HDP 301: Lecture #2: Immune Pathology Pain
HDP 301: Lecture #2: Immune Pathology Pain
Download as ppt, pdf, or txt
You might also like
- Infectious Disorders HandoutsDocument35 pagesInfectious Disorders Handoutsfebie pachecoNo ratings yet
- لقطة شاشة ٢٠٢٣-١١-٠٩ في ٨.٥٣.٥٠ صDocument7 pagesلقطة شاشة ٢٠٢٣-١١-٠٩ في ٨.٥٣.٥٠ صmo44hh44No ratings yet
- Chetna NewDocument8 pagesChetna NewRAVINDER YADAVNo ratings yet
- Inflammation: Course Teacher: Imon RahmanDocument21 pagesInflammation: Course Teacher: Imon RahmanDaksh SabharwalNo ratings yet
- Acut INFLAMMATION - banaldrobie banaldrobieDocument11 pagesAcut INFLAMMATION - banaldrobie banaldrobieammarNo ratings yet
- Acute InflammationDocument10 pagesAcute InflammationLydia Angel HartonoNo ratings yet
- InflammationDocument40 pagesInflammationSangameswaran B.BNo ratings yet
- Inflammation and Inflammatory MediatorsDocument28 pagesInflammation and Inflammatory Mediatorsla.instagramawaNo ratings yet
- Inflammation 30.08.2022Document39 pagesInflammation 30.08.2022Abdur RaquibNo ratings yet
- Pathology (Inflammation and Wound Healing)Document14 pagesPathology (Inflammation and Wound Healing)andrew100% (1)
- Inflammation and Tissue Repair: July 2021Document54 pagesInflammation and Tissue Repair: July 2021EdenNo ratings yet
- IVMS - General Pathology, Inflammation NotesDocument19 pagesIVMS - General Pathology, Inflammation NotesMarc Imhotep Cray, M.D.100% (1)
- 6.hypersensitivity Reactions 2Document32 pages6.hypersensitivity Reactions 2عوض الكريمNo ratings yet
- Immunity PosterDocument6 pagesImmunity PosterAirJeans GamingNo ratings yet
- Inflammation CompleteDocument56 pagesInflammation CompletePunjabi Culture KhushabNo ratings yet
- 4.-acute-inflammationDocument68 pages4.-acute-inflammationjoshuafadama62No ratings yet
- Inflammatory ResponseDocument4 pagesInflammatory ResponsealoisinelsonNo ratings yet
- Protection and Hypersensitivity Mechanism Which Manifest On SkinDocument99 pagesProtection and Hypersensitivity Mechanism Which Manifest On SkinBhayuBarunaNo ratings yet
- Pathophysiology _ InflammationDocument10 pagesPathophysiology _ InflammationIngrid Caroline MunizNo ratings yet
- 2 - Hypersensitvity ReactionsDocument55 pages2 - Hypersensitvity ReactionsSafa TaweelNo ratings yet
- Week 2 - Hour 1 - Inflammation and Wound HealingDocument37 pagesWeek 2 - Hour 1 - Inflammation and Wound HealingniranjiNo ratings yet
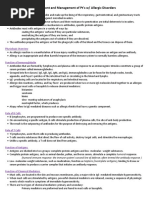
- Assessment and Management of Pt's W/ Allergic Disorders: Physiologic OverviewDocument11 pagesAssessment and Management of Pt's W/ Allergic Disorders: Physiologic OverviewChristina RichardsNo ratings yet
- Session 2Document65 pagesSession 2kasper mkNo ratings yet
- Source:Immunology Eight Edition David MaleDocument3 pagesSource:Immunology Eight Edition David MaleAzzahra FadhlilaNo ratings yet
- Hypersensitivity Reactions Type 3 and Type 4, Pathogenesis of AutoimmunityDocument20 pagesHypersensitivity Reactions Type 3 and Type 4, Pathogenesis of AutoimmunitySalomeSibashviliNo ratings yet
- INFLAMMATION للدراسة الاولية 2023 2024 exportDocument5 pagesINFLAMMATION للدراسة الاولية 2023 2024 exporthaidernajivpn2001No ratings yet
- Acute and Chronic Inflammation: Fatima Obeidat, MDDocument108 pagesAcute and Chronic Inflammation: Fatima Obeidat, MDraanja2100% (1)
- PUBHEALTHDocument18 pagesPUBHEALTHChi Keung Langit ChanNo ratings yet
- Acute Inflammation (1)Document55 pagesAcute Inflammation (1)Chilupula T PetronellaNo ratings yet
- InflammationDocument8 pagesInflammationGhazi Uddin AhmedNo ratings yet
- Workshop 1.2 Inflammation1Document30 pagesWorkshop 1.2 Inflammation1nganleo5801No ratings yet
- Inflammation and RepairDocument34 pagesInflammation and Repairanshum guptaNo ratings yet
- HypersensitivityDocument49 pagesHypersensitivityAkanksha Mahajan100% (1)
- InflammationDocument34 pagesInflammationمصطفى أحمدNo ratings yet
- Inflammation and Healing ReportDocument48 pagesInflammation and Healing Reportks75q5w94yNo ratings yet
- Mechanisms of Inflammation I, II, and III LOsDocument9 pagesMechanisms of Inflammation I, II, and III LOsAndrew SagalovNo ratings yet
- 700 - Wk. 2 - Inflammation, Infection & HIV LODocument10 pages700 - Wk. 2 - Inflammation, Infection & HIV LOAfNo ratings yet
- 3.acute InflammationDocument38 pages3.acute Inflammationyaqeenallawi23No ratings yet
- Drugs Acting On The Immune System: Retchel-Elly D. Dapli-AnDocument60 pagesDrugs Acting On The Immune System: Retchel-Elly D. Dapli-AnJoshua MendozaNo ratings yet
- GP LEC 3Document28 pagesGP LEC 3hetler343No ratings yet
- Immune FinalDocument53 pagesImmune FinalJaylord VerazonNo ratings yet
- Innate ImmunityDocument32 pagesInnate ImmunityYik sNo ratings yet
- Pathophysiology (Chapter 3 & 4)Document50 pagesPathophysiology (Chapter 3 & 4)tedasetesama8No ratings yet
- Inflammation and RepairDocument2 pagesInflammation and RepairSha BtstaNo ratings yet
- PHAR 233-InflammationDocument67 pagesPHAR 233-InflammationLina RamojNo ratings yet
- Allergy and HypersensitivityDocument49 pagesAllergy and HypersensitivityMoshe Cohen'sNo ratings yet
- 2nd Book-Physical Therapy, 2022Document88 pages2nd Book-Physical Therapy, 2022Ahmed Mahmoud MohamedNo ratings yet
- GenPath Mod3 InflammationDocument56 pagesGenPath Mod3 InflammationDanielle HayagNo ratings yet
- Disorders of Immunity Hypersensitivity Reactions: Dr. Mehzabin AhmedDocument25 pagesDisorders of Immunity Hypersensitivity Reactions: Dr. Mehzabin AhmedFrances FranciscoNo ratings yet
- Study-Notes - Inflammation-And-Repair (1) 88Document17 pagesStudy-Notes - Inflammation-And-Repair (1) 88jjjkkNo ratings yet
- Immunity 2Document4 pagesImmunity 2Mkhize KhabazelaNo ratings yet
- Inflammation and RepairDocument77 pagesInflammation and RepaironyekaNo ratings yet
- InflammationDocument8 pagesInflammationHarjot RandhawaNo ratings yet
- INFLAMMATIONDocument9 pagesINFLAMMATIONalkasimamina002No ratings yet
- Hypersensitivity ReactionsDocument25 pagesHypersensitivity Reactionsbpt2100% (4)
- HypersensitivityDocument30 pagesHypersensitivityShweta Mittal100% (1)
- Overview of InflammationDocument6 pagesOverview of InflammationArmand LiberatoNo ratings yet
- Inflammation 3Document44 pagesInflammation 3mikiyaskayleNo ratings yet
- Immunology Unveiled: A Comprehensive Journey through the Human Immune System: Guardians of the Body: The Unseen Heroes of ImmunityFrom EverandImmunology Unveiled: A Comprehensive Journey through the Human Immune System: Guardians of the Body: The Unseen Heroes of ImmunityNo ratings yet
- Hdp301vascularpathologies 2021Document2 pagesHdp301vascularpathologies 2021Linda NguyenNo ratings yet
- Wound Care and Sterile TechniqueDocument27 pagesWound Care and Sterile TechniqueLinda NguyenNo ratings yet
- Respiratory Failure, Hypoxia and HypercapneaDocument4 pagesRespiratory Failure, Hypoxia and HypercapneaLinda NguyenNo ratings yet
- UntitledDocument2 pagesUntitledLinda NguyenNo ratings yet
- UntitledDocument3 pagesUntitledLinda NguyenNo ratings yet
- Skills Checklist: Inserting A Large Bore Naso-Enteric (Referred To As Nasogastric Tube) or Orogastric Tube For Gastric SuctioningDocument2 pagesSkills Checklist: Inserting A Large Bore Naso-Enteric (Referred To As Nasogastric Tube) or Orogastric Tube For Gastric SuctioningLinda NguyenNo ratings yet
- Hdp301infectionrevisedoct2020 1Document24 pagesHdp301infectionrevisedoct2020 1Linda NguyenNo ratings yet
- Acid /base BalanceDocument10 pagesAcid /base BalanceLinda NguyenNo ratings yet
- Hdp301f&e Imbalancesf2020Document6 pagesHdp301f&e Imbalancesf2020Linda NguyenNo ratings yet
- Infection BacteriaandvirusesDocument3 pagesInfection BacteriaandvirusesLinda NguyenNo ratings yet