Burn Management
Burn Management
Download as pptx, pdf, or txt
You might also like
- Incision & Drainage of Abscess Group 9 4bDocument5 pagesIncision & Drainage of Abscess Group 9 4bGUDISELA ramyaNo ratings yet
- Neonatal and Infant CareDocument10 pagesNeonatal and Infant CareCarla JimenezNo ratings yet
- Genaro Garcia Luna Bail ApplicationDocument10 pagesGenaro Garcia Luna Bail ApplicationAristegui NoticiasNo ratings yet
- Wound Care: WHO Surgical Care at The District Hospital 2003Document20 pagesWound Care: WHO Surgical Care at The District Hospital 2003Hero MondaresNo ratings yet
- Procedure For Dressing WoundsDocument5 pagesProcedure For Dressing WoundsAbegyl Nicole FiguraNo ratings yet
- Hypertonic SolutionsDocument4 pagesHypertonic SolutionsVanessa PaguiriganNo ratings yet
- Eczema: Starship Children's Health Clinical GuidelineDocument10 pagesEczema: Starship Children's Health Clinical GuidelineI Wayan Tri Sulaksana GiriNo ratings yet
- © 2021 Lippincott Advisor - Treatments - DebridementDocument5 pages© 2021 Lippincott Advisor - Treatments - DebridementJoyJoy Tabada CalunsagNo ratings yet
- A) General Principles of Wound Care B) Superficial To Mid-Dermal Burns C) Deep Burns Wound Conversion A) General Principles of Wound CareDocument29 pagesA) General Principles of Wound Care B) Superficial To Mid-Dermal Burns C) Deep Burns Wound Conversion A) General Principles of Wound CareTahseenNo ratings yet
- Basic Surgical and Anaesthetic Techniques.Document33 pagesBasic Surgical and Anaesthetic Techniques.jasperezra203No ratings yet
- Patient Education Sheet For Warts TreatmentDocument7 pagesPatient Education Sheet For Warts TreatmentHalim MaherNo ratings yet
- Scabies 2Document21 pagesScabies 2Valdi DwiramaNo ratings yet
- Lorma Burn First AidDocument35 pagesLorma Burn First Aidcyvaldez033094No ratings yet
- Integumentary Disorders (New)Document41 pagesIntegumentary Disorders (New)coosa liquorsNo ratings yet
- GF NOjb 3 GZDXSTD9 I 2 Ol TXAt L03 Z3 X 4 P4 Y2 Q2 Jbi DDocument9 pagesGF NOjb 3 GZDXSTD9 I 2 Ol TXAt L03 Z3 X 4 P4 Y2 Q2 Jbi DsharonchivingeNo ratings yet
- Wound CareDocument3 pagesWound CareMa Corazon MelecioNo ratings yet
- Open Wet Dressings DermatologyDocument3 pagesOpen Wet Dressings Dermatologygeorgeloto12No ratings yet
- Wound Care and Wound DressingDocument46 pagesWound Care and Wound DressingAj Macoto50% (2)
- Minor SurgeryDocument83 pagesMinor Surgerymmohammed seidNo ratings yet
- Emergencies & TBSA MergedDocument57 pagesEmergencies & TBSA MergedDanica FrancoNo ratings yet
- 418RLE-M3-SL2 Quick Assessment of TBSA and Fluid ReplacementDocument7 pages418RLE-M3-SL2 Quick Assessment of TBSA and Fluid ReplacementDanica FrancoNo ratings yet
- Skin Reaction StagesDocument2 pagesSkin Reaction Stagesdaney_0211No ratings yet
- Burn-Medical and Surgical ManagementDocument6 pagesBurn-Medical and Surgical ManagementCristina L. JaysonNo ratings yet
- Scabies Treatment ProphylaxisDocument4 pagesScabies Treatment Prophylaxisduch2020No ratings yet
- Anzym 1212Document1 pageAnzym 1212Mustafa ArarNo ratings yet
- Session20 Dermatological DisordersDocument53 pagesSession20 Dermatological Disordersmbelengo97No ratings yet
- ScabiesDocument14 pagesScabiesRohini SelvarajahNo ratings yet
- Scabies PresentationDocument15 pagesScabies Presentationrhimineecat71No ratings yet
- Derm Primary Care 2022Document111 pagesDerm Primary Care 2022FazrulNo ratings yet
- ScabiesDocument18 pagesScabiesRashidul IslamNo ratings yet
- الجرب مرشد علاجيDocument3 pagesالجرب مرشد علاجيyasinoNo ratings yet
- Nursing Aspect - Wound ManagementDocument54 pagesNursing Aspect - Wound ManagementBbieSyg Usagi Tsukino0% (1)
- ملف الصور الاهم - - -Document100 pagesملف الصور الاهم - - -mohamedeen hamzaNo ratings yet
- ABC of Burns First Aid and Treatment of Minor BurnsDocument3 pagesABC of Burns First Aid and Treatment of Minor BurnsDita DitotNo ratings yet
- Chapter 33 HygieneDocument14 pagesChapter 33 HygieneKathleen FrugalidadNo ratings yet
- Nursing Care of Children With BurnsDocument52 pagesNursing Care of Children With Burnskarpagamanbu100% (5)
- Maryville NURS 623 ExamDocument14 pagesMaryville NURS 623 ExamWizzardNo ratings yet
- Skin PrepDocument19 pagesSkin PrepANA DelafuenteNo ratings yet
- Iihq@: Dressing A Burn WoundDocument3 pagesIihq@: Dressing A Burn Woundshubham rathodNo ratings yet
- Fluid and Medication Spill ProtocolDocument6 pagesFluid and Medication Spill ProtocolScribdTranslationsNo ratings yet
- First Aid KitDocument20 pagesFirst Aid KitCruzCommodoreNo ratings yet
- Assessment of Skin Integrity: Nursing ProcessDocument17 pagesAssessment of Skin Integrity: Nursing ProcessCONEY CHING SAINo ratings yet
- BurnsDocument9 pagesBurnsVincentus BinNo ratings yet
- BurnsDocument77 pagesBurnsvinay7975741385No ratings yet
- Demonstration On Bed BathDocument8 pagesDemonstration On Bed Bathsujatamudi007No ratings yet
- Burn ManagementDocument7 pagesBurn ManagementnrhmhealthNo ratings yet
- Materi 9 SpectrofotometriDocument18 pagesMateri 9 Spectrofotometrirahma denia putriNo ratings yet
- Demonstration On Surgical DressingDocument7 pagesDemonstration On Surgical DressingM senNo ratings yet
- BURN Water SafetyDocument24 pagesBURN Water SafetyMary Clair BarbadilloNo ratings yet
- Management of Burn PDFDocument5 pagesManagement of Burn PDFaditiNo ratings yet
- C. Health Problems Common in ToddlerDocument72 pagesC. Health Problems Common in ToddlerRika MaeNo ratings yet
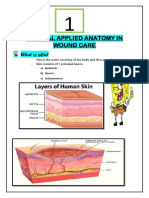
- Clinical Applied Anatomy in Wound CareDocument18 pagesClinical Applied Anatomy in Wound CareKlinik Komuniti Perwira100% (2)
- Initial Management:: First AidDocument6 pagesInitial Management:: First AidxerwaneNo ratings yet
- First Aid: Benito, Ira Serrano, EllyzaDocument40 pagesFirst Aid: Benito, Ira Serrano, EllyzaEllyza SerranoNo ratings yet
- UNIT 4 CP2-Basic Wound Care - Part 1Document60 pagesUNIT 4 CP2-Basic Wound Care - Part 1thembi MagagulaNo ratings yet
- Acid and Chemical BurnsDocument2 pagesAcid and Chemical BurnsًNo ratings yet
- Caring For A CastDocument39 pagesCaring For A CastGrape JuiceNo ratings yet
- Disastermanagguide PDFDocument56 pagesDisastermanagguide PDFNataraj ThambiNo ratings yet
- Standard Measures of Management of Infected WoundDocument11 pagesStandard Measures of Management of Infected WoundMohamed FarahatNo ratings yet
- Survival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)From EverandSurvival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)No ratings yet
- PDF Sex Matters How Male Centric Medicine Endangers Womens Health and What We Can Do About It 2Nd Edition Alyson J Mcgregor Ebook Full ChapterDocument54 pagesPDF Sex Matters How Male Centric Medicine Endangers Womens Health and What We Can Do About It 2Nd Edition Alyson J Mcgregor Ebook Full Chapterdaisy.noble43275% (4)
- Aspirin (Acetyl-Salicylic Acid) Drug MonographDocument1 pageAspirin (Acetyl-Salicylic Acid) Drug MonographMuhammad Arsalan100% (1)
- Ventilasi MekanikDocument47 pagesVentilasi MekanikzahrahNo ratings yet
- EballaststoffeDocument12 pagesEballaststoffePhan VanduNo ratings yet
- PSY709 Module Handbook PDFDocument40 pagesPSY709 Module Handbook PDFFilipe BoilerNo ratings yet
- Management of Chylothorax: By: Muhammad Aris Furqon Mentor: Muhammad Arza PutraDocument25 pagesManagement of Chylothorax: By: Muhammad Aris Furqon Mentor: Muhammad Arza PutraMuhammad Aris FurqonNo ratings yet
- 296 1179 1 PBDocument2 pages296 1179 1 PBKriti KumariNo ratings yet
- Ncma 217 ReviewerDocument3 pagesNcma 217 ReviewerJared Dela cruzNo ratings yet
- Real Ielts Exam T.Me/Ieltsc1: Section 4Document5 pagesReal Ielts Exam T.Me/Ieltsc1: Section 4muhammad bilalNo ratings yet
- Botox LeafletDocument1 pageBotox LeafleteidwisamNo ratings yet
- Tamoxifen PDFDocument5 pagesTamoxifen PDFErza GenatrikaNo ratings yet
- Dissertation Herbal MedicineDocument5 pagesDissertation Herbal MedicineBestOnlinePaperWritingServiceUK100% (1)
- L 8 Listening - Question Paper PDFDocument10 pagesL 8 Listening - Question Paper PDFVipin VargheseNo ratings yet
- TEST UNIT 9 Lop11Document5 pagesTEST UNIT 9 Lop11Hạnh HuỳnhNo ratings yet
- Bo 20 de on Thi Tot Nghiep 2021 Tieng Anh Bam Sat de Minh Hoa Co Dap an Đã Chuyển ĐổiDocument112 pagesBo 20 de on Thi Tot Nghiep 2021 Tieng Anh Bam Sat de Minh Hoa Co Dap an Đã Chuyển ĐổiThanh ThanhNo ratings yet
- Abnormalpuerperium 190328060723 1Document126 pagesAbnormalpuerperium 190328060723 1Preeti ChouhanNo ratings yet
- HEALTH6 Q2 Mod2 LivinginaHealthySchoolandCommunity V4Document18 pagesHEALTH6 Q2 Mod2 LivinginaHealthySchoolandCommunity V4toores.annemNo ratings yet
- NCP&SOAPIEDocument4 pagesNCP&SOAPIEMica OmotsosircNo ratings yet
- Cholecystitis - Complications of Cholecystitis A Comprehensive Contemporary Imaging ReviewDocument17 pagesCholecystitis - Complications of Cholecystitis A Comprehensive Contemporary Imaging ReviewSamuel WidjajaNo ratings yet
- Prudential PruPersonal AccidentDocument13 pagesPrudential PruPersonal AccidentpriscillasooNo ratings yet
- Pronation TherapyDocument26 pagesPronation TherapyydtrgnNo ratings yet
- Final Grant Proposal Marisa TestaDocument33 pagesFinal Grant Proposal Marisa Testaapi-546990429No ratings yet
- Use of Anesthesia in Pediatric Dentistry: A Cross Sectional SurveyDocument5 pagesUse of Anesthesia in Pediatric Dentistry: A Cross Sectional SurveyYenni ZulkifliNo ratings yet
- Bending The Trends To Promote Health and Well-Being: A Strategic Foresight On The Future of Health PromotionDocument32 pagesBending The Trends To Promote Health and Well-Being: A Strategic Foresight On The Future of Health PromotionLaura LizarazoNo ratings yet
- NCM 114 Care of Older AdultsDocument47 pagesNCM 114 Care of Older Adultsbrilliant dumayNo ratings yet
- Jadual Kuliah Tahun 2 Semester 1 Sesi 2022-2023Document24 pagesJadual Kuliah Tahun 2 Semester 1 Sesi 2022-2023Yusni RahimNo ratings yet
- LWW Bates 05 General Survey Transcript FinalDocument8 pagesLWW Bates 05 General Survey Transcript FinalSaeidreza SardariNo ratings yet
- Top 200 DrugsDocument4 pagesTop 200 DrugsEsther AhnNo ratings yet
- NATIONALDocument25 pagesNATIONALManisha raiNo ratings yet