Anemias: Clinical Pharmacy
Anemias: Clinical Pharmacy
Download as pptx, pdf, or txt
You might also like
- Urn - 00760065 - IgDocument1 pageUrn - 00760065 - IgsaleemNo ratings yet
- PallorDocument16 pagesPallorManal AlQuaimi100% (1)
- Comply With Infection Prevention and Control Policies and ProceduresDocument42 pagesComply With Infection Prevention and Control Policies and Procedurespavan0% (1)
- Liabilities of PhysiciansDocument7 pagesLiabilities of PhysiciansRem Alfelor100% (2)
- Anemia: Presented byDocument36 pagesAnemia: Presented byParmvir Singh100% (1)
- Nutritional AnemiaDocument53 pagesNutritional AnemiaANUREET KAURNo ratings yet
- Hyproliferative Anemias: What Is Anemia?Document15 pagesHyproliferative Anemias: What Is Anemia?yamie sulongNo ratings yet
- AnaemiaDocument61 pagesAnaemiaArathyNo ratings yet
- NCLEX Drugs For AnemiaDocument9 pagesNCLEX Drugs For AnemiajthsNo ratings yet
- GGFHGFJKL KJKHGFDGHJKLDocument14 pagesGGFHGFJKL KJKHGFDGHJKLVania Millenia MelindaNo ratings yet
- 8 AnemiaDocument31 pages8 AnemiaVenom LyteNo ratings yet
- AnemiaDocument57 pagesAnemiaSandhya BasnetNo ratings yet
- ANEMIADocument35 pagesANEMIASaurabhi SharmaNo ratings yet
- ANEMIA ملونة كاملةDocument19 pagesANEMIA ملونة كاملةArcangela QuaintrelleNo ratings yet
- Salinan Terjemahan 307211717 Laporan Pendahuluan AnemiaDocument16 pagesSalinan Terjemahan 307211717 Laporan Pendahuluan AnemiaRidho HidayatullahNo ratings yet
- Ms. Tashmera P. Datukali: Mindanao State University Buug Campus - Ipil Extension Sanito, Ipil, Zamboanga Sibugay ProvinceDocument12 pagesMs. Tashmera P. Datukali: Mindanao State University Buug Campus - Ipil Extension Sanito, Ipil, Zamboanga Sibugay Provincesandro2000No ratings yet
- AnemiaDocument92 pagesAnemiasangeetachatterjee100% (1)
- AnemiaDocument71 pagesAnemiaAnsu MaliyakalNo ratings yet
- Presentation 1Document73 pagesPresentation 1ابراهيم محمدNo ratings yet
- Red Blood Cells DisordersDocument70 pagesRed Blood Cells Disordersluna zeidNo ratings yet
- Gorres, Sierra MaeDocument4 pagesGorres, Sierra MaegorresNo ratings yet
- AnemiaDocument31 pagesAnemiamehtahrridayNo ratings yet
- Anaemia by Haider AliDocument38 pagesAnaemia by Haider AliAbdul SamadNo ratings yet
- L1 HematologyDocument49 pagesL1 Hematologyalisafaa1281No ratings yet
- AnemiaDocument33 pagesAnemiaJasmine Thabith100% (8)
- AntmiaDocument85 pagesAntmiafrendirachmadNo ratings yet
- ANEMIADocument4 pagesANEMIAcabelin randy amenNo ratings yet
- Anemia GDocument47 pagesAnemia GkalfNo ratings yet
- Anemia NevinDocument69 pagesAnemia NevinAbdallah AlasalNo ratings yet
- ANAEMIA_31-10-23_dr.TUGUDocument26 pagesANAEMIA_31-10-23_dr.TUGUataya2442No ratings yet
- Anemia: Prepared byDocument20 pagesAnemia: Prepared byAishah MalikNo ratings yet
- AnemiaDocument103 pagesAnemiaAhemigishaNo ratings yet
- Anaemia002Document8 pagesAnaemia002Motea AlawlaqiNo ratings yet
- Cap 13Document88 pagesCap 13Saul RivasNo ratings yet
- Anemia of Diminished ErythropoiesisDocument43 pagesAnemia of Diminished ErythropoiesisJared Khoo Er HauNo ratings yet
- Lec 1Document4 pagesLec 1Sajjad FalahNo ratings yet
- HEMATOLOGIC DISORDERS (AutoRecovered)Document68 pagesHEMATOLOGIC DISORDERS (AutoRecovered)newsletteremail.blcckchain.comNo ratings yet
- AnemiasDocument18 pagesAnemiashussein alnasryNo ratings yet
- Anaemia: DR Adjugah J. U. B. Med Sci (Physiology), MBBS, FMCFM, Mph. Consultant Family PhysicianDocument78 pagesAnaemia: DR Adjugah J. U. B. Med Sci (Physiology), MBBS, FMCFM, Mph. Consultant Family PhysicianAkwu AkwuNo ratings yet
- AnaemiaDocument17 pagesAnaemiatooba hussainNo ratings yet
- Dental Considerations in Hematological DisordersDocument21 pagesDental Considerations in Hematological DisordersMariya FatmaNo ratings yet
- Anemia in PregnancyDocument33 pagesAnemia in PregnancyKomal Dhulap100% (1)
- 1 Anemia PDDocument40 pages1 Anemia PDአንዋርጀማልNo ratings yet
- Module 7 HEMATOLOGIC DISORDERSDocument60 pagesModule 7 HEMATOLOGIC DISORDERSMaclenard merinNo ratings yet
- ANEMIADocument81 pagesANEMIAArvin HermosoNo ratings yet
- Anemia During PregnancyDocument39 pagesAnemia During PregnancyBhawna JoshiNo ratings yet
- Drug Treatment of AnemiasDocument29 pagesDrug Treatment of AnemiasKashmala100% (1)
- Presentation On Blood DisordersDocument122 pagesPresentation On Blood Disordersvarshasharma05No ratings yet
- AnemiaDocument7 pagesAnemiaKabirNo ratings yet
- AnemiaDocument7 pagesAnemiaمحمد حميدNo ratings yet
- Childhood Anaemia (Nutritional)Document66 pagesChildhood Anaemia (Nutritional)Emereole FrancesNo ratings yet
- Hematology and Oncology 1 Lyst1717831134671Document99 pagesHematology and Oncology 1 Lyst1717831134671jdjxwsncvdNo ratings yet
- Nama: Teguh Pentana NIM: 16330107 Mata Kuliah: Farmakoterapi Kelas: DDocument20 pagesNama: Teguh Pentana NIM: 16330107 Mata Kuliah: Farmakoterapi Kelas: DteguhxletNo ratings yet
- Anemia (HT & PE)Document8 pagesAnemia (HT & PE)Karina DesianaNo ratings yet
- Anaemia - THE MULASDocument60 pagesAnaemia - THE MULASabrahammwansa2No ratings yet
- Therapeutic Choices 2011Document1,365 pagesTherapeutic Choices 2011priyarajan007No ratings yet
- Case Study Notes - FinalDocument11 pagesCase Study Notes - FinalAlex LiganNo ratings yet
- انيماDocument59 pagesانيمااحمد احمدNo ratings yet
- Anemia Dr. I. Cadiz MDocument28 pagesAnemia Dr. I. Cadiz Mdoc_ircmNo ratings yet
- Anaemia'sDocument27 pagesAnaemia'sRayan100% (4)
- Anemia NotesDocument8 pagesAnemia Notesalin malekNo ratings yet
- Hypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Types Of Hemolytic Anemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandTypes Of Hemolytic Anemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Hypopituitarism: Dr. Rasikapriya First Year PaediatricsDocument34 pagesHypopituitarism: Dr. Rasikapriya First Year PaediatricsReshu ThakuriNo ratings yet
- Hyperemesis Gravidarum: Prepared By:-Mr. Arkab Khan PathanDocument22 pagesHyperemesis Gravidarum: Prepared By:-Mr. Arkab Khan PathanReshu ThakuriNo ratings yet
- Approach To The Child With Anemia: Official Reprint From UptodateDocument39 pagesApproach To The Child With Anemia: Official Reprint From UptodateReshu ThakuriNo ratings yet
- Rectal Prolapse: DR Anas Ahmad PGR - Surgical Unit 2 Shalamar Hospital-LahoreDocument37 pagesRectal Prolapse: DR Anas Ahmad PGR - Surgical Unit 2 Shalamar Hospital-LahoreReshu ThakuriNo ratings yet
- (Dwarfism) : Regents BiologyDocument23 pages(Dwarfism) : Regents BiologyReshu ThakuriNo ratings yet
- Anaemi A: Joshi Abhishek Ashvinbhai F.Y.P.B.B.Sc - Nursing Govt - College of Nursing JamnagarDocument82 pagesAnaemi A: Joshi Abhishek Ashvinbhai F.Y.P.B.B.Sc - Nursing Govt - College of Nursing JamnagarReshu ThakuriNo ratings yet
- Time Management 3 NewDocument23 pagesTime Management 3 NewMount Saipal International AcademyNo ratings yet
- Exercise Week 14 (Pages 128-137)Document11 pagesExercise Week 14 (Pages 128-137)YATTNo ratings yet
- Pertinent Provisions of PD 603Document14 pagesPertinent Provisions of PD 603Frederick EboñaNo ratings yet
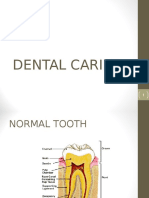
- Dental CariesDocument74 pagesDental CariesParidhi Garg67% (3)
- Prevention of Post ERCP Pancreatitis Where Are We NowDocument5 pagesPrevention of Post ERCP Pancreatitis Where Are We NowPaul HartingNo ratings yet
- Wound Care PefDocument3 pagesWound Care PefJenny Agustin FabrosNo ratings yet
- Week 6 PERSONAL DEVELOPMENT LAS G11Document3 pagesWeek 6 PERSONAL DEVELOPMENT LAS G11elainevidalrodriguezNo ratings yet
- Listeria MonocytogenesDocument30 pagesListeria Monocytogenestummalapalli venkateswara raoNo ratings yet
- For 10 KLDDocument4 pagesFor 10 KLDrahul100% (1)
- Dissertation Topics in Rajiv Gandhi University of Health SciencesDocument7 pagesDissertation Topics in Rajiv Gandhi University of Health SciencesWhereCanIFindSomeoneToWriteMyPaperNewarkNo ratings yet
- Hydro LettuceDocument4 pagesHydro LettuceGilberto Alexis Alcantara OrtizNo ratings yet
- Mom - 12.10.2021Document2 pagesMom - 12.10.2021SHOBHIT MAURYANo ratings yet
- Lesson1 Line DanceDocument13 pagesLesson1 Line DanceMaria VictoriaNo ratings yet
- Heat Wave Action Plan RMC 2017Document30 pagesHeat Wave Action Plan RMC 2017Saarthak BadaniNo ratings yet
- Maureen Chilila, Jhpiego-Zambia, IAS 2012 Poster, Couple CounselingDocument1 pageMaureen Chilila, Jhpiego-Zambia, IAS 2012 Poster, Couple CounselingJhpiegoNo ratings yet
- Recall The Functions of The Organs in The Gas Exchange SystemDocument14 pagesRecall The Functions of The Organs in The Gas Exchange SystemAhmad AhmadNo ratings yet
- The Program Proposal - DiabetesDocument11 pagesThe Program Proposal - DiabetesRifa'atul Mahmudah100% (2)
- FnolDocument2 pagesFnolamol.d.kelkarNo ratings yet
- HIS VidDocument8 pagesHIS VidJacqueline HarleNo ratings yet
- Factories Act - Final For PrintDocument21 pagesFactories Act - Final For PrintRamesh Kumar RNo ratings yet
- BMS Activity List PDFDocument2 pagesBMS Activity List PDFKeith FernándezNo ratings yet
- Florence Nightingale: The Fixed Determination of An Indomitable WillDocument14 pagesFlorence Nightingale: The Fixed Determination of An Indomitable WillDipesh MuthaNo ratings yet
- Curriculum Vitae Lettre de Motivation InfirmièreDocument5 pagesCurriculum Vitae Lettre de Motivation InfirmièreEkoume Serges-ArmelNo ratings yet
- Bronchial Asthma: Sudhakar Lakavath Dept - Of.PharmacologyDocument50 pagesBronchial Asthma: Sudhakar Lakavath Dept - Of.PharmacologySudhakar LakavathNo ratings yet
- Batch20 Group 6 Macro Economics Project ReportDocument28 pagesBatch20 Group 6 Macro Economics Project ReportHK1959No ratings yet
- Star Women Care - Premium Chart (Including Tax - Two Year)Document2 pagesStar Women Care - Premium Chart (Including Tax - Two Year)dharam singhNo ratings yet