Abnormal Thyroid Function in Pregnancy
Abnormal Thyroid Function in Pregnancy
Download as pptx, pdf, or txt
You might also like
- Grabovoi - Codes For Various Types of Diesease Version 1-NUMBER SEQUENCE GGDocument39 pagesGrabovoi - Codes For Various Types of Diesease Version 1-NUMBER SEQUENCE GGManojkumar Nair93% (29)
- 1-Complete Blood Count - PO1106326185-399Document8 pages1-Complete Blood Count - PO1106326185-399Arup KumarNo ratings yet
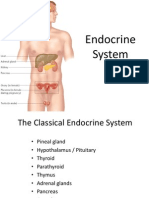
- Endocrine SystemDocument96 pagesEndocrine SystemSandhya Kakkar100% (4)
- Topic Presentation On Thyroid Disorders in PregnancyDocument31 pagesTopic Presentation On Thyroid Disorders in PregnancySairindri SahooNo ratings yet
- Hypothyroidism in PregnancyDocument14 pagesHypothyroidism in PregnancyShajia ZafarNo ratings yet
- Diagnosis of HypothyroidismDocument10 pagesDiagnosis of HypothyroidismHanzla IrfanNo ratings yet
- Thyroid Disease in PregnancyDocument53 pagesThyroid Disease in PregnancyTee Wei SianNo ratings yet
- Thyroid Disorders: A Practical ApproachDocument26 pagesThyroid Disorders: A Practical ApproachSadashivayya SoppimathNo ratings yet
- Hypothyroid in Pregnancy Andi CakraDocument32 pagesHypothyroid in Pregnancy Andi CakraCakraEkky100% (1)
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Document63 pagesClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaNo ratings yet
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocument48 pagesLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteNo ratings yet
- HMB Nice GuidelinesDocument192 pagesHMB Nice Guidelineschar1356No ratings yet
- National Guidelines For Screening of Hypothyroidism During PregnancyDocument48 pagesNational Guidelines For Screening of Hypothyroidism During PregnancyManish Chandra PrabhakarNo ratings yet
- FOGSI Focus Benefit Beyond ContraceptionDocument89 pagesFOGSI Focus Benefit Beyond ContraceptionG S SHEKHAWATNo ratings yet
- Thyroid DX PXLDocument62 pagesThyroid DX PXLabduljebarNo ratings yet
- TPO in PregnancyDocument18 pagesTPO in PregnancyRoxana TudorNo ratings yet
- Hyperthyroidsm: EpidemiologyDocument6 pagesHyperthyroidsm: EpidemiologyEllieNo ratings yet
- Thyroid GlandDocument49 pagesThyroid Glandjuliefe pinionNo ratings yet
- SPLIT TEE WELDING ProcedureDocument42 pagesSPLIT TEE WELDING ProcedureScribdTranslationsNo ratings yet
- Gds137 Slide HyperthyroidismDocument30 pagesGds137 Slide HyperthyroidismLouie Kem Anthony BabaranNo ratings yet
- Pemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKDocument12 pagesPemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKBonitavanyNo ratings yet
- Thyroid Function Test (TFT'S) : Presented By: Shoaib Ahmad Usama Maqsood Kamran AnjumDocument52 pagesThyroid Function Test (TFT'S) : Presented By: Shoaib Ahmad Usama Maqsood Kamran AnjumpriyaNo ratings yet
- ImmunisationDocument42 pagesImmunisationDr. Ajeta GuptaNo ratings yet
- Thyroid Tests and ResultsDocument9 pagesThyroid Tests and ResultsKristel BelgicaNo ratings yet
- The Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornDocument36 pagesThe Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornRahmayantiYuliaNo ratings yet
- Dermoid CystDocument13 pagesDermoid CystGaganaNo ratings yet
- Variations, Errors, and QualityDocument46 pagesVariations, Errors, and QualityJohn Reden RomeroNo ratings yet
- Thyroid and InfertilityDocument36 pagesThyroid and InfertilitySairindri SahooNo ratings yet
- RCOG Screening GuidelinesDocument10 pagesRCOG Screening GuidelinesJo FishburnNo ratings yet
- Thyroid Disorders (Final Draft)Document17 pagesThyroid Disorders (Final Draft)mogesie1995No ratings yet
- Endocrine 160110083024Document65 pagesEndocrine 160110083024Ryan CracknellNo ratings yet
- Preconceptional Care (Veena)Document44 pagesPreconceptional Care (Veena)Veena Madhuri100% (1)
- Guidelines of The American Thyroid Association PREGNANCY PDFDocument47 pagesGuidelines of The American Thyroid Association PREGNANCY PDFIqra AnugerahNo ratings yet
- CHN1 Health Care Delivery System2Document22 pagesCHN1 Health Care Delivery System2MicaNo ratings yet
- Primary Dysmenorrhea ConsensusDocument11 pagesPrimary Dysmenorrhea ConsensusNorman AjxNo ratings yet
- (OBS) 1.09 Pre-Conceptional Counselling & Prenatal Care - Bongala (Sep 8)Document16 pages(OBS) 1.09 Pre-Conceptional Counselling & Prenatal Care - Bongala (Sep 8)Noreen Hannah GabrielNo ratings yet
- Fogsi ChecklistDocument131 pagesFogsi ChecklistParimi VinodNo ratings yet
- FunctionTests Brochure PDFDocument2 pagesFunctionTests Brochure PDFArslan SaleemNo ratings yet
- Hormon GDSDocument23 pagesHormon GDSBRI KUNo ratings yet
- Hyperthyroidism in PregnancyDocument21 pagesHyperthyroidism in PregnancyCharisse Aser Flores AquinoNo ratings yet
- PITUITARYDocument37 pagesPITUITARYaparna shamaNo ratings yet
- Therapeutics: Thyroid DisordersDocument24 pagesTherapeutics: Thyroid DisordersSharas FarhadNo ratings yet
- Hyperprolactinem IaDocument63 pagesHyperprolactinem Iakhadzx100% (2)
- Prenatal Diagnosis and ScreeningDocument55 pagesPrenatal Diagnosis and ScreeningRania ZahoNo ratings yet
- 1-Good Health Gold Package - PO2257496339-951Document1 page1-Good Health Gold Package - PO2257496339-951Aafaq BhuttoNo ratings yet
- Dermoid Cyst: Jump To Navigation Jump To SearchDocument4 pagesDermoid Cyst: Jump To Navigation Jump To Searchfgfxgx100% (1)
- Goiter and Malignant Thyroid DiseaseDocument24 pagesGoiter and Malignant Thyroid Diseaseshaza ewisNo ratings yet
- PCOS Evidence-Based Guideline For Assessment and Management PcosDocument167 pagesPCOS Evidence-Based Guideline For Assessment and Management PcosJalajarani AridassNo ratings yet
- PreConception Care 4 Student VersionDocument38 pagesPreConception Care 4 Student VersionKajal SinghNo ratings yet
- Let's Talk About Thyroid PDFDocument92 pagesLet's Talk About Thyroid PDFEidi IdhamNo ratings yet
- Thyroid Disorders During PregnancyDocument25 pagesThyroid Disorders During PregnancyA.H.ANo ratings yet
- Pre-Conceptional Counselling and Pre-Conceptional Care2Document61 pagesPre-Conceptional Counselling and Pre-Conceptional Care2divyamathew100% (1)
- Thyroid StormDocument15 pagesThyroid Stormdr_arvindanNo ratings yet
- Thyroid Disorders in ElderlyDocument16 pagesThyroid Disorders in ElderlyYayatRuslanNo ratings yet
- VivaChek Company Introduction Updated Oct 2016 (En)Document16 pagesVivaChek Company Introduction Updated Oct 2016 (En)Malik AlnabhaniNo ratings yet
- Fertility: Assessment and Treatment For People With Fertility ProblemsDocument4 pagesFertility: Assessment and Treatment For People With Fertility ProblemsPatrick CoghlanNo ratings yet
- Recent Advances in Management of Fetal Growth DisordersDocument77 pagesRecent Advances in Management of Fetal Growth Disorderszaranahar100% (1)
- Assessment and Management of Women With Polycystic Ovary Syndrome (PCOS)Document17 pagesAssessment and Management of Women With Polycystic Ovary Syndrome (PCOS)Triratna FauziahNo ratings yet
- Thyroiddisease 190216062020Document42 pagesThyroiddisease 190216062020Manikandan Vp100% (1)
- Thyroid FunctionDocument12 pagesThyroid Functionسلطان القلح100% (1)
- Wedge Wire ScreensDocument6 pagesWedge Wire Screenscumpio425428No ratings yet
- Hyperthyroidism in PregnancyDocument29 pagesHyperthyroidism in PregnancyLavina JainNo ratings yet
- Thyroid Talk-FMD RdsDocument58 pagesThyroid Talk-FMD RdsSriman YarrarapuNo ratings yet
- CTG Interpretation 1Document27 pagesCTG Interpretation 1asri khazaliNo ratings yet
- Cme Anemia and Rhesus Disease O&gDocument84 pagesCme Anemia and Rhesus Disease O&gasri khazaliNo ratings yet
- Eech & Abnormal PresentationsDocument14 pagesEech & Abnormal Presentationsasri khazaliNo ratings yet
- Anatomy and Physiology of The EarDocument17 pagesAnatomy and Physiology of The Earasri khazaliNo ratings yet
- Congenital and Perinatal Cytomegalovirus Infection: Chun Soo Kim, M.D., PH.DDocument7 pagesCongenital and Perinatal Cytomegalovirus Infection: Chun Soo Kim, M.D., PH.Dasri khazaliNo ratings yet
- 2017 Guidelines of The American Thyroid Association For The Diagnosis and Management of Thyroid Disease During Pregnancy and The PostpartumDocument85 pages2017 Guidelines of The American Thyroid Association For The Diagnosis and Management of Thyroid Disease During Pregnancy and The Postpartumdiegoesteban1234No ratings yet
- Biochemistry of Hormones (Part 1)Document31 pagesBiochemistry of Hormones (Part 1)arun231187100% (2)
- Biochemistry University Questions and AnswersDocument80 pagesBiochemistry University Questions and AnswersPragadeesh ChakravarthyNo ratings yet
- HOMEOSTASIS - Lecture (Human Biology)Document22 pagesHOMEOSTASIS - Lecture (Human Biology)dokteraanNo ratings yet
- Corrected 1041 File Part 1Document160 pagesCorrected 1041 File Part 1walebayo06No ratings yet
- © Ncert Not To Be Republished: C C I C 22Document17 pages© Ncert Not To Be Republished: C C I C 22SatyarthShuklaNo ratings yet
- EEF467 Tutorial Sheet 1Document5 pagesEEF467 Tutorial Sheet 1NK-NGAMNo ratings yet
- 1 Endocrine System Review GuidemwDocument3 pages1 Endocrine System Review GuidemwdfgvsfdsfNo ratings yet
- Totalt4 ArcDocument6 pagesTotalt4 Arctesteste testeNo ratings yet
- Endocrine System Reviewer LecDocument3 pagesEndocrine System Reviewer LecMadelleNo ratings yet
- STUDY QUESTIONS Endocrine System 1 - DR P Kumar Biochem-GeneticsDocument24 pagesSTUDY QUESTIONS Endocrine System 1 - DR P Kumar Biochem-Geneticsteklay100% (1)
- Thyroid PathologyDocument9 pagesThyroid PathologyJordan FernandezNo ratings yet
- NIH Public Access: Author ManuscriptDocument11 pagesNIH Public Access: Author ManuscriptErika Lisseth Saldarriaga GonzálezNo ratings yet
- Haematology Complete Blood Count (CBC EXT) : 021808250310 MR - AJAY KUMAR 662326Document7 pagesHaematology Complete Blood Count (CBC EXT) : 021808250310 MR - AJAY KUMAR 662326ANSHU KUMAR RANANo ratings yet
- Chapter 5Document6 pagesChapter 5Shiny ChenNo ratings yet
- Control and Co-OrdinationDocument20 pagesControl and Co-OrdinationAnisha ThomasNo ratings yet
- Hypothyroidism DsDocument69 pagesHypothyroidism DsAS BravoNo ratings yet
- Physiology of PregnancyDocument56 pagesPhysiology of PregnancyMimah Garbosa100% (1)
- Yoga and Hyperthyroidism PDFDocument16 pagesYoga and Hyperthyroidism PDFRaushan Kumar MishraNo ratings yet
- Biology f4 NoteDocument68 pagesBiology f4 NoteE-SKUUL ACADEMYNo ratings yet
- 15th Week Minerals 2023Document40 pages15th Week Minerals 2023VizhiNo ratings yet
- AceDocument10 pagesAceConrad Ace PerezNo ratings yet
- Thyroid Storm - Mary L SchreiberDocument4 pagesThyroid Storm - Mary L Schreibervanny leutualyNo ratings yet
- Good Health Package PDFDocument8 pagesGood Health Package PDFRatan Swami SrivastavaNo ratings yet
- Blood ReportsDocument16 pagesBlood ReportsHafsa NawaazNo ratings yet
- Levothyroxine Interactions With Food and Dietary Supplements-A Systematic ReviewDocument20 pagesLevothyroxine Interactions With Food and Dietary Supplements-A Systematic Reviewalan_pedraza864No ratings yet
- HypothyridismDocument18 pagesHypothyridismanuu1404No ratings yet