Abc of Burns: Kanwal Khan Lecturer ZCPT
Abc of Burns: Kanwal Khan Lecturer ZCPT
Download as pptx, pdf, or txt
You might also like
- Classification of FracturesDocument50 pagesClassification of Fracturesmohammad farhanNo ratings yet
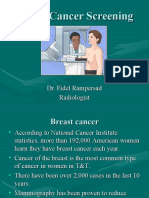
- MammogramDocument55 pagesMammogramShanta BaijooNo ratings yet
- Sofa Score PDFDocument4 pagesSofa Score PDFMadyline VictoryaNo ratings yet
- Nurse Bob's MICU/CCU Survival Guide Critical Care Concepts General Nursing Requirements of The Intensive Care PatientDocument7 pagesNurse Bob's MICU/CCU Survival Guide Critical Care Concepts General Nursing Requirements of The Intensive Care Patientlil' princessNo ratings yet
- BurnsDocument89 pagesBurnsmaila jean50% (2)
- Management of Burn Injuries: Dr. Lawal G.D Registrar, Dept. of Surgery, NHADocument53 pagesManagement of Burn Injuries: Dr. Lawal G.D Registrar, Dept. of Surgery, NHAawesome0% (1)
- Burn - Emergency ManagementDocument28 pagesBurn - Emergency ManagementHira Ashraf100% (1)
- DR TahirDocument61 pagesDR TahirRohail GulNo ratings yet
- Burns ClassificationDocument4 pagesBurns ClassificationNedaAbdullahNo ratings yet
- FrostbiteDocument19 pagesFrostbiteKhadim Hussain Shah100% (2)
- SnakebiteDocument4 pagesSnakebiteallenininiNo ratings yet
- Pressure UlcersDocument38 pagesPressure UlcersRadwa EbedNo ratings yet
- Pressuread Ulcer Prevention Master ClassDocument52 pagesPressuread Ulcer Prevention Master ClassMuhd FaiziNo ratings yet
- Classification of BurnsDocument18 pagesClassification of BurnsLina DsouzaNo ratings yet
- Poisoning & BitesDocument12 pagesPoisoning & BitesJudy HandlyNo ratings yet
- Classification and Management of Open Fractures: DR Ramachandran MS., Dept of Orthopedics, SMS Medical CollegeDocument35 pagesClassification and Management of Open Fractures: DR Ramachandran MS., Dept of Orthopedics, SMS Medical CollegeRamachandran GovindasamyNo ratings yet
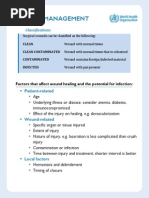
- Wound ManagementDocument4 pagesWound ManagementnrhmhealthNo ratings yet
- Guidelines For Management of Head InjuryDocument18 pagesGuidelines For Management of Head InjuryChellamani UmakanthanNo ratings yet
- Shoulder Dislocation DraftDocument26 pagesShoulder Dislocation Drafthusnajihah18No ratings yet
- Jemal Yimam Jibril Berhanu Kalkidan Zenebe: Presented byDocument57 pagesJemal Yimam Jibril Berhanu Kalkidan Zenebe: Presented byVincent SerNo ratings yet
- Management of Patients With Burn InjuryDocument36 pagesManagement of Patients With Burn Injuryraghad awwad100% (1)
- Student Version Skin Wounds 1119 9 11 13Document68 pagesStudent Version Skin Wounds 1119 9 11 13brandywestonNo ratings yet
- Wound Care Dressings and Their Uses: Carolyn Watts MSN, RN, CWON Vanderbilt University Medical Center Nashville, TNDocument34 pagesWound Care Dressings and Their Uses: Carolyn Watts MSN, RN, CWON Vanderbilt University Medical Center Nashville, TNSuciNo ratings yet
- Shock in Children TutorialDocument37 pagesShock in Children TutorialSsenyonga DominicNo ratings yet
- Heat StrokeDocument2 pagesHeat StrokeshydlNo ratings yet
- Rehabilitation Methods For The Burn Injured Individual PDFDocument25 pagesRehabilitation Methods For The Burn Injured Individual PDFNestor BalboaNo ratings yet
- Anatomical Basis Infection Hand FESSHDocument36 pagesAnatomical Basis Infection Hand FESSHProfesseur Christian DumontierNo ratings yet
- NPWT Renasys and Pico Clinical GuidelinesDocument78 pagesNPWT Renasys and Pico Clinical GuidelinesArdianto SucintaNo ratings yet
- Coronary Artery Disease (Cad) Definition:: Atherosclerosis - AccumulationDocument8 pagesCoronary Artery Disease (Cad) Definition:: Atherosclerosis - AccumulationReiche GomezNo ratings yet
- Nursing CS BurnsDocument1 pageNursing CS BurnsBai Jannah Sahida SilonganNo ratings yet
- OT6 - Amyotrophic Lateral SclerosisDocument19 pagesOT6 - Amyotrophic Lateral SclerosisAnnbe BarteNo ratings yet
- Introduction To Wound CareDocument34 pagesIntroduction To Wound CareRamon Carlo Almiranez100% (1)
- NZONA Traction 2009Document29 pagesNZONA Traction 2009babukiranNo ratings yet
- Lozano Disaster Nursing PDFDocument21 pagesLozano Disaster Nursing PDFDeva Hiyas100% (1)
- School Safety Concept - v.02Document40 pagesSchool Safety Concept - v.02chris annNo ratings yet
- Disorders of Special Senses 2020Document68 pagesDisorders of Special Senses 2020Cres Padua Quinzon100% (1)
- Adult NursingDocument100 pagesAdult NursingAaron Wallace100% (1)
- Endocrin E Diseases: by Group 3Document53 pagesEndocrin E Diseases: by Group 3Ash AshNo ratings yet
- Introduction To Trauma: LSU Medical Student Clerkship, New Orleans, LADocument31 pagesIntroduction To Trauma: LSU Medical Student Clerkship, New Orleans, LAnandang100% (1)
- BurnDocument47 pagesBurnYelle Quilatan100% (1)
- Anatomical Planes: MD Valeria de La Peña GutierrezDocument36 pagesAnatomical Planes: MD Valeria de La Peña GutierrezValeria De la peña100% (1)
- Burn Injury and Its ManagementsDocument86 pagesBurn Injury and Its ManagementsBaraka Sayore0% (1)
- Head Injury OkeDocument42 pagesHead Injury OkeAnonymous p9msXAEwNo ratings yet
- Patient AssessmentDocument5 pagesPatient AssessmentMary Janine Joy RimanoNo ratings yet
- Pain ManagementDocument39 pagesPain ManagementAli Khsheish100% (1)
- Hand Anatomy and Infections NewDocument29 pagesHand Anatomy and Infections NewSaranya RNo ratings yet
- Infection Control: Dept. of Conservative Dentistry & Endodontics, Jodhpur Dental CollegeDocument58 pagesInfection Control: Dept. of Conservative Dentistry & Endodontics, Jodhpur Dental CollegeabhijeetNo ratings yet
- Cardiac Monitoring LectureDocument30 pagesCardiac Monitoring LectureAlma Janella TOSINONo ratings yet
- Chemplast Cuddalore Vinyls Limited: Dengue Awareness ProgrammeDocument16 pagesChemplast Cuddalore Vinyls Limited: Dengue Awareness ProgrammeBala Ganesh100% (1)
- Burns and InjuryDocument27 pagesBurns and InjuryJane Ann Alolod100% (1)
- Type of Wound Dressing (Qeh2 Workshop)Document22 pagesType of Wound Dressing (Qeh2 Workshop)Eric PaulNo ratings yet
- Burn WoundDocument68 pagesBurn WoundjrefkyNo ratings yet
- Medical EmergenciesDocument3 pagesMedical Emergencieskiranvarma2uNo ratings yet
- Wound Dressing: Nor Afifi Syafika Binti Mohd NasirDocument55 pagesWound Dressing: Nor Afifi Syafika Binti Mohd NasirlekhaNo ratings yet
- Type of Wound Dressing1Document31 pagesType of Wound Dressing1Eric PaulNo ratings yet
- Supracondylar FractureDocument53 pagesSupracondylar Fracturedesire kbpNo ratings yet
- Suture PresentationDocument46 pagesSuture Presentationammusuma1999No ratings yet
- Health Assessment ChecklistDocument19 pagesHealth Assessment Checklistramzan aliNo ratings yet
- What Is Traction?Document5 pagesWhat Is Traction?Tweenie DalumpinesNo ratings yet
- BURNSDocument10 pagesBURNSAngeline TaghapNo ratings yet
- Stoma Management: Shankar ZanwarDocument33 pagesStoma Management: Shankar Zanwarpradeep nair100% (1)
- Nursing - Burn InjuryDocument39 pagesNursing - Burn Injuryamaracha2003No ratings yet
- RCT - Masters - 2022Document24 pagesRCT - Masters - 2022Kanwal KhanNo ratings yet
- Measures of Morbidity 2022Document50 pagesMeasures of Morbidity 2022Kanwal KhanNo ratings yet
- Introtoepi 2022Document47 pagesIntrotoepi 2022Kanwal KhanNo ratings yet
- Lect11-Ethics in ResearchDocument27 pagesLect11-Ethics in ResearchKanwal KhanNo ratings yet
- Lect9-Sample Size & Data AnalysisDocument19 pagesLect9-Sample Size & Data AnalysisKanwal KhanNo ratings yet
- Screening - Master - 2022Document57 pagesScreening - Master - 2022Kanwal KhanNo ratings yet
- Confounder, Bias, EM - 2022Document32 pagesConfounder, Bias, EM - 2022Kanwal KhanNo ratings yet
- Cohort - 2022Document20 pagesCohort - 2022Kanwal KhanNo ratings yet
- Lect7 QuestionnaireDesigningDocument38 pagesLect7 QuestionnaireDesigningKanwal KhanNo ratings yet
- Lect4 FormulationofObjectivesDocument16 pagesLect4 FormulationofObjectivesKanwal KhanNo ratings yet
- Lect8 SamplingTechniquesDocument21 pagesLect8 SamplingTechniquesKanwal KhanNo ratings yet
- Lect3 LiteratureReviewDocument33 pagesLect3 LiteratureReviewKanwal KhanNo ratings yet
- Lect5-Case Control Study DesignDocument16 pagesLect5-Case Control Study DesignKanwal KhanNo ratings yet
- Lect4-Cross Sectional Study DesignDocument8 pagesLect4-Cross Sectional Study DesignKanwal KhanNo ratings yet
- Lect5 VariablesDocument13 pagesLect5 VariablesKanwal KhanNo ratings yet
- Lect3-Introduction To Study Designs Desciptive StudiesDocument30 pagesLect3-Introduction To Study Designs Desciptive StudiesKanwal KhanNo ratings yet
- Anterior Shoulder Pain: What Questions Would You Ask in The Subjective Examination?Document3 pagesAnterior Shoulder Pain: What Questions Would You Ask in The Subjective Examination?Kanwal KhanNo ratings yet
- Lect3 DescriptiveEpiPhD2021Document30 pagesLect3 DescriptiveEpiPhD2021Kanwal KhanNo ratings yet
- Passive Movements - KinesiologyDocument18 pagesPassive Movements - KinesiologyKanwal Khan50% (2)
- Trunk and Cervical OrthosisDocument21 pagesTrunk and Cervical OrthosisKanwal Khan100% (1)
- OrthoticsDocument19 pagesOrthoticsKanwal KhanNo ratings yet
- Kinesiology-I: Introduction To Manual Muscle TestingDocument12 pagesKinesiology-I: Introduction To Manual Muscle TestingKanwal Khan100% (1)
- Movt Sci-Ii: Conventional GradingDocument4 pagesMovt Sci-Ii: Conventional GradingKanwal KhanNo ratings yet
- Lect2 ProblemStatementDocument10 pagesLect2 ProblemStatementKanwal KhanNo ratings yet
- Lect1 SelectingResearchTopicDocument18 pagesLect1 SelectingResearchTopicKanwal KhanNo ratings yet
- Oatis - CH08 117 149 PDFDocument33 pagesOatis - CH08 117 149 PDFKanwal KhanNo ratings yet
- Ziauddin College of Physical Therapy Date - Movement Science - Ii Semester Ii AssignmentDocument1 pageZiauddin College of Physical Therapy Date - Movement Science - Ii Semester Ii AssignmentKanwal KhanNo ratings yet
- Manual Physical Therapy, Cervical Traction, and Strengthening Exercises in Patients With Cervical Radiculopathy: A Case SeriesDocument10 pagesManual Physical Therapy, Cervical Traction, and Strengthening Exercises in Patients With Cervical Radiculopathy: A Case SeriesKanwal KhanNo ratings yet
- Biomechanics of Foot and AnkleDocument34 pagesBiomechanics of Foot and AnkleKanwal KhanNo ratings yet
- Anatomy Physiology The Muscular System MCQ QuizDocument32 pagesAnatomy Physiology The Muscular System MCQ QuizKanwal KhanNo ratings yet
- RHIHLIA21168V012021Document7 pagesRHIHLIA21168V012021pizza nmorevikNo ratings yet
- LPPDocument4 pagesLPPMargarida ReisNo ratings yet
- Sleep in Critical Illness Physiology, Assessment, and Its Importance To ICU CareDocument318 pagesSleep in Critical Illness Physiology, Assessment, and Its Importance To ICU Caregwyneth.green.512No ratings yet
- Medical Terminology AbbreviationsDocument11 pagesMedical Terminology Abbreviationsmamona zaheerNo ratings yet
- Post-Sepsis Syndrome: Critical Care Nursing QuarterlyDocument11 pagesPost-Sepsis Syndrome: Critical Care Nursing Quarterlyjonathan moralesNo ratings yet
- Transport of Critically Ill PatientDocument26 pagesTransport of Critically Ill PatientHayatul AkmaLia0% (1)
- 1 s2.0 S1053077022009168 MainDocument8 pages1 s2.0 S1053077022009168 MainOttofianus Alvedo Hewick KalangiNo ratings yet
- NCM118 Lecture 1Document18 pagesNCM118 Lecture 1mirai desuNo ratings yet
- Neuro in The ICUDocument4 pagesNeuro in The ICUEduardo GarciaNo ratings yet
- "Māori" Annotated Bibliography 2-2024 3Document760 pages"Māori" Annotated Bibliography 2-2024 3bonduranNo ratings yet
- Usa Today: Life May Change For Us All'Document28 pagesUsa Today: Life May Change For Us All'Lucia SobralNo ratings yet
- Massachusetts General Hospital's Pre-Admission Testing Area (PATA)Document24 pagesMassachusetts General Hospital's Pre-Admission Testing Area (PATA)marufwaliNo ratings yet
- I. Overview of Informatics and Nursing Informatics InformaticsDocument25 pagesI. Overview of Informatics and Nursing Informatics InformaticsReniella HidalgoNo ratings yet
- ICU Triage (Edit)Document22 pagesICU Triage (Edit)FatyahNo ratings yet
- Icu PsychosisDocument20 pagesIcu PsychosisAryn Phillips100% (1)
- Adaptations To Rehabilitation Services During The Covid-19 Pandemic Proposed by Scientific and Professional Rehabilitation OrganizationsDocument9 pagesAdaptations To Rehabilitation Services During The Covid-19 Pandemic Proposed by Scientific and Professional Rehabilitation Organizationssari murnaniNo ratings yet
- Newer Modes of Ventilation2Document9 pagesNewer Modes of Ventilation2Saradha PellatiNo ratings yet
- Recent Advances in Cardiorespiratory Monitoring in Acute Respiratory Distress Syndrome PatientsDocument11 pagesRecent Advances in Cardiorespiratory Monitoring in Acute Respiratory Distress Syndrome PatientseavasiNo ratings yet
- ICU protocol 2015 قصر العيني by mansdocsDocument227 pagesICU protocol 2015 قصر العيني by mansdocsWalaa YousefNo ratings yet
- OPD Group Insurance PolicyDocument26 pagesOPD Group Insurance PolicyRakshith RaghuNo ratings yet
- Picco Technology Clinical Evidence Brochure en Non - UsDocument25 pagesPicco Technology Clinical Evidence Brochure en Non - UsRichard DaiNo ratings yet
- World Sepsis Day 2021 Webinar SlidesDocument74 pagesWorld Sepsis Day 2021 Webinar Slidessyukri alhamdaNo ratings yet
- Analysis of Laboratory Critical Value Reporting at A Large Academic Medical CenterDocument7 pagesAnalysis of Laboratory Critical Value Reporting at A Large Academic Medical CenterLevi GasparNo ratings yet
- Basics of Mechanical Ventilation. ISBN 3319899805, 978-3319899800Document23 pagesBasics of Mechanical Ventilation. ISBN 3319899805, 978-3319899800meghanleetha100% (16)
- Simplified FenclDocument18 pagesSimplified Fenclrina febriatiNo ratings yet
- The Pediatric Early Warning System Score: A Severity of Illness Score To Predict Urgent Medical Need in Hospitalized ChildrenDocument8 pagesThe Pediatric Early Warning System Score: A Severity of Illness Score To Predict Urgent Medical Need in Hospitalized ChildrenRavikiran SuryanarayanamurthyNo ratings yet
- Deniz 2022Document10 pagesDeniz 2022syakurNo ratings yet
- Copyofresumeicuforstaffnurse Doc 1Document3 pagesCopyofresumeicuforstaffnurse Doc 1api-362213296No ratings yet