16 pagesEpisiotomyRosu GeorgeNo ratings yet
- Complications and Treatment of JaundiceDocument7 pagesComplications and Treatment of JaundicenihalNo ratings yet
- Cephalopelvic DisproportionDocument3 pagesCephalopelvic DisproportionAira MiyaNo ratings yet
- Dystocia - Case ReportDocument51 pagesDystocia - Case ReportPaijo SusenoNo ratings yet
- Normal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, VapiDocument48 pagesNormal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, Vapivimmy47100% (1)
- Shoulder DystociaDocument39 pagesShoulder DystocianormaNo ratings yet
- Cord PresentationDocument24 pagesCord PresentationAmirNo ratings yet
- Physical-Assessment-of-Post-Partum-Mother-MIDTERM NotesDocument27 pagesPhysical-Assessment-of-Post-Partum-Mother-MIDTERM NotesAudrie Allyson Gabales100% (1)
- Vasa Previa - Antenatal Hemorrhage, PregnancyDocument10 pagesVasa Previa - Antenatal Hemorrhage, PregnancyQasimNo ratings yet
- Obstructed LaborDocument4 pagesObstructed Laborkhadzx100% (2)
- DystociaDocument17 pagesDystociaKarinaNo ratings yet
- Hyperemesis GravidarumDocument16 pagesHyperemesis GravidarumGracy Casaña100% (2)
- PlacentaDocument21 pagesPlacentaAttiqaQureshiNo ratings yet
- Hydatidiform MoleDocument3 pagesHydatidiform MoleJny SherpaNo ratings yet
- Retained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateDocument19 pagesRetained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateHartanto Lie100% (1)
- Post Mastectomy ExerciseDocument4 pagesPost Mastectomy ExerciseKusum RoyNo ratings yet
- Ectopic Pregnancy - OMDocument9 pagesEctopic Pregnancy - OMrheind100% (1)
- Joy Zachariah's Case Study.Document11 pagesJoy Zachariah's Case Study.Kuto Yvonne CheronoNo ratings yet
- Psychological Perspective of Abnormal LaborDocument25 pagesPsychological Perspective of Abnormal LaborPriscilla Sarah PayneNo ratings yet
- Abnormal Uterine Bleeding: Case PresentaationDocument15 pagesAbnormal Uterine Bleeding: Case PresentaationGauthamNo ratings yet
- PlacentaDocument59 pagesPlacentaEdna Jenkins100% (9)
- Prematurely Ruptured of Membranes (PROM)Document23 pagesPrematurely Ruptured of Membranes (PROM)NiNie Sie MbakayuNeNo ratings yet
- A Case of Cervical CancerDocument24 pagesA Case of Cervical CancerDebbie beeNo ratings yet
- NSVDDocument48 pagesNSVDchiqui14100% (2)
- Anesthesia and Analgesia: Far Eastern UniversityDocument59 pagesAnesthesia and Analgesia: Far Eastern UniversityAlexandra Duque-DavidNo ratings yet
- Primary Uterine InertiaDocument4 pagesPrimary Uterine InertiaTrisha Cayabyab100% (1)
- OLIGOHYDRAMNIOSDocument3 pagesOLIGOHYDRAMNIOSRuzzel Cabrera-BermonteNo ratings yet
- Oduction: Key Stages of LabourDocument11 pagesOduction: Key Stages of LabournelsonNo ratings yet
- Abortion and Ectopic PregnancyDocument3 pagesAbortion and Ectopic PregnancyJefelson Eu Palaña NahidNo ratings yet
- Nursing Care of A Family During Labor and BirthDocument19 pagesNursing Care of A Family During Labor and BirthPbNo ratings yet
- Abnormal Uterine ActionDocument36 pagesAbnormal Uterine ActionMed PoxNo ratings yet
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
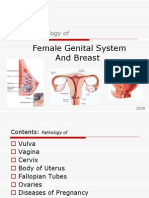
- Pathology ofDocument114 pagesPathology ofRahul Audenesen BratNo ratings yet
- Blood Supply Pelvic OrgansDocument39 pagesBlood Supply Pelvic OrgansoliviaNo ratings yet
- 6th Grade Structure Processes and Responses To Plants 6bDocument9 pages6th Grade Structure Processes and Responses To Plants 6bapi-232424041No ratings yet
- Infertility Concern With Gardasil HPV Vaccine Auto Saved)Document8 pagesInfertility Concern With Gardasil HPV Vaccine Auto Saved)TomGambillNo ratings yet
- Trimix Injection InstructionsDocument3 pagesTrimix Injection InstructionsInfolad1No ratings yet
- Amniocentesis ProcedureDocument6 pagesAmniocentesis ProcedureYenny YuliantiNo ratings yet
- Nepal PosterDocument1 pageNepal Posterapi-282838160No ratings yet
- Sex StoryDocument2 pagesSex Storystopbrag80% (5)
- Anatomy Mid ExamDocument9 pagesAnatomy Mid ExamAji Nikka AngelesNo ratings yet
- Postpartum HemorrhageDocument50 pagesPostpartum HemorrhageSamuel SutantoNo ratings yet
- Pydp 2018-2020Document1 pagePydp 2018-2020sherrylin ginezNo ratings yet
- Karyotype ActivityDocument4 pagesKaryotype ActivityRut ChristineNo ratings yet
- U S. Medical Eligibility Criteria For Contraceptive Use, 2010Document77 pagesU S. Medical Eligibility Criteria For Contraceptive Use, 2010gerte_yuewNo ratings yet
- Placenta Previa: Case DiscussionDocument4 pagesPlacenta Previa: Case DiscussionTin SumangaNo ratings yet
- Jonaliza Empay - Chapter I SummaryDocument9 pagesJonaliza Empay - Chapter I SummaryJones EmpsNo ratings yet
- AbortionDocument92 pagesAbortionniraj_sdNo ratings yet
- CBSE Sample Paper Biology Class XIIDocument10 pagesCBSE Sample Paper Biology Class XIItttomtiaNo ratings yet
- Aphrodisiac Effect of Areca Catechu L. and Pedalium Murex in RatsDocument6 pagesAphrodisiac Effect of Areca Catechu L. and Pedalium Murex in RatsGREESTYNo ratings yet
- Jurnal Keputihan 1Document6 pagesJurnal Keputihan 1Muh AqwilNo ratings yet
- Normal Weight Singleton Gestation Weight Gain ChartDocument1 pageNormal Weight Singleton Gestation Weight Gain ChartmaKitten08No ratings yet
- FAFTA Report 2019Document5 pagesFAFTA Report 2019FAFTA CampaignNo ratings yet
- Antenatal Corticosteroid Therapy Before 24 Weeks.13-1Document11 pagesAntenatal Corticosteroid Therapy Before 24 Weeks.13-1mutya yulindaNo ratings yet
- Information For Women With EndometriosisDocument45 pagesInformation For Women With EndometriosisVhic MuhreeNo ratings yet
- (Methods in Molecular Biology 912) Jacques Cohen, Don Rieger (Auth.), Gary D. Smith, Jason E. Swain, Thomas B. Pool (Eds.) - Embryo Culture - Methods and Protocols-Humana Press (2012) PDFDocument432 pages(Methods in Molecular Biology 912) Jacques Cohen, Don Rieger (Auth.), Gary D. Smith, Jason E. Swain, Thomas B. Pool (Eds.) - Embryo Culture - Methods and Protocols-Humana Press (2012) PDFNkimsearNo ratings yet
- Chapter IDocument38 pagesChapter ILouresa Mae TNo ratings yet
- EMS115810 Vasectomy 1Document14 pagesEMS115810 Vasectomy 1Gia KuteliaNo ratings yet