Concepts of Critical Care: Gamar Akalal Sugala Clinical Resource Nurse
Concepts of Critical Care: Gamar Akalal Sugala Clinical Resource Nurse
Download as ppt, pdf, or txt
You might also like
- Aota Fieldwork Performance EvaluationDocument6 pagesAota Fieldwork Performance Evaluationapi-699389850No ratings yet
- ORNAC Standards Coordinator Coordonnatrice Coordonnateur Des Normes de LAIISOCDocument8 pagesORNAC Standards Coordinator Coordonnatrice Coordonnateur Des Normes de LAIISOCFrancesca ReyesNo ratings yet
- 2 Adherence To The Clinical Practice 069Document8 pages2 Adherence To The Clinical Practice 069Josh Matthew RosalesNo ratings yet
- NPIDocument8 pagesNPIArt Christian RamosNo ratings yet
- Recovery Room NurseDocument5 pagesRecovery Room NurseChristin 'Kirei' AndoloNo ratings yet
- ShockDocument34 pagesShockeman shNo ratings yet
- PICC Line TroubleshootingDocument67 pagesPICC Line TroubleshootingTatumNo ratings yet
- 2-Safety in PhlebotomyDocument73 pages2-Safety in PhlebotomySymonette OcturaNo ratings yet
- FranklinCovey Continuing Education Course Listing 2019 v1Document16 pagesFranklinCovey Continuing Education Course Listing 2019 v1jorge tizzaNo ratings yet
- QA03005 Critical Testand Critical Result ReportingDocument7 pagesQA03005 Critical Testand Critical Result Reportingdebbie o. azcunaNo ratings yet
- 01 Quality and Patient Safety ProgramDocument25 pages01 Quality and Patient Safety ProgramAnildevraj MbaNo ratings yet
- Guidelines For Sedation and Anesthesia in GI Endos PDFDocument11 pagesGuidelines For Sedation and Anesthesia in GI Endos PDFHernan RuedaNo ratings yet
- Nosocomial Infections: Dr. Tjatur Winarsanto SPPD RST Ciremai CirebonDocument48 pagesNosocomial Infections: Dr. Tjatur Winarsanto SPPD RST Ciremai CirebonNovita Trilianty MagdalenaNo ratings yet
- Documenting ConferringDocument40 pagesDocumenting ConferringDidik Atmojo0% (1)
- Job DescriptionDocument3 pagesJob DescriptionRicanie CadornaNo ratings yet
- Minimal Moderate Sedation StandardsDocument59 pagesMinimal Moderate Sedation StandardsSheila JuddNo ratings yet
- Specimen Collection and ProcessingDocument7 pagesSpecimen Collection and ProcessingJangHanbyul100% (1)
- DIC - RLE #4 For HemaDocument12 pagesDIC - RLE #4 For HemaApril Mae Magos LabradorNo ratings yet
- Ventilator Associated Pneumonia 1Document14 pagesVentilator Associated Pneumonia 1Jennifer ThieleNo ratings yet
- Stroke: AHA/ASA Guidelines For The Early Management of Patients With Acute Ischemic Stroke (2019)Document14 pagesStroke: AHA/ASA Guidelines For The Early Management of Patients With Acute Ischemic Stroke (2019)Natalia OrtizNo ratings yet
- Cardiogenic SyokDocument51 pagesCardiogenic SyokRamadhyanNo ratings yet
- 2017 Syllabus - MVH Modular Sedation SeriesDocument11 pages2017 Syllabus - MVH Modular Sedation SeriesyalahopaNo ratings yet
- Blood Transfusion ReactionDocument9 pagesBlood Transfusion ReactionReema Akberali noorani0% (1)
- Chapter 3 Musculoskeletal System Part 1Document55 pagesChapter 3 Musculoskeletal System Part 1kamalab04100% (1)
- Group 3-DIALYSISDocument62 pagesGroup 3-DIALYSISFesto HakiNo ratings yet
- Emergency Drugs (LEAD)Document8 pagesEmergency Drugs (LEAD)RayePrudenteNo ratings yet
- What Is SBAR?: How Can SBAR Help You?Document12 pagesWhat Is SBAR?: How Can SBAR Help You?Mohamat MutajirNo ratings yet
- 2017 - Guideline Hearth Failure PDFDocument129 pages2017 - Guideline Hearth Failure PDFMarvin M. Vargas AlayoNo ratings yet
- Module Assessment2 Chapter1Document17 pagesModule Assessment2 Chapter1Rena Mae Sison100% (1)
- Outcomes of Ebp Process 2017Document3 pagesOutcomes of Ebp Process 2017api-272725467100% (1)
- Nursing Documentation StandardsDocument27 pagesNursing Documentation StandardsVany Ogin100% (1)
- RN Scopeofpractice May2011Document18 pagesRN Scopeofpractice May2011api-71200129No ratings yet
- Issue 29 - The Nurse Advocate - Hamad Medical Corporation - April 2017Document20 pagesIssue 29 - The Nurse Advocate - Hamad Medical Corporation - April 2017Brent ForemanNo ratings yet
- Registration and Billing System &CSSDDocument4 pagesRegistration and Billing System &CSSDSthitapragyan senapatiNo ratings yet
- 3 TK1 T5-Draft Policies and Procedures For The Antimicrobial Stewardship Program FinalDocument5 pages3 TK1 T5-Draft Policies and Procedures For The Antimicrobial Stewardship Program FinalMt. CarmelNo ratings yet
- Laboratory1 Safety and Infection ControlDocument74 pagesLaboratory1 Safety and Infection ControlRyu ddaengNo ratings yet
- Sepsis: Pathophysiology and Management in The ICUDocument38 pagesSepsis: Pathophysiology and Management in The ICUprashsubbuNo ratings yet
- Report - Planning For The Nursing ServiceDocument4 pagesReport - Planning For The Nursing ServiceAnj GaliNo ratings yet
- Diagnostic TestDocument40 pagesDiagnostic TestLimYi100% (1)
- Specimen Collection and Transporation Instructions-1Document6 pagesSpecimen Collection and Transporation Instructions-1Marvel Vision100% (1)
- Konferensi PerawatDocument159 pagesKonferensi PerawatdroenNo ratings yet
- CLCGP030 Theatre Operating List Session Scheduling PolicyDocument19 pagesCLCGP030 Theatre Operating List Session Scheduling PolicyJeffy PuruggananNo ratings yet
- Medical Record Review ToolsDocument10 pagesMedical Record Review ToolstopNo ratings yet
- Job Description:: Phlebotomists DutiesDocument7 pagesJob Description:: Phlebotomists DutiesRajeev PareekNo ratings yet
- Introduction To Critical Care NursingDocument13 pagesIntroduction To Critical Care NursingRAIHANNo ratings yet
- Ebook A Guide To Improving Your Patient Safety Event Reporting Culture Plus A Leadership Action ListDocument8 pagesEbook A Guide To Improving Your Patient Safety Event Reporting Culture Plus A Leadership Action ListJery JsNo ratings yet
- CPG Management of Post-Operative Infectious EndophthalmitisDocument41 pagesCPG Management of Post-Operative Infectious EndophthalmitisnrajentranNo ratings yet
- Pre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIDocument25 pagesPre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIFatima MNo ratings yet
- 4 Safe Transfusion Right Blood Right Patient Right Time and Right PlaceDocument11 pages4 Safe Transfusion Right Blood Right Patient Right Time and Right PlaceEtrya Wianda100% (1)
- A Model For Reducing Medical ErrorsDocument4 pagesA Model For Reducing Medical ErrorsPinto PintoNo ratings yet
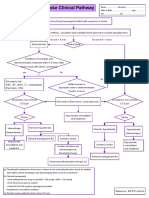
- Stroke Clinical PathwayDocument1 pageStroke Clinical PathwayKanoknun PisitpatcaragulNo ratings yet
- Quality Control in Clinical LaboratoryDocument4 pagesQuality Control in Clinical Laboratorymuleraviraj01No ratings yet
- Just Culture: Theory and PracticeDocument13 pagesJust Culture: Theory and PracticeSouheil DamajNo ratings yet
- Nabl Cap Accreditation ProcessDocument42 pagesNabl Cap Accreditation ProcessCOMET ENVIRONS PVT LTDNo ratings yet
- Environmental SurveillanceDocument11 pagesEnvironmental Surveillancedr rajoreNo ratings yet
- Canadian Accreditation ToolsDocument70 pagesCanadian Accreditation ToolsAbdur Rashid KhanNo ratings yet
- Crossmatching Procedure PDFDocument2 pagesCrossmatching Procedure PDFgreatgeniusNo ratings yet
- ChecklistDocument12 pagesChecklistNethera Kiza ImperialNo ratings yet
- Nursing Leadersip and Management: - ControllingDocument42 pagesNursing Leadersip and Management: - ControllingGee Cee Odero100% (1)
- Clinical Governance Strategy A Complete Guide - 2020 EditionFrom EverandClinical Governance Strategy A Complete Guide - 2020 EditionNo ratings yet
- Outlines of CME/PD Activities: WorkshopDocument3 pagesOutlines of CME/PD Activities: WorkshopGummie Akalal SugalaNo ratings yet
- Nurses' Job Burnout and Job Satisfaction During The COVID-19 Pandemic in The PhilippinesDocument14 pagesNurses' Job Burnout and Job Satisfaction During The COVID-19 Pandemic in The PhilippinesGummie Akalal SugalaNo ratings yet
- 6 Doctor of Philosophy in Nursing Education Cur Rev 2015Document2 pages6 Doctor of Philosophy in Nursing Education Cur Rev 2015Gummie Akalal SugalaNo ratings yet
- Hand-Over Summary: No. Simulation Activities Administration Date Details CommentsDocument4 pagesHand-Over Summary: No. Simulation Activities Administration Date Details CommentsGummie Akalal SugalaNo ratings yet
- Management by Objective Approach in Nursing Performance Appraisal and Its Impact On Quality of Nursing CareDocument13 pagesManagement by Objective Approach in Nursing Performance Appraisal and Its Impact On Quality of Nursing CareGummie Akalal SugalaNo ratings yet
- Ngos and Government Partnership For Health Systems Strengthening: A Qualitative Study Presenting Viewpoints of Government, Ngos and Donors in PakistanDocument8 pagesNgos and Government Partnership For Health Systems Strengthening: A Qualitative Study Presenting Viewpoints of Government, Ngos and Donors in PakistanGummie Akalal SugalaNo ratings yet
- Clinical Simulation Administration: Executive Administration of Academic Affairs and Training in Collaboration WithDocument5 pagesClinical Simulation Administration: Executive Administration of Academic Affairs and Training in Collaboration WithGummie Akalal SugalaNo ratings yet
- Renewal Passport Application Form (Adult) : Department of Foreign AffairsDocument2 pagesRenewal Passport Application Form (Adult) : Department of Foreign AffairsGummie Akalal SugalaNo ratings yet
- Venue Evaluation FormDocument2 pagesVenue Evaluation FormGummie Akalal SugalaNo ratings yet
- MRN Date Primary Nurse 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21Document1 pageMRN Date Primary Nurse 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21Gummie Akalal SugalaNo ratings yet
- Corses Clasficatn - 3 DocsDocument3 pagesCorses Clasficatn - 3 DocsGummie Akalal SugalaNo ratings yet
- Nursing Case Study Evaluation SheetDocument1 pageNursing Case Study Evaluation SheetGummie Akalal SugalaNo ratings yet
- C2P2 Updated 2 DaysDocument4 pagesC2P2 Updated 2 DaysGummie Akalal SugalaNo ratings yet
- August 2018.: AchievementsDocument3 pagesAugust 2018.: AchievementsGummie Akalal SugalaNo ratings yet
- SDFHKDocument4 pagesSDFHKGummie Akalal SugalaNo ratings yet
- Essential Safety Requirements: Security Forces Hospital Program Makkah ESR GuideDocument24 pagesEssential Safety Requirements: Security Forces Hospital Program Makkah ESR GuideGummie Akalal SugalaNo ratings yet
- The Following Daily Assessment Were Not AUTHIRIZED by The Primary Nurse After The ShiftDocument2 pagesThe Following Daily Assessment Were Not AUTHIRIZED by The Primary Nurse After The ShiftGummie Akalal SugalaNo ratings yet
- Daily Log of ActivitiesDocument1 pageDaily Log of ActivitiesGummie Akalal SugalaNo ratings yet
- DDFFDocument1 pageDDFFGummie Akalal SugalaNo ratings yet
- Methodology: Boiling of The Shells To Be BrittleDocument2 pagesMethodology: Boiling of The Shells To Be BrittleGummie Akalal SugalaNo ratings yet
- EeeDocument4 pagesEeeGummie Akalal SugalaNo ratings yet
- Clinical Simulation Administration (CSA) Activities' Brief ReportDocument3 pagesClinical Simulation Administration (CSA) Activities' Brief ReportGummie Akalal SugalaNo ratings yet
- Kamc Csicu Kamc Csicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc NicuDocument3 pagesKamc Csicu Kamc Csicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc Nicu Kamc NicuGummie Akalal SugalaNo ratings yet
- 1B Approval Form PDFDocument1 page1B Approval Form PDFGummie Akalal SugalaNo ratings yet
- CONFLICT Perception of Incompatible AspirationsDocument8 pagesCONFLICT Perception of Incompatible AspirationsGummie Akalal SugalaNo ratings yet
- Every Good Act Is Charity 1Document2 pagesEvery Good Act Is Charity 1Gummie Akalal SugalaNo ratings yet
- The Power of Love Unites All Religion 1Document3 pagesThe Power of Love Unites All Religion 1Gummie Akalal SugalaNo ratings yet
- Dept of Health Budget PresentationDocument14 pagesDept of Health Budget PresentationWVXU NewsNo ratings yet
- Guide NbdeDocument36 pagesGuide NbdeLeShaggy DonatelloNo ratings yet
- High Risk NeonateDocument102 pagesHigh Risk NeonateJaya Prabha100% (2)
- Uiip Flu Fact SheetDocument4 pagesUiip Flu Fact Sheetapi-277123092No ratings yet
- Nursing Grand Rounds Reviewer PDFDocument17 pagesNursing Grand Rounds Reviewer PDFAlyssa Jade GolezNo ratings yet
- Asgct 19th Annual Meeting ProgramDocument14 pagesAsgct 19th Annual Meeting ProgramQ-MT Branch HQ 497 OM&MNo ratings yet
- Clinical Nutrition: Course ContentDocument46 pagesClinical Nutrition: Course ContentUNITED HOSPITAL OF AFRICANo ratings yet
- Gynaecology - Topical Past Papers (2007-2019)Document34 pagesGynaecology - Topical Past Papers (2007-2019)Mahad WyneNo ratings yet
- Hemangioma Propranolol GuidelineDocument2 pagesHemangioma Propranolol GuidelineSake Cinema21No ratings yet
- Rheumatology ReviewDocument37 pagesRheumatology Reviewkarar AhmedNo ratings yet
- Problems Questions With Answers 2020 Incidence PrevalenceDocument3 pagesProblems Questions With Answers 2020 Incidence PrevalenceKhaleedNo ratings yet
- Accessible, Affordable and Quality Healthcare For All: Sector ProfileDocument50 pagesAccessible, Affordable and Quality Healthcare For All: Sector ProfileswajitmishraNo ratings yet
- Natalie Alwin BMT Resume SusieDocument1 pageNatalie Alwin BMT Resume Susieapi-340258456No ratings yet
- Hand Hygiene Policy 8.0Document20 pagesHand Hygiene Policy 8.0Nasradin AhmedNo ratings yet
- Managing Academic Anxiety: Presented By: Undergraduate Advising& Academic SupportDocument27 pagesManaging Academic Anxiety: Presented By: Undergraduate Advising& Academic SupportRamonaMihaelaNo ratings yet
- Emergency Room Reflection PaperDocument3 pagesEmergency Room Reflection PaperRoshin TejeroNo ratings yet
- Students Worksheet 9 English For Nursing - Corona Virus Covid-19Document5 pagesStudents Worksheet 9 English For Nursing - Corona Virus Covid-19Ihat SholihatNo ratings yet
- Health Talk On Testicular ExaminationDocument18 pagesHealth Talk On Testicular ExaminationrumasadraunaNo ratings yet
- ABO Grouping - Overview, Clinical Indications - Applications, Test PerformanceDocument7 pagesABO Grouping - Overview, Clinical Indications - Applications, Test PerformanceleandroNo ratings yet
- Pru Treasure Flexi II Brochure (01 July 2023)Document29 pagesPru Treasure Flexi II Brochure (01 July 2023)Darren ChenNo ratings yet
- TCCC Skill Sets by Responder Level Master 190422 ApprovedDocument4 pagesTCCC Skill Sets by Responder Level Master 190422 ApprovedIon MarinNo ratings yet
- Dental Abscess - Symptoms, Diagnosis and Treatment - BMJ Best PracticeDocument1 pageDental Abscess - Symptoms, Diagnosis and Treatment - BMJ Best PracticeTri Sakti Sunda RomdhoniNo ratings yet
- MasarwehDocument3 pagesMasarwehapi-507112896No ratings yet
- NPD, PA and EPLDocument57 pagesNPD, PA and EPLVikhilPatelNo ratings yet
- ScriptDocument3 pagesScriptJamjam AguilaNo ratings yet
- Ateneo de Zamboanga University: Level IiDocument7 pagesAteneo de Zamboanga University: Level IiNur SetsuNo ratings yet
- Evidence Based PracticeDocument5 pagesEvidence Based PracticeDhanesh Verma100% (2)
- 5th ReflectionDocument2 pages5th Reflectionapi-478150357No ratings yet