Hormone Replacement Therapy (HRT) :: DR - Fatin
Hormone Replacement Therapy (HRT) :: DR - Fatin
Download as ppt, pdf, or txt
You might also like
- Very Advanced Maternal Age, TOG-2021Document10 pagesVery Advanced Maternal Age, TOG-2021saeed hasan saeedNo ratings yet
- 21 - Postoperative Complications and Managament IDocument30 pages21 - Postoperative Complications and Managament IAmmarNo ratings yet
- Male and Female Reproductive System TestDocument2 pagesMale and Female Reproductive System TestRoana Marie Tapia100% (5)
- Hormone Replacement TherapyDocument43 pagesHormone Replacement Therapymedmc303No ratings yet
- HRTDocument62 pagesHRTArpita ArpitaNo ratings yet
- Background of The Condition:: Those That Put A Person at Risk of Developing A Problem)Document3 pagesBackground of The Condition:: Those That Put A Person at Risk of Developing A Problem)Genelly Anne Argañoza RamosNo ratings yet
- Perimenopause: For Some Time, A Woman Will Continue To Menstruate, AlthoughDocument7 pagesPerimenopause: For Some Time, A Woman Will Continue To Menstruate, Althoughmsah820No ratings yet
- NIH Facts PMH Therapy ReviewDocument24 pagesNIH Facts PMH Therapy ReviewwaterprincessNo ratings yet
- Metabolic and Endocrine Pharmacology: Gonadol DrugsDocument38 pagesMetabolic and Endocrine Pharmacology: Gonadol Drugstheintrov100% (1)
- Menstrual Disorders 2Document39 pagesMenstrual Disorders 2Nanang Hidayatulloh100% (1)
- MenopuseDocument30 pagesMenopusemohamed mowafeyNo ratings yet
- Group 7 Drugs Acting on the Hormonal SystemDocument35 pagesGroup 7 Drugs Acting on the Hormonal Systemolajidepeace30No ratings yet
- Therapeutic Success in The Primary Amenorrhea Is Very Limited. Management Is Done According To CauseDocument66 pagesTherapeutic Success in The Primary Amenorrhea Is Very Limited. Management Is Done According To CauseNyshan KarkiNo ratings yet
- PcosDocument9 pagesPcosMonomay HalderNo ratings yet
- Pharmacological Agents of Respiratory System DisordersDocument5 pagesPharmacological Agents of Respiratory System Disorderslaiba.habib18No ratings yet
- Hormonal ContraceptivesDocument25 pagesHormonal Contraceptivesmd easarur rahmanNo ratings yet
- Pcod Natural TreatmentDocument4 pagesPcod Natural Treatmenttusharphale100% (1)
- The Gonadal Hormones & Inhibitors: by M.H.Farjoo M.D., PH.DDocument133 pagesThe Gonadal Hormones & Inhibitors: by M.H.Farjoo M.D., PH.DsajidNo ratings yet
- Oestradiol As Hemihydrate + DrospirenoneDocument15 pagesOestradiol As Hemihydrate + Drospirenoneddandan_2No ratings yet
- 3 - Nursing Management of Female Physiologic Processes-102969Document36 pages3 - Nursing Management of Female Physiologic Processes-102969Izziddin YassineNo ratings yet
- DR SR Agatha ShinyalaDocument60 pagesDR SR Agatha ShinyalaCLEMENTNo ratings yet
- Hormone Replacement TherapyDocument24 pagesHormone Replacement TherapyZai Akma100% (2)
- Nursing Management of MenopauseDocument37 pagesNursing Management of MenopauseSuby Beigh82% (11)
- Reproductive System DrugsDocument100 pagesReproductive System DrugsR-jay Guevara100% (1)
- Premenstrual Syndrome 2Document25 pagesPremenstrual Syndrome 2anojan100% (1)
- Sex HormonesDocument12 pagesSex Hormoneshadeelizedeen08No ratings yet
- Pharmadoor - Isoprinosine BulaDocument6 pagesPharmadoor - Isoprinosine Bularamon leyvaNo ratings yet
- Drugs Mechanism of Action Side Effect/Adverse Effect/Contraindication Nursing InterventionsDocument17 pagesDrugs Mechanism of Action Side Effect/Adverse Effect/Contraindication Nursing InterventionsJerome Vergel RubianesNo ratings yet
- Reproductive System DiseasesDocument42 pagesReproductive System DiseasesrnrmmanphdNo ratings yet
- 2019 Gonadal Hormones-3Document197 pages2019 Gonadal Hormones-3Vishwajeet RaneNo ratings yet
- Management of Menopause: OS Tang Department of Obstetrics and Gynaecology University of Hong KongDocument55 pagesManagement of Menopause: OS Tang Department of Obstetrics and Gynaecology University of Hong Kongbebekdd22No ratings yet
- Pharmacology of The Reproductive SystemDocument5 pagesPharmacology of The Reproductive SystemMark Russel Sean LealNo ratings yet
- 2015 Ovulation-InductionDocument11 pages2015 Ovulation-InductionMARIAPAULACASTILLO1No ratings yet
- Menstrual IrregularitiesDocument60 pagesMenstrual IrregularitiesAlice WankhedeNo ratings yet
- Amenorrhea Presented by Muhammad AbdullahDocument28 pagesAmenorrhea Presented by Muhammad Abdullahtooba hussainNo ratings yet
- MenopauseDocument52 pagesMenopauseGaoudam NatarajanNo ratings yet
- Menopause: Treatments For Menopausal SymptomsDocument9 pagesMenopause: Treatments For Menopausal SymptomsAmy LalringhluaniNo ratings yet
- Section For NotesDocument3 pagesSection For NotesKeNo ratings yet
- N.K Jain SOP 4Document5 pagesN.K Jain SOP 4Gautam ShrivastavaNo ratings yet
- Amenorrhea & Heavy Menstrual BleedingDocument22 pagesAmenorrhea & Heavy Menstrual BleedingJanesel Plariza PanerioNo ratings yet
- InfertilityDocument38 pagesInfertilityRaghad AmjadNo ratings yet
- Fact Sheet: Patient EducationDocument5 pagesFact Sheet: Patient Educationisaco1531012No ratings yet
- Gynecological NursingDocument329 pagesGynecological Nursingsharon ocharaNo ratings yet
- ABNORMAL UTERINE BLEEDING PPTDocument35 pagesABNORMAL UTERINE BLEEDING PPTvmconlibrary2022No ratings yet
- Womens HealthDocument12 pagesWomens HealthPooja ChoudharyNo ratings yet
- Seminar# 14 Management of Abnormal Gynecological Bleeding 2Document75 pagesSeminar# 14 Management of Abnormal Gynecological Bleeding 2Amir MajdiNo ratings yet
- Menstruation-Related DisordersDocument55 pagesMenstruation-Related Disordersaqeelamr557No ratings yet
- Dysfunctional Uterine BleedingDocument2 pagesDysfunctional Uterine BleedingBubblets Margaux GoldiNo ratings yet
- Estradiol Valerate 2mg + Nongestrel 0.5mg (PROGYLUTON)Document12 pagesEstradiol Valerate 2mg + Nongestrel 0.5mg (PROGYLUTON)ddandan_2No ratings yet
- Discharge PlanningDocument3 pagesDischarge Planningfjhjhkyu50% (2)
- An Update On Menopause ManagementDocument10 pagesAn Update On Menopause ManagementJuan FranciscoNo ratings yet
- DefaultDocument16 pagesDefaultRoFi PoXerNo ratings yet
- Diseases of The Male and FemaleDocument4 pagesDiseases of The Male and FemaleemilieNo ratings yet
- AmenorrheaDocument13 pagesAmenorrheaJanesel Plariza PanerioNo ratings yet
- Amenorrhea Burhan 49Document40 pagesAmenorrhea Burhan 49Burhan NabiNo ratings yet
- Pcos - Clinical Case DiscussionDocument4 pagesPcos - Clinical Case Discussionreham macadatoNo ratings yet
- AUB StartedDocument13 pagesAUB StartedIbrahim AbdullahNo ratings yet
- CONTRACEPTIONDocument38 pagesCONTRACEPTIONGopala HariNo ratings yet
- ClimacteriumDocument68 pagesClimacteriumkuhan KalaichelvanNo ratings yet
- Different Faces of PCOS (Polycystic Ovarian Syndrome) : Shahnaz AkbarDocument38 pagesDifferent Faces of PCOS (Polycystic Ovarian Syndrome) : Shahnaz AkbararyNo ratings yet
- Absent or Irregular PeriodsDocument6 pagesAbsent or Irregular PeriodsEcbNo ratings yet
- Estradiol 10mcg (Vagifen)Document13 pagesEstradiol 10mcg (Vagifen)asdwasdNo ratings yet
- Recurrent MiscarriageDocument9 pagesRecurrent MiscarriageAmmarNo ratings yet
- Intestinal DiseasesDocument20 pagesIntestinal DiseasesAmmarNo ratings yet
- Induced Abortion: Dr. Ali Murad Dr. Wassan NoriDocument12 pagesInduced Abortion: Dr. Ali Murad Dr. Wassan NoriAmmarNo ratings yet
- Endometrial Hyperplasia and Endometrial CancerDocument14 pagesEndometrial Hyperplasia and Endometrial CancerAmmarNo ratings yet
- Invasive Disease of VulvaDocument5 pagesInvasive Disease of VulvaAmmarNo ratings yet
- Contraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToDocument22 pagesContraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToAmmarNo ratings yet
- EndometrisisDocument10 pagesEndometrisisAmmarNo ratings yet
- 10 - Spinal Cord Injuries Lec.1Document7 pages10 - Spinal Cord Injuries Lec.1AmmarNo ratings yet
- 7 - HydrocephalusDocument4 pages7 - HydrocephalusAmmarNo ratings yet
- 5 - Space Occupying LesionsDocument39 pages5 - Space Occupying LesionsAmmarNo ratings yet
- 6 - Intracranial MassDocument5 pages6 - Intracranial MassAmmarNo ratings yet
- 4 - Raised ICPDocument6 pages4 - Raised ICPAmmarNo ratings yet
- 3 - Head Injured PatientDocument94 pages3 - Head Injured PatientAmmarNo ratings yet
- Medical History QuestionnaireDocument3 pagesMedical History QuestionnaireDre EzNo ratings yet
- Abortion Causes & Types: Presented by DeepakDocument41 pagesAbortion Causes & Types: Presented by DeepakMrs. DeepakNo ratings yet
- Newborn Baby Assessment NIPE OSCE GuideDocument23 pagesNewborn Baby Assessment NIPE OSCE GuideChen BrionesNo ratings yet
- Indravati PCPNDT 2 MoDocument6 pagesIndravati PCPNDT 2 MoDr Sachin Chitnis M O UPHC AiroliNo ratings yet
- Aakash Model Test Papers Solutions XII T1 BiologyDocument22 pagesAakash Model Test Papers Solutions XII T1 BiologyAbhinay KumarNo ratings yet
- Drugs Used in ObstetricsDocument37 pagesDrugs Used in ObstetricsWhirmey ChinyamaNo ratings yet
- Module 1 NCM109Document41 pagesModule 1 NCM109AmethystNo ratings yet
- Dylan CharlesDocument2 pagesDylan CharlesHafni KumarNo ratings yet
- Contraceptive Methods Bio ProjectDocument8 pagesContraceptive Methods Bio ProjectMr. CrustNo ratings yet
- Unit 3. (Group 16) Fertilization of Ovum, Embedding of The Blastocyst, Development and Growth of The FetusDocument80 pagesUnit 3. (Group 16) Fertilization of Ovum, Embedding of The Blastocyst, Development and Growth of The FetusKu NiniNo ratings yet
- Amanda Froisland - Registered Nurse BSN 2Document2 pagesAmanda Froisland - Registered Nurse BSN 2api-353034662No ratings yet
- Prelim Reviewer 2023Document83 pagesPrelim Reviewer 2023jakexsanchez1515No ratings yet
- DAMEDocument10 pagesDAMEFlavia SchaidhauerNo ratings yet
- La Consolacion University Philippines Catmon, City of Malolos, BulacanDocument8 pagesLa Consolacion University Philippines Catmon, City of Malolos, BulacanLowi MesiasNo ratings yet
- Lesson Plan Preparing For Parenthood Pregnancy and Labor - 0Document15 pagesLesson Plan Preparing For Parenthood Pregnancy and Labor - 0Sweta ManandharNo ratings yet
- Gynaecology - Riley HarrisonDocument45 pagesGynaecology - Riley HarrisonFiras AliNo ratings yet
- Chapter 4 EmbryogenesisDocument20 pagesChapter 4 EmbryogenesisAbd EloihedNo ratings yet
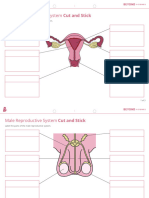
- Human Reproductive System Cut and StickDocument3 pagesHuman Reproductive System Cut and StickLachlan WRIGHTNo ratings yet
- Pediatric and Adolescent GynecologyDocument11 pagesPediatric and Adolescent GynecologyAndrea GuidoteNo ratings yet
- L7 7Bd4, Pregnancy WorksheetDocument1 pageL7 7Bd4, Pregnancy Worksheetxs5kqfmc7cNo ratings yet
- Preterm PROM: Prediction, Prevention, PrinciplesDocument6 pagesPreterm PROM: Prediction, Prevention, PrinciplesanggunNo ratings yet
- Obstetrics Gyn MCPS ProspectusDocument24 pagesObstetrics Gyn MCPS Prospectususman sajid100% (2)
- Uts-9 1-13 2Document27 pagesUts-9 1-13 2shandierika.pitaoNo ratings yet
- The Fifth HouseDocument3 pagesThe Fifth HouseAshish Kumar AgnihotriNo ratings yet
- LeopoldsDocument2 pagesLeopoldsMhianne SarmientoNo ratings yet
- How To Pass Kuwait Interview As A Nurse, What Questions Can Be Asked in Kuwait InterviewDocument4 pagesHow To Pass Kuwait Interview As A Nurse, What Questions Can Be Asked in Kuwait InterviewpamelajemberNo ratings yet
- NCP - PreeclampsiaDocument3 pagesNCP - PreeclampsiaRap De la Cruz50% (2)
- Absalan 2012Document4 pagesAbsalan 2012Tiffany LamNo ratings yet