Peritonitis: Presentan: FAUZAN AKBAR YUSYAHADI - 12100118191
Peritonitis: Presentan: FAUZAN AKBAR YUSYAHADI - 12100118191
Download as ppt, pdf, or txt
You might also like
- Indications of Upper GI EndosDocument25 pagesIndications of Upper GI EndosDrTanta100% (3)
- Esophageal and Gastric VaricesDocument15 pagesEsophageal and Gastric VaricesDumbo D' CatNo ratings yet
- Appendix Chapter, Sabiston Textbook of SurgeryDocument43 pagesAppendix Chapter, Sabiston Textbook of SurgeryShuo Huang100% (2)
- Basic Emergency Skills in Trauma Part 3 - Penetrating Abdoninal Injury - Dr. Oliver BelarmaDocument3 pagesBasic Emergency Skills in Trauma Part 3 - Penetrating Abdoninal Injury - Dr. Oliver BelarmaRaquel ReyesNo ratings yet
- PeritonitissDocument46 pagesPeritonitissNinaNo ratings yet
- Acute PeritonitisDocument4 pagesAcute PeritonitisSatrio Tri HadmokoNo ratings yet
- PeritonitisDocument42 pagesPeritonitisvriliadiar100% (1)
- Immune System. It's Possible That A Virus or Bacterium May Trigger Crohn's DiseaseDocument11 pagesImmune System. It's Possible That A Virus or Bacterium May Trigger Crohn's DiseaseZulfiana RahayuNo ratings yet
- Acute Limb Ischemia SiteDocument23 pagesAcute Limb Ischemia Sitebenypermadi100% (2)
- Hernia - Surgery PrecisDocument1 pageHernia - Surgery PrecisSherif WagdyNo ratings yet
- Radiology Imaging of Urinary TractDocument40 pagesRadiology Imaging of Urinary TractMuhammad Zaniar RamadhaniNo ratings yet
- Chole SysDocument8 pagesChole SysKas MulyadiNo ratings yet
- Acute AbdomenDocument58 pagesAcute AbdomenkharisaNo ratings yet
- Upper Endos PDFDocument6 pagesUpper Endos PDFTeky WidyariniNo ratings yet
- Clinical Practice Guideline For The Management of Anorectal Abscess Fistula-In-Ano and Rectovaginal FistulaDocument17 pagesClinical Practice Guideline For The Management of Anorectal Abscess Fistula-In-Ano and Rectovaginal FistulaAlivia HanumNo ratings yet
- SURGERY Lecture 3 - Abdominal Hernia (Dr. Mendoza)Document12 pagesSURGERY Lecture 3 - Abdominal Hernia (Dr. Mendoza)Medisina101100% (1)
- 1 PeritonitisDocument26 pages1 PeritonitisGizachew AsimareNo ratings yet
- Peritonitis: Signs and Symptoms of Peritonitis IncludeDocument4 pagesPeritonitis: Signs and Symptoms of Peritonitis IncludeCharlene Rose Tavarro BarreraNo ratings yet
- Acute AbdomenDocument19 pagesAcute AbdomenNazmi Z. MehmetiNo ratings yet
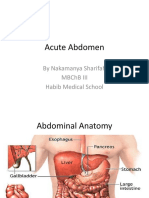
- Acute Abdomen: by Nakamanya Sharifah MBCHB Iii Habib Medical SchoolDocument48 pagesAcute Abdomen: by Nakamanya Sharifah MBCHB Iii Habib Medical SchoolNina100% (1)
- Polycystic Kidney DiseaseDocument9 pagesPolycystic Kidney DiseaseCésar Aguilar ContrerasNo ratings yet
- Umbilical HerniaDocument19 pagesUmbilical HerniabonopazioNo ratings yet
- Inguinal Scrotal SwellingsDocument23 pagesInguinal Scrotal SwellingsAzmyza Azmy100% (1)
- Chronic Limb Ischaemia: MR Hanif Hussein Consultant Vascular Surgeon, HKLDocument35 pagesChronic Limb Ischaemia: MR Hanif Hussein Consultant Vascular Surgeon, HKLZulzaire ZulkefliNo ratings yet
- A Case Presentation On AppendecitisDocument30 pagesA Case Presentation On AppendecitisrodericpalanasNo ratings yet
- Colonoscopy ProcedureDocument3 pagesColonoscopy Procedurejmarcos84100% (1)
- DiverticulitisDocument34 pagesDiverticulitisSahirNo ratings yet
- Acute and Chronic Gastrointestinal BleedingDocument7 pagesAcute and Chronic Gastrointestinal BleedingMarwan M.100% (1)
- Summary For Acute AppendicitisDocument13 pagesSummary For Acute AppendicitisFemale calmNo ratings yet
- Guidelines SBO (Small Bowel Obstruction)Document14 pagesGuidelines SBO (Small Bowel Obstruction)Ghege GuntaranNo ratings yet
- Penetrating Abdominal TraumaDocument67 pagesPenetrating Abdominal TraumarizkaNo ratings yet
- Appendectomy in BPJSDocument29 pagesAppendectomy in BPJSRinthoNo ratings yet
- Diverticular DiseaseDocument30 pagesDiverticular Diseasept.mahmoudNo ratings yet
- CHolelitiasis, CholesistitisDocument44 pagesCHolelitiasis, CholesistitistrianaamaliaNo ratings yet
- Chapter 31 - Duodenal and Intestinal Atresia and Stenosis PDFDocument16 pagesChapter 31 - Duodenal and Intestinal Atresia and Stenosis PDFArdi Suhardjo100% (1)
- Surgicl Pathology of OesophagusDocument91 pagesSurgicl Pathology of Oesophagusmikaaa000No ratings yet
- Acute Abdomen and PeritonitisDocument17 pagesAcute Abdomen and PeritonitisAsuri KrishnaNo ratings yet
- Stoma Examination OSCE GuideDocument5 pagesStoma Examination OSCE GuideEssa AfridiNo ratings yet
- 21 Obstructive JaundiceDocument12 pages21 Obstructive JaundicejumaymayaNo ratings yet
- HERNIORRHAPHYDocument2 pagesHERNIORRHAPHYSheldon Deypalubos Jr.No ratings yet
- Renal TumorsDocument38 pagesRenal TumorsMim Rashed0% (1)
- HydroceleDocument39 pagesHydroceleNd Eye100% (2)
- IntussusceptionDocument33 pagesIntussusceptionNovendi RizkaNo ratings yet
- Gastrectomy 1Document86 pagesGastrectomy 1Mysnow OpalNo ratings yet
- GangreneDocument18 pagesGangreneFelita Surya RiniNo ratings yet
- Penetrating Abdominal Trauma Emergency ManagementDocument29 pagesPenetrating Abdominal Trauma Emergency Managementanjali singhNo ratings yet
- PeritonitisDocument11 pagesPeritonitisMihir PatelNo ratings yet
- Hypertrophic Pyloric StenosisDocument17 pagesHypertrophic Pyloric StenosisMohammed Fareed100% (1)
- Wrist Fractures: Musculoskeletal TraumaDocument4 pagesWrist Fractures: Musculoskeletal TraumaDewina Dyani Rosari IINo ratings yet
- BPH - Pathophysiology and EvaluationDocument80 pagesBPH - Pathophysiology and EvaluationJulfikar KhanNo ratings yet
- JP US IntussusceptionDocument52 pagesJP US IntussusceptionJoshua PulinatNo ratings yet
- Genito Urinary Disorder LectureDocument64 pagesGenito Urinary Disorder LectureIrzan GustantoNo ratings yet
- Malunion Delayed Union and Nonunion FracturesDocument31 pagesMalunion Delayed Union and Nonunion FracturesRasjad ChairuddinNo ratings yet
- Case Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyDocument46 pagesCase Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyAjiMary M. DomingoNo ratings yet
- Hirschprung Disease: Department of Radiology Medical Faculty of Hasanuddin University, MakassarDocument15 pagesHirschprung Disease: Department of Radiology Medical Faculty of Hasanuddin University, Makassardewi sartikaNo ratings yet
- All Previous Essay SurgeryDocument170 pagesAll Previous Essay Surgeryalsfyabdullah2021100% (1)
- Head & Neck: Most CommonDocument6 pagesHead & Neck: Most CommonJüdith Marie Reyes BauntoNo ratings yet
- Nursing Assessment: Patient History, An Infant or A Child May Be Relatively Free From Symptom Until She or He CriesDocument4 pagesNursing Assessment: Patient History, An Infant or A Child May Be Relatively Free From Symptom Until She or He Criescyrilcarinan100% (1)
- Hirschsprung's Disease - AthigamanDocument128 pagesHirschsprung's Disease - Athigamanprived100% (4)
- Acute Cellulitis and Erysipelas in Adults - Treatment - UpToDateDocument28 pagesAcute Cellulitis and Erysipelas in Adults - Treatment - UpToDateYahir PerezNo ratings yet
- Mid TermDocument17 pagesMid TermTamoghna NaskarNo ratings yet
- Feasibility of Neuromuscular Electrical StimulatioDocument201 pagesFeasibility of Neuromuscular Electrical StimulatiolarissacrhfisioterapiaNo ratings yet
- Cefepime Vs Zosyn For Empiric Sepsis CoverageDocument2 pagesCefepime Vs Zosyn For Empiric Sepsis Coveragetl drNo ratings yet
- Septic ShockDocument16 pagesSeptic ShockGelo JvrNo ratings yet
- Hemodynamic Disorders, Thrombosis and ShockDocument40 pagesHemodynamic Disorders, Thrombosis and ShockAndi Tri NugrahaNo ratings yet
- Nutrisi Pasien ICUDocument25 pagesNutrisi Pasien ICUmichaelarshantyNo ratings yet
- NURS 328: Understanding Research: Assignment 1 Facilitating Evidence-Based Practice: Dissemination ProjectDocument11 pagesNURS 328: Understanding Research: Assignment 1 Facilitating Evidence-Based Practice: Dissemination ProjectKuharaj TharmakulasinghamNo ratings yet
- Critical Care of The Burn Patient - The First 48 HoursDocument14 pagesCritical Care of The Burn Patient - The First 48 HoursAndre MessiasNo ratings yet
- Management of Severe Spreading Odontogenic Infection in Third Trimester of Pregnancy: A Case ReportDocument5 pagesManagement of Severe Spreading Odontogenic Infection in Third Trimester of Pregnancy: A Case ReportrindaNo ratings yet
- Patofisiologi Luka BakarDocument34 pagesPatofisiologi Luka BakarRut HutagaolNo ratings yet
- Fast Hug in Bed PleaseDocument7 pagesFast Hug in Bed PleaseGuillermo Obando LaraNo ratings yet
- Soni 2010Document4 pagesSoni 2010AlejandroVeraVargasNo ratings yet
- Icu BookDocument140 pagesIcu BookRaMy “MhMd” ElaRabyNo ratings yet
- Referensi Nilai KritisDocument9 pagesReferensi Nilai KritisFaiz AchmadNo ratings yet
- 10-Article Text-26-1-10-20170412Document5 pages10-Article Text-26-1-10-20170412naeem186No ratings yet
- 132 Emergency MedicineDocument14 pages132 Emergency MedicineVania NandaNo ratings yet
- Meningitis JournalDocument5 pagesMeningitis JournalFaza KahfiNo ratings yet
- Rekapitulasi Laporan Kematian Dari Januari 2020 - Juni 2020Document45 pagesRekapitulasi Laporan Kematian Dari Januari 2020 - Juni 2020muhammad ilmanNo ratings yet
- Post-Operative Care, DSTC Online, Jun.2021Document38 pagesPost-Operative Care, DSTC Online, Jun.2021tepat rshsNo ratings yet
- Final Exam National Board of Examinations JUNE 2020 Pathology Paper-I Time: 3 Hours PATH/J/20/32/I MAX. MARKS: 100 Important InstructionsDocument1 pageFinal Exam National Board of Examinations JUNE 2020 Pathology Paper-I Time: 3 Hours PATH/J/20/32/I MAX. MARKS: 100 Important InstructionsSrinivas PingaliNo ratings yet
- Systemic in Ammatory Response Syndrome (SIRS) : Where Did It Come From and Is It Still Relevant Today?Document8 pagesSystemic in Ammatory Response Syndrome (SIRS) : Where Did It Come From and Is It Still Relevant Today?Jhanu JaguarNo ratings yet
- CVP MonitoringDocument24 pagesCVP MonitoringsofiamansoorNo ratings yet
- PancreatitisDocument12 pagesPancreatitisjhodane100% (4)
- Febre No Pos OperatorioDocument4 pagesFebre No Pos OperatorioRafaelNo ratings yet
- Ob/Neonatal Liability IssuesDocument107 pagesOb/Neonatal Liability IssuesCamille DiCostanzo PickelNo ratings yet
- ShockDocument72 pagesShockWOne Wann100% (1)
- (Intubate!) : Stag e Description GFR (Ml/min/1.73Document7 pages(Intubate!) : Stag e Description GFR (Ml/min/1.73Jamie PalmeriNo ratings yet
- Pathophysiology and History of Diabetic Septic FootDocument8 pagesPathophysiology and History of Diabetic Septic Footahmed ebrahimNo ratings yet
- Basic Concepts in SurgeryDocument13 pagesBasic Concepts in Surgerysk0% (1)