Cerebral Palsy (CP) : DR Raj Kumar Yadav Assist. Prof., PMR MBBS VI Sem. - 25/04/2019
Cerebral Palsy (CP) : DR Raj Kumar Yadav Assist. Prof., PMR MBBS VI Sem. - 25/04/2019
Download as pptx, pdf, or txt
You might also like
- Mark Klimek Full Nclex ReviewerDocument30 pagesMark Klimek Full Nclex ReviewerAlex Bell100% (2)
- NRNP 6675 Final Exam Questions and Answers Latest 2024Document26 pagesNRNP 6675 Final Exam Questions and Answers Latest 2024kinyuaboris990No ratings yet
- Medback - Cerebral PalsyDocument47 pagesMedback - Cerebral Palsyyreshgem100% (2)
- Cerebral PalsyDocument97 pagesCerebral PalsyPrernaSharma100% (4)
- Major Depressive Disorder: Presented By: Justin Darrell A. SALACUPDocument15 pagesMajor Depressive Disorder: Presented By: Justin Darrell A. SALACUPJoana Mikee Rasay100% (1)
- Cerebral PalsyDocument38 pagesCerebral PalsyRahul KambleNo ratings yet
- CP 1Document38 pagesCP 1Sabah shahatNo ratings yet
- Cerebral PalsyDocument33 pagesCerebral PalsySaran GodcilNo ratings yet
- Cerebral PalsyDocument96 pagesCerebral PalsyRahini PaniNo ratings yet
- Cerebral Palsy BrieflyDocument50 pagesCerebral Palsy BrieflymeenoNo ratings yet
- CPDocument86 pagesCPMahnoorNo ratings yet
- Cerebral PalsyDocument35 pagesCerebral PalsyEnuga ApplegateNo ratings yet
- Cerebral Palsy New MateryDocument95 pagesCerebral Palsy New MateryAgus WibowoNo ratings yet
- 6 - Cerebral PalsyDocument52 pages6 - Cerebral PalsySaleha TariqNo ratings yet
- CP UpdatedDocument45 pagesCP UpdatedSivakumar Kathuu KarthikeyanNo ratings yet
- Presented By: Rose Ann M.Garcia BSN-2CDocument44 pagesPresented By: Rose Ann M.Garcia BSN-2Cmichael so100% (3)
- Spinal Muscle AtrophyDocument33 pagesSpinal Muscle AtrophyAaliyah ShaikhNo ratings yet
- Cerebral Palsy - EstDocument45 pagesCerebral Palsy - EstAisyah NabilaNo ratings yet
- DR D Kalpana, M.D, D.M (Neuro) Assoc. Professor of Pediatric Neurology, Medical College, TrivandrumDocument54 pagesDR D Kalpana, M.D, D.M (Neuro) Assoc. Professor of Pediatric Neurology, Medical College, TrivandrumjspradeepscribdNo ratings yet
- Cerebral Palsy (CP) : Neurology Chapter of IAPDocument42 pagesCerebral Palsy (CP) : Neurology Chapter of IAPIslam Mohsen0% (1)
- Cerebral Palsy (CP) : Neurology Chapter of IAPDocument42 pagesCerebral Palsy (CP) : Neurology Chapter of IAPWegrimel AriegaraNo ratings yet
- Cerebral PalsyDocument28 pagesCerebral Palsyghofran001997No ratings yet
- Cerebral Palsy by DR - Jaya ShankerDocument38 pagesCerebral Palsy by DR - Jaya ShankerJaya Shankar TedlaNo ratings yet
- Cerebral PalsyDocument60 pagesCerebral PalsychandniNo ratings yet
- Cerebral PalsyDocument11 pagesCerebral PalsySanthosh.S.UNo ratings yet
- Discuss Surgical Management of Cerebral Palsy - 000Document72 pagesDiscuss Surgical Management of Cerebral Palsy - 000SamNo ratings yet
- Kelainan Saraf KongenitalDocument35 pagesKelainan Saraf KongenitalTitisNo ratings yet
- Cerebral-Palsy 2Document36 pagesCerebral-Palsy 2Phoebe TuyogonNo ratings yet
- CP Sujit ModifiedDocument34 pagesCP Sujit ModifiedSujit KoiralaNo ratings yet
- CP MedbackDocument30 pagesCP MedbackJoanna EdenNo ratings yet
- Cerebral Palsy Lecture1 ٠٥١٤٥٠Document56 pagesCerebral Palsy Lecture1 ٠٥١٤٥٠nagmxxmNo ratings yet
- Care of A Child With Neuro Muscular DisordersDocument25 pagesCare of A Child With Neuro Muscular DisordersBilly RayNo ratings yet
- Cerebral PalsyDocument27 pagesCerebral PalsyAman SamNo ratings yet
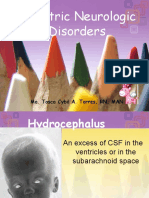
- Pediatric Neurologic Disorders: Ma. Tosca Cybil A. Torres, RN, MANDocument97 pagesPediatric Neurologic Disorders: Ma. Tosca Cybil A. Torres, RN, MANMa Tosca Cybil TorresNo ratings yet
- Approach To Floppy Infant: LT Col (DR) Bindu T Nair Professor (Pediatrics)Document56 pagesApproach To Floppy Infant: LT Col (DR) Bindu T Nair Professor (Pediatrics)Dorjee SengeNo ratings yet
- Cerebrals PalsyDocument21 pagesCerebrals PalsycaliaabelorNo ratings yet
- Rehabilitation of Cerebral Palsy & Motor DelayDocument49 pagesRehabilitation of Cerebral Palsy & Motor DelayasloocltNo ratings yet
- Compre ReviewDocument11 pagesCompre ReviewLyka Monique Barien SerranoNo ratings yet
- CPDocument13 pagesCPRiphu RashydNo ratings yet
- On Cerebral PalsyDocument18 pagesOn Cerebral Palsyanimol abrahamNo ratings yet
- 4. Cerebral PalsyDocument27 pages4. Cerebral PalsyA AZIZNo ratings yet
- Cerebral Palsy: PediatricsDocument50 pagesCerebral Palsy: PediatricsRANJIT GOGOINo ratings yet
- NCM 109-Cerebral PalsyDocument36 pagesNCM 109-Cerebral PalsyLeigh Ann Prosyne Lozada100% (1)
- Cerebral PalsyDocument4 pagesCerebral Palsyfire_n_iceNo ratings yet
- Slide Gross MotorDocument16 pagesSlide Gross MotorNur Impiana100% (1)
- Cerebral Palsy HandoutDocument2 pagesCerebral Palsy HandoutcaliaabelorNo ratings yet
- Cerebral Palsy: Submitted By: Prerna Sharma M.SC Nursing, 4 SemesterDocument97 pagesCerebral Palsy: Submitted By: Prerna Sharma M.SC Nursing, 4 Semestervarshasharma05100% (2)
- Neema Rawat Microteaching (Spina Bifida)Document67 pagesNeema Rawat Microteaching (Spina Bifida)Dimple GoyalNo ratings yet
- Neuro DisordersDocument159 pagesNeuro DisordersQuolette Constante100% (1)
- Spina BifidaDocument23 pagesSpina BifidaNihal EmadNo ratings yet
- Cerebral PalsyDocument20 pagesCerebral PalsyاسيرالاحزانNo ratings yet
- 15.spina BifidaDocument37 pages15.spina BifidaAbdullah AzamNo ratings yet
- Cerebral Palsy: An OverviewDocument9 pagesCerebral Palsy: An OverviewShanya VishnoiNo ratings yet
- Text FinalDocument6 pagesText FinalSahil KaushikNo ratings yet
- Cerebral PalsyDocument54 pagesCerebral PalsyMalathi KrishnanNo ratings yet
- CNS 2Document9 pagesCNS 2husainozelNo ratings yet
- Human GaitDocument58 pagesHuman GaitKota AnuroopNo ratings yet
- Cerebral PalsyDocument6 pagesCerebral Palsymogza3386No ratings yet
- 16 (A) - Cerebral PalsyDocument54 pages16 (A) - Cerebral PalsyAbdullah AzamNo ratings yet
- Cerebral Palsy (CP)Document23 pagesCerebral Palsy (CP)Piyu ShindeNo ratings yet
- UNIT I Cerebral PalsyDocument31 pagesUNIT I Cerebral PalsyTharangini GudlapuriNo ratings yet
- Pediatrics DR SandeepDocument8 pagesPediatrics DR SandeepAkshara SrriNo ratings yet
- Case StudyDocument13 pagesCase Studyapi-662629390No ratings yet
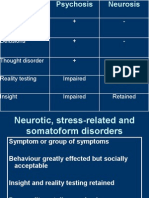
- Neurotic, Stress-Related and Somatoform DisDocument17 pagesNeurotic, Stress-Related and Somatoform Disapi-3703352No ratings yet
- Worksheet CCJMDocument2 pagesWorksheet CCJMapi-631170779No ratings yet
- Autism Center - Suppport BillDocument2 pagesAutism Center - Suppport BillJamaica MagallanesNo ratings yet
- Febrile SeizureDocument39 pagesFebrile SeizureTejinder SinghNo ratings yet
- Depression DepressionDocument14 pagesDepression DepressionYana IñigoNo ratings yet
- Module-10-Lecture-1-Cannabis, Mental Health, and Brain DisordersDocument13 pagesModule-10-Lecture-1-Cannabis, Mental Health, and Brain DisordersAbdul Aziz Success CoachNo ratings yet
- 17759-Article Text-51855-1-10-20220529Document12 pages17759-Article Text-51855-1-10-20220529Istu KuntoroNo ratings yet
- Case StudyDocument5 pagesCase Studywaqar.baig2025No ratings yet
- CVA SsDocument39 pagesCVA SsAnushri ManeNo ratings yet
- Jadwal Atls Online 7 Agustus 2021, JKTDocument4 pagesJadwal Atls Online 7 Agustus 2021, JKTDanar PratamaNo ratings yet
- Wisner 2019Document1 pageWisner 2019Miguel Ángel Cerón LealNo ratings yet
- Ischemic StrokeDocument17 pagesIschemic StrokejamalNo ratings yet
- The Bipolar Spectrum-The Shaping of A New Paradigm in Psychiatry Hagop AkiskalDocument3 pagesThe Bipolar Spectrum-The Shaping of A New Paradigm in Psychiatry Hagop AkiskalLaura Berenice Romero GonzálezNo ratings yet
- RH Incompatibility and PregnancyDocument2 pagesRH Incompatibility and PregnancyChelcee MagsinoNo ratings yet
- KiaraDocument7 pagesKiaraYethie Hillda PranataNo ratings yet
- Chicago Feeding Group 2022 Picky Vs PFD Vs ARFID Differential Diagnosis HANDOUTS File FOR PRINTING 1 01-220308-195443Document61 pagesChicago Feeding Group 2022 Picky Vs PFD Vs ARFID Differential Diagnosis HANDOUTS File FOR PRINTING 1 01-220308-195443Karen FioriNo ratings yet
- An Etiologic Classification of Autism Spectrum Disorders: Lidia V. Gabis MD and John Pomeroy MDDocument4 pagesAn Etiologic Classification of Autism Spectrum Disorders: Lidia V. Gabis MD and John Pomeroy MDCarlos Charlotte SalvadorNo ratings yet
- Agora Vs Social Phobia (Neurosis)Document8 pagesAgora Vs Social Phobia (Neurosis)Nur Liyana MazliNo ratings yet
- DSM V Clinical Cases - Chapter 15 Disruptive, Impulse-Control and Conduct DisordersDocument7 pagesDSM V Clinical Cases - Chapter 15 Disruptive, Impulse-Control and Conduct DisordersIzzyinOzzieNo ratings yet
- Daftar Pustaka: Diagnosis. British Journal of Hospital Medicine, June 2008, Vol 69, No 6Document2 pagesDaftar Pustaka: Diagnosis. British Journal of Hospital Medicine, June 2008, Vol 69, No 6Mohamad NasrullohNo ratings yet
- Retraction Ring LeafletDocument2 pagesRetraction Ring LeafletAna100% (1)
- Breaking Bad NewsDocument26 pagesBreaking Bad News8625g8xmbpNo ratings yet
- SpleenDocument36 pagesSpleenHoe TeohNo ratings yet
- Kegawatdaruratan Di Bidang Bedah Umum (Acute Abdomen)Document40 pagesKegawatdaruratan Di Bidang Bedah Umum (Acute Abdomen)Bimo MuktiNo ratings yet
- Urine Color ChartDocument1 pageUrine Color Chartsurajsongara199No ratings yet
- Euro J of Neurology - 2023 - Abou Mrad - Central Vein Sign and Paramagnetic Rim Sign From Radiologically Isolated SyndromeDocument7 pagesEuro J of Neurology - 2023 - Abou Mrad - Central Vein Sign and Paramagnetic Rim Sign From Radiologically Isolated SyndromeRenju KuriakoseNo ratings yet