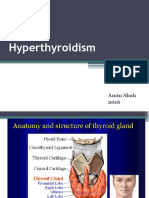
Hyperthyroidism
Hyperthyroidism
Download as pptx, pdf, or txt
You might also like
- Urinary System WorksheetDocument4 pagesUrinary System Worksheetayoonia75% (4)
- Peripheral Nervous SystemDocument1 pagePeripheral Nervous SystemChris_Barber09No ratings yet
- ThyrotoxicosisDocument105 pagesThyrotoxicosisAli Murtaza Abbas100% (1)
- Thyroid Function TestDocument28 pagesThyroid Function TestDhinesh Muthusamy100% (1)
- Thyroid Function TestDocument21 pagesThyroid Function TestPat JacintoNo ratings yet
- Thyroid Disorder: Meaza Bulbula (M. Pharm)Document61 pagesThyroid Disorder: Meaza Bulbula (M. Pharm)Ko MhdNo ratings yet
- Lec#15+16 Thyroid DisordersDocument82 pagesLec#15+16 Thyroid DisordersKhaldoun AlmomaniNo ratings yet
- PharmacotherapyDocument63 pagesPharmacotherapyNyahahahaNo ratings yet
- Hyperthyroid Is MDocument45 pagesHyperthyroid Is MThippagalla Harshitha HarshithaNo ratings yet
- Tutorial Presentation: Artika Mala (s170201) Week 2Document22 pagesTutorial Presentation: Artika Mala (s170201) Week 2Artika MalaNo ratings yet
- Hormone Assays: Immuno-Serology SectionDocument52 pagesHormone Assays: Immuno-Serology SectionjeffreyNo ratings yet
- Thyroid DiseaseDocument36 pagesThyroid Diseasejozemomo206No ratings yet
- Mbs127 Slide Hyperthyroidism 1Document46 pagesMbs127 Slide Hyperthyroidism 1revita262No ratings yet
- THYROIDDocument191 pagesTHYROIDTonie AbabonNo ratings yet
- Lecture (1) - THDocument34 pagesLecture (1) - THyoussef hossamNo ratings yet
- Lecture 17 - Thyroid Disorders (Including Struma and CA Thyroid) - Dr. M. Robikhul Ikhsan, SP - PD-KEMD (2021)Document21 pagesLecture 17 - Thyroid Disorders (Including Struma and CA Thyroid) - Dr. M. Robikhul Ikhsan, SP - PD-KEMD (2021)Ivan AditamaNo ratings yet
- Hypo Thyroid Is MDocument27 pagesHypo Thyroid Is Mdhiraj parmarNo ratings yet
- Hyperthyroid Is MDocument42 pagesHyperthyroid Is MkapilNo ratings yet
- Interpretation of Laboratory Thyroid Function Tests: The "Hidden" Health ProblemDocument38 pagesInterpretation of Laboratory Thyroid Function Tests: The "Hidden" Health Problemalanoud.877No ratings yet
- Sophie Keyte Bvms (Hons) Mvetmed (Dist) Fhea Dipacvim Mrcvs Sophie - Keyte@Bristol - Ac.UkDocument24 pagesSophie Keyte Bvms (Hons) Mvetmed (Dist) Fhea Dipacvim Mrcvs Sophie - Keyte@Bristol - Ac.UkStefana UrsuNo ratings yet
- Hyperthyroid 170715182805Document71 pagesHyperthyroid 170715182805Suryati HusinNo ratings yet
- Thyroid ReportDocument105 pagesThyroid ReportAARVNo ratings yet
- Thyroid DiseaseDocument72 pagesThyroid Diseaseluna zeidNo ratings yet
- Hyperthyroidism and HypothyroidismDocument59 pagesHyperthyroidism and HypothyroidismJun AmaroNo ratings yet
- Management of Thyroid DisordersDocument119 pagesManagement of Thyroid DisordersmatthiaspaullowNo ratings yet
- Hormones 20Document80 pagesHormones 20Stephanie Ortiz FonsecaNo ratings yet
- Lecture (2) TherapDocument25 pagesLecture (2) Therapyoussef hossamNo ratings yet
- 09 Thyroid Practice - v2Document23 pages09 Thyroid Practice - v2Shahriar honarmandNo ratings yet
- Hyper and HypothyroidismDocument63 pagesHyper and Hypothyroidismmeetgagiya2005No ratings yet
- #30 Thyroid and Thyroid TestingDocument25 pages#30 Thyroid and Thyroid TestingasclswisconsinNo ratings yet
- Thyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsDocument7 pagesThyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsPrincess Noreen SavellanoNo ratings yet
- Thyroid DiseasesDocument77 pagesThyroid DiseasesAllan MakalaNo ratings yet
- Thyroid DiseasesDocument44 pagesThyroid DiseasesPLDT HOMENo ratings yet
- Thyroid Gland DisordersDocument64 pagesThyroid Gland DisordersFaisal RavifNo ratings yet
- F1) P-Thyroid DisordersDocument9 pagesF1) P-Thyroid Disordersstella.gillesania.chenNo ratings yet
- DR Ananta Thyroid SlideDocument73 pagesDR Ananta Thyroid SlideRoshan Kumar PanditNo ratings yet
- Thyroid Function Test and Adrenal Function TestsDocument64 pagesThyroid Function Test and Adrenal Function TestsDr Abhinav Manish MDNo ratings yet
- Thyroid Gland Diseases in ChildrenDocument29 pagesThyroid Gland Diseases in ChildrenadinayNo ratings yet
- THYROTOXICOSISDocument20 pagesTHYROTOXICOSISfig8fashion1No ratings yet
- Hypothyroid in Pregnancy Andi CakraDocument32 pagesHypothyroid in Pregnancy Andi CakraCakraEkky100% (1)
- Thyroid Function Tests PPT of IMS BHUDocument74 pagesThyroid Function Tests PPT of IMS BHUPriyanshu Mandal100% (1)
- PATIENT WITH ENDOCRINE DYSFUNCTION THYROID .pptx1Document52 pagesPATIENT WITH ENDOCRINE DYSFUNCTION THYROID .pptx1sembakarani thevagumaranNo ratings yet
- HypothyroidismDocument59 pagesHypothyroidismAmir Mahmoud100% (1)
- HypertyroidismDocument46 pagesHypertyroidismenriNo ratings yet
- Thyroid Function Tests: Drneha Mahajan MD PathologyDocument71 pagesThyroid Function Tests: Drneha Mahajan MD PathologyMukesh Kumar ChaudharyNo ratings yet
- Thyroid Disease in PregnancyDocument67 pagesThyroid Disease in PregnancySiti Fatimah100% (2)
- Endocrinologic DisordersDocument80 pagesEndocrinologic Disordersfanuiel mandefroNo ratings yet
- HYPERTHYROIDISMDocument40 pagesHYPERTHYROIDISMEmmanuelNo ratings yet
- Thyroid DisordersDocument22 pagesThyroid DisordersNimer Abdelhadi AliNo ratings yet
- THyroid Function Test 123Document36 pagesTHyroid Function Test 123lenin coolNo ratings yet
- SC2 2015 HyperthyroidismDocument38 pagesSC2 2015 HyperthyroidismShafern TanNo ratings yet
- Thyroid Disorders: (Hyperthyroidism and Hypothyroidism)Document28 pagesThyroid Disorders: (Hyperthyroidism and Hypothyroidism)Mina RoxasNo ratings yet
- Hypothyroidism: Bagian Penyakit Dalam FK Uisu MedanDocument50 pagesHypothyroidism: Bagian Penyakit Dalam FK Uisu Medanindra saputraNo ratings yet
- Hyperthyroidism: A Practical Approach To Diagnosis and ManagementDocument70 pagesHyperthyroidism: A Practical Approach To Diagnosis and ManagementMutiara Manuella TambaNo ratings yet
- Thyroid Function TestsDocument29 pagesThyroid Function TestsAkwesaNo ratings yet
- Medical and Surgical Complications in Pregnancy: Ramon M. Gonzalez, MDDocument161 pagesMedical and Surgical Complications in Pregnancy: Ramon M. Gonzalez, MDaldeeray01No ratings yet
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamNo ratings yet
- Thyroid LectureDocument65 pagesThyroid LectureAndres TabaresNo ratings yet
- Thyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoDocument35 pagesThyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoNinaNo ratings yet
- Disorders of The Thyroid GandDocument167 pagesDisorders of The Thyroid GandWendy Figueroa MijaresNo ratings yet
- Medical and Surgical Complications PDFDocument206 pagesMedical and Surgical Complications PDFparmcparmcNo ratings yet
- Core CH 8 Transport in HumansDocument10 pagesCore CH 8 Transport in Humansommp100% (1)
- Learning Objectives:: Pathophysiology & Therapeutics, I (MSPR 521) Lecture No. 14Document9 pagesLearning Objectives:: Pathophysiology & Therapeutics, I (MSPR 521) Lecture No. 14adzhangNo ratings yet
- DR - Datis - Kharrazian Gut Bacteria TranscriptDocument35 pagesDR - Datis - Kharrazian Gut Bacteria TranscriptGreg Wolfe100% (4)
- Integumentary SystemDocument34 pagesIntegumentary SystemJerneth Nyka FloresNo ratings yet
- Human Body - Wikipedia PDFDocument18 pagesHuman Body - Wikipedia PDFMavura ZwideNo ratings yet
- Tumors of Nervous SystemDocument50 pagesTumors of Nervous SystemNininghrNo ratings yet
- Brain Anatomy ThesisDocument4 pagesBrain Anatomy Thesisbrittanyjonescolumbia100% (2)
- Chapter 79. Adrenal GlandsDocument42 pagesChapter 79. Adrenal GlandsJeremy IrvanNo ratings yet
- The PNF (Proprioceptive Neuromuscular Facilitation) Stretching Technique - A Brief ReviewDocument6 pagesThe PNF (Proprioceptive Neuromuscular Facilitation) Stretching Technique - A Brief ReviewDiane Troncoso Alegria0% (1)
- The Human Body in Art Education Presentation in Red Brown Hand Drawn Textured StyleDocument73 pagesThe Human Body in Art Education Presentation in Red Brown Hand Drawn Textured StyleMiangela lalaNo ratings yet
- Pag-Oring Nuevo National High SchoolDocument2 pagesPag-Oring Nuevo National High SchoolAlmiraMayAlvarezMarquezNo ratings yet
- NCM 106 Drugs Acting On Immune SystemDocument24 pagesNCM 106 Drugs Acting On Immune SystemLi mNo ratings yet
- The Endocrine SystemDocument41 pagesThe Endocrine SystemОксана КрасильниковаNo ratings yet
- Lymphoma Dr. Asad 13.7.2023Document181 pagesLymphoma Dr. Asad 13.7.2023Yousuf SawdagorNo ratings yet
- Reproductive SystemDocument7 pagesReproductive SystemRiaz siddiquiNo ratings yet
- Science Unit 1 7TH JDocument2 pagesScience Unit 1 7TH JHafiz Danish Rehman RanaNo ratings yet
- Gannguan PubertasDocument56 pagesGannguan PubertasAde Yosdi PutraNo ratings yet
- Anatomy & Physiology: Mrs. Tina Joy G. Mante, RN, MANDocument30 pagesAnatomy & Physiology: Mrs. Tina Joy G. Mante, RN, MANTina G. ManteNo ratings yet
- Learn The Anatomy of The HeartDocument2 pagesLearn The Anatomy of The Heartapi-534129744No ratings yet
- Assessment of Neurologic FunctionDocument63 pagesAssessment of Neurologic FunctionChombe JcNo ratings yet
- The Respiratory SystemDocument8 pagesThe Respiratory SystemDavid DanielNo ratings yet
- Paediatric Nephrology Syllabus FinalDocument13 pagesPaediatric Nephrology Syllabus FinalClever BarbieNo ratings yet
- Lymphatic SystemDocument5 pagesLymphatic SystemEmmanuel A. GalvanNo ratings yet
- Lymphatic System MCQDocument6 pagesLymphatic System MCQtarekhk05No ratings yet
- McqsDocument10 pagesMcqsDAWOODNo ratings yet
- Data Olahan Rawat Inap2014Document58 pagesData Olahan Rawat Inap2014daffa11No ratings yet
- Histopathology: Acute T-Cell Mediated Rejection: Anne Margarette Canapi, MDDocument75 pagesHistopathology: Acute T-Cell Mediated Rejection: Anne Margarette Canapi, MDAnneCanapiNo ratings yet
- Central Nervous System: The Spinal CordDocument30 pagesCentral Nervous System: The Spinal CordRO OMNo ratings yet