Chest Tubes
Chest Tubes
Download as ppt, pdf, or txt
You might also like
- Iso Auto-Service 4R2SDocument2 pagesIso Auto-Service 4R2SMuhd ShafiqNo ratings yet
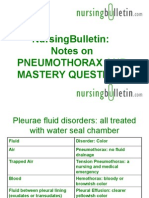
- Chest Tubes and Drainage Systems: Deb Updegraff RN, CNS Picu LPCHDocument28 pagesChest Tubes and Drainage Systems: Deb Updegraff RN, CNS Picu LPCHLucila LugoNo ratings yet
- Chest TubesDocument28 pagesChest Tubeswarda farooqNo ratings yet
- ChesttubedrainageDocument65 pagesChesttubedrainagejerinthomasrajanNo ratings yet
- Tube ThoracostomyDocument17 pagesTube ThoracostomyheiyuNo ratings yet
- Chest DrainageDocument22 pagesChest DrainageAmeliaM100% (7)
- Assisting With Chest Tube InsertionDocument5 pagesAssisting With Chest Tube InsertionLoveSheryNo ratings yet
- Chest Tube and Water-Seal DrainageDocument25 pagesChest Tube and Water-Seal DrainageGhadaNo ratings yet
- Skills LabDocument3 pagesSkills Labmilcah_castilloNo ratings yet
- Chest Tube ThoracostomyDocument7 pagesChest Tube Thoracostomyfufoo_tracylirioNo ratings yet
- Chest Tube ThoracostomyDocument7 pagesChest Tube Thoracostomyskyblueali100% (2)
- Pleural TappingDocument15 pagesPleural TappingAnusha Verghese100% (1)
- Chest Tube Care Management TroubleshootingDocument5 pagesChest Tube Care Management TroubleshootingRaina Ginella DsouzaNo ratings yet
- Chest Tubes and ThoracentesisDocument18 pagesChest Tubes and ThoracentesisecleptosNo ratings yet
- Management of Chest TubeDocument22 pagesManagement of Chest TubeFatima Hafza Sahiddin100% (1)
- Chest TubeDocument3 pagesChest TubeJohn Michael SalinasNo ratings yet
- Chest Tube ThoracostomyDocument4 pagesChest Tube ThoracostomyKodok IjooNo ratings yet
- ThoracostomyDocument2 pagesThoracostomyJanelle MarceraNo ratings yet
- What Is A Tracheostomy? Why Is A Tracheostomy Performed?Document5 pagesWhat Is A Tracheostomy? Why Is A Tracheostomy Performed?Mara JnelleNo ratings yet
- Laxmi MamDocument7 pagesLaxmi MamkamalshrishNo ratings yet
- Management of Chest TubeDocument22 pagesManagement of Chest Tubernrmmanphd100% (1)
- Chest Tubes OUPUTDocument3 pagesChest Tubes OUPUTparislove19No ratings yet
- Chest Tubes and ThoracentesisDocument18 pagesChest Tubes and ThoracentesisecleptosNo ratings yet
- Ateneo de Naga University: College of NursingDocument3 pagesAteneo de Naga University: College of NursingRenie SerranoNo ratings yet
- LM 3 - Chest TubeDocument5 pagesLM 3 - Chest TubeMelrhean GraceNo ratings yet
- Pleural Anatomy 1st Year Clinical by DR MuzaffarDocument22 pagesPleural Anatomy 1st Year Clinical by DR MuzaffarKashar SaeedNo ratings yet
- NursingBulletin Notes On PneumothoraxDocument27 pagesNursingBulletin Notes On Pneumothoraxseigelystic100% (11)
- CTTDocument47 pagesCTTleizelgalvezNo ratings yet
- Respiratory System: Gemalyn BulawanDocument122 pagesRespiratory System: Gemalyn BulawanSofia Deneise Anasarias100% (1)
- Oxygenation 3.0Document14 pagesOxygenation 3.0Jake Yvan DizonNo ratings yet
- Surgical Tubes: Hadi MunibDocument57 pagesSurgical Tubes: Hadi MunibAli ahmedNo ratings yet
- CTT CareDocument76 pagesCTT CareMarites Santos AquinoNo ratings yet
- Assisting in Thoracostomy Tube InsertionDocument54 pagesAssisting in Thoracostomy Tube Insertioncoosa liquorsNo ratings yet
- Prosedur WSD (Water Seal Drainage)Document44 pagesProsedur WSD (Water Seal Drainage)White GooseNo ratings yet
- Types of Chest Drainage SystemDocument3 pagesTypes of Chest Drainage SystembernardsoNo ratings yet
- Chest Tube Insertion: An Intercostal CatheterDocument2 pagesChest Tube Insertion: An Intercostal CatheterssNo ratings yet
- TRACHEOSTOMYDocument2 pagesTRACHEOSTOMY3C SAVELLA, Glaiza Marie RNo ratings yet
- Abdominal ParacentesisDocument4 pagesAbdominal ParacentesisRashmi C S100% (1)
- Chest TubeDocument8 pagesChest TubetanabalrajNo ratings yet
- Chest Tube DrainageDocument7 pagesChest Tube Drainagekim reyes100% (1)
- Chest Tubes and Water Seal Drainage: P. NandiDocument8 pagesChest Tubes and Water Seal Drainage: P. Nandikim_sayamNo ratings yet
- Chest TubeDocument18 pagesChest TubeAyu MasturaNo ratings yet
- IR LCTR 10 Part 2Document33 pagesIR LCTR 10 Part 2seemabfarwauaeNo ratings yet
- Chest Tube Insertion and MonitoringDocument4 pagesChest Tube Insertion and MonitoringCamille Cirineo Arensol100% (2)
- Chapter 27: Lower Respiratory Problems Pleural Effusion With Thoracentesis and Chest TubeDocument3 pagesChapter 27: Lower Respiratory Problems Pleural Effusion With Thoracentesis and Chest TubeSherree HayesNo ratings yet
- Chest Tube DrainageDocument45 pagesChest Tube DrainageDonald BidenNo ratings yet
- Chest DrainagesDocument64 pagesChest DrainagesgeoellaabcabNo ratings yet
- 1-3 Way Bottle System and SuctioningDocument9 pages1-3 Way Bottle System and SuctioningJz Andamun100% (2)
- Tracheostomy: ENT Department DMC & Hospital Ludhiana PunjabDocument46 pagesTracheostomy: ENT Department DMC & Hospital Ludhiana PunjabVikrant MittalNo ratings yet
- WSDDocument59 pagesWSDdiandrasafirinaNo ratings yet
- Chest TubesDocument2 pagesChest TubesLeahandJosh NadhernyNo ratings yet
- Nursing Practices: Troubleshooting Thoracostomy Tube ManagementDocument6 pagesNursing Practices: Troubleshooting Thoracostomy Tube ManagementDeo RizkyandriNo ratings yet
- TracheostomyDocument4 pagesTracheostomyNapieh Bulalaque PolisticoNo ratings yet
- Oncology - Presentation EditedDocument71 pagesOncology - Presentation EditedSarah Racheal AkelloNo ratings yet
- Care of Patient On I C DDocument15 pagesCare of Patient On I C DGeorge John Jeelu SusanNo ratings yet
- Craven & Hirnle's Nursing Procedures and Fundamentals OnlineDocument4 pagesCraven & Hirnle's Nursing Procedures and Fundamentals Onlineisapatrick8126No ratings yet
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- AP Corporate ProfileDocument28 pagesAP Corporate ProfileMuhd ShafiqNo ratings yet
- Bloodborne April 08Document32 pagesBloodborne April 08Muhd ShafiqNo ratings yet
- Employee Training LogDocument3 pagesEmployee Training LogMuhd ShafiqNo ratings yet
- Borang Audit DalamanDocument5 pagesBorang Audit DalamanMuhd ShafiqNo ratings yet
- IC 2023 Calendar of Events 9053Document5 pagesIC 2023 Calendar of Events 9053Muhd ShafiqNo ratings yet
- Template Turtle DiagramDocument1 pageTemplate Turtle DiagramMuhd ShafiqNo ratings yet
- IC Transition Plan Template 8544 V1Document4 pagesIC Transition Plan Template 8544 V1Muhd ShafiqNo ratings yet
- Excel ChandranDocument2 pagesExcel ChandranMuhd ShafiqNo ratings yet
- Robotic Scrubber Downtime RecordDocument1 pageRobotic Scrubber Downtime RecordMuhd ShafiqNo ratings yet
- Annex 2f COVID19Document1 pageAnnex 2f COVID19Muhd ShafiqNo ratings yet
- Quality Management Summary Report Test 1Document4 pagesQuality Management Summary Report Test 1Muhd ShafiqNo ratings yet
- File LABEL INTERNAL AUDITDocument1 pageFile LABEL INTERNAL AUDITMuhd ShafiqNo ratings yet
- Sample Material Required QO RehabDocument2 pagesSample Material Required QO RehabMuhd ShafiqNo ratings yet
- 02 Internal Audit ChecklistDocument2 pages02 Internal Audit ChecklistMuhd ShafiqNo ratings yet
- 7 Step Isolation Cleaning ProcessDocument5 pages7 Step Isolation Cleaning ProcessMuhd ShafiqNo ratings yet
- ATP2022Document60 pagesATP2022Muhd ShafiqNo ratings yet
- ASTMA NisreenDocument19 pagesASTMA NisreenMuhd ShafiqNo ratings yet
- Gantt Chart: Learn About Gantt ChartsDocument4 pagesGantt Chart: Learn About Gantt ChartsMuhd ShafiqNo ratings yet
- The Respiratory System of OxDocument14 pagesThe Respiratory System of OxHemant JoshiNo ratings yet
- Hemoroid NewDocument33 pagesHemoroid NewaldisNo ratings yet
- Astro Diagnosis VirgoDocument42 pagesAstro Diagnosis VirgoOvn Murthy100% (1)
- Reformer Mat3Document66 pagesReformer Mat3Suat Barut100% (5)
- Pelvic TraumaDocument47 pagesPelvic TraumaMuhammad DaniyalNo ratings yet
- Nir Hus Absite Review Q9Document9 pagesNir Hus Absite Review Q9nir4846No ratings yet
- Wandering Spleen, Gastric and Pancreatic Volvulus and Right-Sided Descending and Sigmoid ColonDocument8 pagesWandering Spleen, Gastric and Pancreatic Volvulus and Right-Sided Descending and Sigmoid ColonChristabella Natalia WijayaNo ratings yet
- Planes and Diameters of The PelvisDocument32 pagesPlanes and Diameters of The PelvisRumelle ReyesNo ratings yet
- 234b1e3ba7994c728793b8e1725bd0e1Document12 pages234b1e3ba7994c728793b8e1725bd0e1Максим КариNo ratings yet
- Pelvic Trauma: DR Indro Wibowo SejatiDocument42 pagesPelvic Trauma: DR Indro Wibowo SejatiIndro Wibowo100% (1)
- PostureDocument2 pagesPostureNader Morris100% (1)
- Topographic Anatomy of The Pelvis PDFDocument23 pagesTopographic Anatomy of The Pelvis PDFEl SpinnerNo ratings yet
- Pelvic OMM GuideDocument3 pagesPelvic OMM GuideSameer AkhtarNo ratings yet
- Surgery II Schedule 2020-21 PDFDocument2 pagesSurgery II Schedule 2020-21 PDFArianneJulienaCervaniaAndradaNo ratings yet
- Anatomy ProstateDocument2 pagesAnatomy ProstatenavjavNo ratings yet
- Topographic Anatomy of Abdominal OrgansDocument18 pagesTopographic Anatomy of Abdominal OrgansHasnain IdreesNo ratings yet
- Abd AortaDocument48 pagesAbd AortaSanjib NepramNo ratings yet
- Anatomy - Vertebral ColumnDocument5 pagesAnatomy - Vertebral ColumnArmelda Elda MuhollariNo ratings yet
- Inguinal Region 1617Document23 pagesInguinal Region 1617Gx NavinNo ratings yet
- Anterior Abdominal WallDocument108 pagesAnterior Abdominal WallMunikrishna Salavakam100% (1)
- Regional Techniques For Cardiac and Cardiac-Related ProceduresDocument15 pagesRegional Techniques For Cardiac and Cardiac-Related Procedures凌晓敏No ratings yet
- Estudio Osteopor Osteoporisis GloriaDocument5 pagesEstudio Osteopor Osteoporisis Gloriadiana corralNo ratings yet
- Body Condition Score Chart Dogs - 0Document1 pageBody Condition Score Chart Dogs - 0dacaNo ratings yet
- Pelvic TiltDocument15 pagesPelvic TiltFarrukh Shahzad83% (6)
- Anatomy For Beginners 3 - DigestionDocument20 pagesAnatomy For Beginners 3 - DigestionDefy R PradentyNo ratings yet
- EXPLORING THE HUMAN HEART Key To CorrectionDocument3 pagesEXPLORING THE HUMAN HEART Key To CorrectionAsh KetchumNo ratings yet
- Lesson 1 - The Human BodyDocument8 pagesLesson 1 - The Human BodyGilmar ManzanoNo ratings yet
- Adrenal 1 5Document41 pagesAdrenal 1 5Ditas ChuNo ratings yet
- Thoracic Duct - Wikipedia PDFDocument22 pagesThoracic Duct - Wikipedia PDFPratibha AgarwalNo ratings yet
- Displaying All Codes For DRG 552Document3 pagesDisplaying All Codes For DRG 552drtimadamsNo ratings yet